
Abstract
The superior mesenteric artery syndrome also known as Wilkie’s syndrome or Benign duodenal stasis, is a condition that occurs when the third duodenum is compressed between the superior mesenteric artery anteriorly and the abdominal aorta posteriorly following the disappearance of the perivascular fatty tissue. It can emulate the symptoms of an upper abdominal obstruction. This case involves a 9-year-old female patient experiencing food vomiting that did not improve with medication. Radiological work-up, which included an abdominal X-ray and a CT angiography, led to the diagnosis of extrinsic and incomplete obstruction of the third duodenum by the aorto-mesenteric clamp. Unfortunately, this diagnosis is rarely made. The purpose of this article is to provide a review of the etiology, clinical presentation, and imaging findings of this syndrome.
Introduction
The superior mesenteric artery (SMA) syndrome is the result of compression of the third duodenum by a vascular clamp formed by the SMA and the aorta after disappearance of perivascular fatty tissue, which then causes the angle between the vessels to narrow. 1 First described by Austrian professor Carl Von Rokitansky in 1861 and later detailed by Wilkie in 1927, SMA incidence has been estimated at 0.1% to 0.3% and a typical age range of 10 to 39 years old, it preferentially affects young female adults and adolescents. Additionally, no racial or ethnic predisposition has yet been identified. 2 Despite the benign nature of SMA syndrome, if its symptoms are severe and its treatment is inadequate, it could be fatal. 3 Patients who have SMA syndrome typically exhibit hazy bowel obstruction symptoms. Typically recurrent nausea and vomiting are the most frequently reported clinical symptoms. The diagnosis of SMA syndrome can be challenging as its symptoms can mimic other gastrointestinal disorders. However, various imaging modalities are used to help in the early recognition of this condition, and prompt treatment can prevent the morbidity and mortality, making it crucial for clinicians to have a high index of suspicion for this syndrome in patients presenting with non-specific symptoms of small bowel obstruction. 4 We present a clinical case of this condition in a 9 years old female. We diagnosed it through the evaluation of clinical features and abdominal CT. A brief review of the related literatures will be reviewed through this article.
Case Presentation
A 9-year-old female patient from a non-consanguineous marriage, was being treated for depressive syndrome, currently under antidepressants,presented with persistent weight-bearing epigastralgia for 6 months before unprovoked late postprandial vomiting alleviate her symptoms. There were no gas, no bleeding in the stomach, and no cessation of feces were present in this patient. Her clinical examination revealed an abdominal mass, dullness, dehydrated skin folds without impaction, and an otherwise normal somatic examination. Considering the clinical picture, the proximal duodenum and dilated stomach are visible on an abdominal X-ray. A CT scan of the abdomen with contrast revealed a stenosis of the second part of the duodenum, along with a narrowed aorto-mesenteric space and a 15.8° aortomesenteric angle (lines). The aortomesenteric gap is 2.7 mm wide (Figure 1). The management included 20 days of oral and then parenteral nutrition based on postural treatment in left lateral decubitus. An uncomplicated surgical bypass (gastro-entero-anastomosis) was carried out because the patient’s condition did not improve despite medical treatment. Feeding was on day 3 after surgery resumed and the patient has been released on day 7 with only minor postoperative side effects and improved clinical outcomes at 4 months.
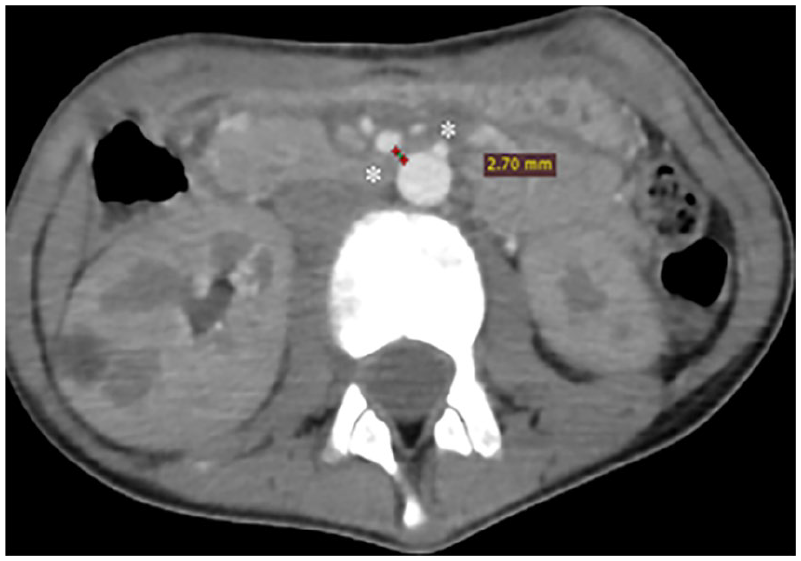
Axial contrast CT scan shows short aorta-SMA distance (2.7 mm) at level of duodenum (asterisk) after inserting a nasogastric tube.
Discussion
Superior mesenteric artery (SMA) syndrome is a misdiagnosed condition defined as compression of the third portion of the duodenum between the abdominal aorta and the superior mesenteric artery. 5 First described by Austrian professor Carl Von Rokitansky in 1861 and later detailed by Wilkie in 1927, SMA incidence has been estimated at 0.1% to 0.3% and a typical age range of 10 to 39 years old, it preferentially affects young female adults and adolescents. Additionally, no racial or ethnic predisposition has yet been identified. 6 Because the disease is uncommon and has vague symptoms, it can be difficult to distinguish from other anatomical or motility-related causes of duodenal obstruction.
The onset may be acute or may progress insidiously depending on the etiology and the extent of duodenal obstruction. In our patient, the assessment of rapid weight loss was subjective, although at the time of the examination, the patient had a critically low body mass index.
Ultrasound is a valuable tool for early detection of reduced aorto-mesenteric angle in patients with unexplained abdominal pain to suspect SMA syndrome. It can also show the short distance and the narrow angle between the aorta and SMA. It is a rapid, reproducible and non-invasive diagnostic test. However, it depends mainly on the patient’s condition, the operator’s experience, and the specifications of the ultrasound machine. 7
Additionally, abdominal CT with contrast injection and multiplanar reconstructions is a very useful noninvasive diagnostic technique that provides good vascular anatomic detail and allows accurate measurement of the aorto-mesenteric angle and distance to the third duodenal portion. The 2 main signs of this disease are an aortomesenteric angle of less than 22° with a sensitivity of 42.8% and a specificity of 100%, and an aortomesenteric distance of less than 8 mm with a sensitivity and specificity of 100%, 8 as observed in our patient. Normal aortomesenteric distance is usually between 10 and 28 mm. A normal aortomesenteric angle has been described as between 38° and 56°. 9 Associated radiological signs include a dilated stomach and duodenum to the aortomesenteric space, followed by an area of caliber disparity as the duodenum passes below the superior mesenteric artery. Sagittal reconstruction oriented obliquely (Figure 2) along the axis of the SMA provides more accurate measurements. 8

Obliquely oriented sagittal reconstruction of superior mesenteric artery (SMA) showing a aortomesenteric angle of 15.8°.
Although the barium study of the upper gastrointestinal tract has been used for the diagnosis of this syndrome, the radiological findings of this examination are often nonspecific and the advent of multiplanar computed tomography has played an important role in its diagnosis.
The clinical findings usually pose the problem of differential diagnosis with other pathologies such as pancreatitis, ulcer, megaduodenum, and eating disorders. 1 The interpretation of clinical symptoms and signs along with a clinical suspicion and radiological examinations are the key components in making the diagnosis of SMA syndrome.
The management of this syndrome is initially conservative, especially in the acute context. The objective of this treatment is to empty the stomach and duodenum and to provide enteral feeding, by placing a nasogastric tube and administering a high-calorie liquid diet hoping to restore a normal aortomesenteric distance and relieve the obstruction. If conservative treatment fails in a patient with severe symptoms, surgery is indicated; the first choice is open duodeno-jejunostomy, with good operative results in 79% to 100% of cases. 1 Given the possibility of marginal ulceration during the latter procedure, a vagotomy should be taken into account. It has also been successful to transpose the third segment of the duodenum anteriorly to the superior mesenteric vessels, which aims to permanently bypass the obstruction. 10
Conclusion
The Superior mesenteric artery (SMA) syndrome is a benign condition that can have serious consequences if managed late. Therefore, it should be brought up to radiologists and clinicians’ knowledge to make them very vigilant in detecting it, and to describe the role of multidetector CT angiography in its diagnosis by presenting the imaging findings of this syndrome.
Footnotes
Author Contributions
I would like to express my gratitude to my professors and all the colleagues who participated in the completion of this work.
Ethical Approval and Informed Consent
Written informed consent was obtained from a legally authorized representative for anonymized patient information to be published in this article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Guarantor of Submission
The corresponding author is the guarantor of submission.