
Abstract
The brown tumor is a non-neoplastic lesion resulting from an abnormality in bone metabolism in the context of primary, secondary, or tertiary hyperparathyroidism. They can affect any bone structure and be single or multiple. They are usually located on the long bones, pelvis, ribs, and collarbones. Facial localization is rare and is found in only 4.5% of brown tumors dominated by mandibular involvement. The treatment of a brown tumor depends on several elements: etiology, location, and symptomatology. It can regress or disappear after the treatment of hyperparathyroidism, thus avoiding surgical removal. Otherwise, excision of this mass is performed. We illustrate through this case a brown mandibular tumor revealing secondary hyperparathyroidism in a patient with a history of end-stage chronic renal failure on hemodialysis and associated neurofibromatosis type 1.
Introduction
A brown tumor is a benign focal bone lesion caused by localized and rapid osteoclastic turnover of bone, resulting from the direct effects of chronic excess parathormone (PTH), 1 it is more common in tertiary than in primary and secondary HPT and more likely with associated severe vitamin D deficiency.1-3 They can affect any bone structure and be single or multiple. They are generally located on the long bones, pelvis, ribs, and collarbones. Facial location is rare and is found in only 4.5% of brown tumors dominated by mandibular involvement.
We illustrate through this case a mandibular brown tumor revealing secondary hyperparathyroidism in a patient with a history of end-stage chronic renal failure on hemodialysis and associated neurofibromatosis type 1.
Case Report
A 14-year-old child with a history of neurofibromatosis type 1, end-stage chronic renal failure on hemodialysis, currently presents with mandibular swelling that had been increasing in size for 6 months.
On clinical examination, the child presents with scoliosis associated with café-au-lait spots, and a slight deformation of the lower limbs. (Figure 1) with a general deterioration in health. A computed tomography facial scan was requested to characterize the swelling and search for other locations

(A) Posterior view of the child showing scoliosis (green arrow); (B) Anterior view of the child showing café-au-lait spots on the entire abdomen and chest (red arrow).
A computed tomography facial scan revealed an osteolytic lesional process of the mandibular body lateralized on the left, well limited, with regular contours, multilocular, blowing the cortical bone which is laminated, not enhancing, without cortical lysis, nor periosteal reaction in gaze, pushing back the dental roots (Figure 2).
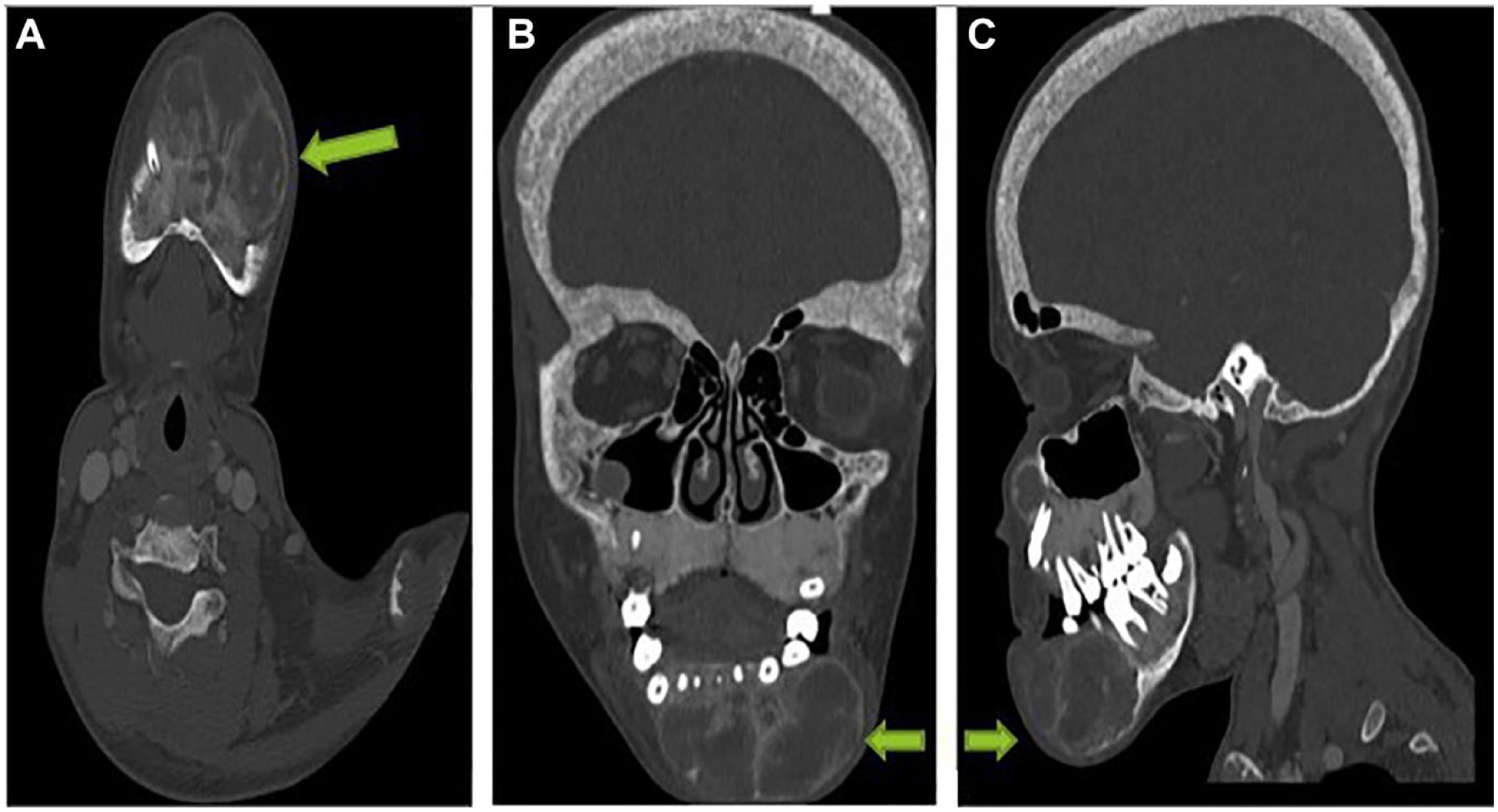
CT facial (A: Axial section, B: Coronal reconstruction, C: Sagittal reconstruction) revealed an osteolytic lesion involving the left mandibular body, well circumscribed, with regular contours, multilocular, expanding the cortical bone, non-enhancing, and without cortical lysis.
It is associated with a second lesional process at the level of the upper left alveolar process, having the same characteristics (Figure 3)

CT facial (A: Coronal reconstruction, B: Axial section) revealed an osteolytic lesion involving the upper left alveolar process, having same characteristic.
Thickening of the cranial vault and all the bones of the facial bones with a pepper and salt appearance (Figure 4).

CT facial axial section showing thickening of the cranial vault (A) and all the bones of the face (B) with a salt and pepper appearance.
Multiple lacunar foci of osteolysis of the cranial vault, the spinous processes of the cervical spine and the left clavicle (Figure 5).
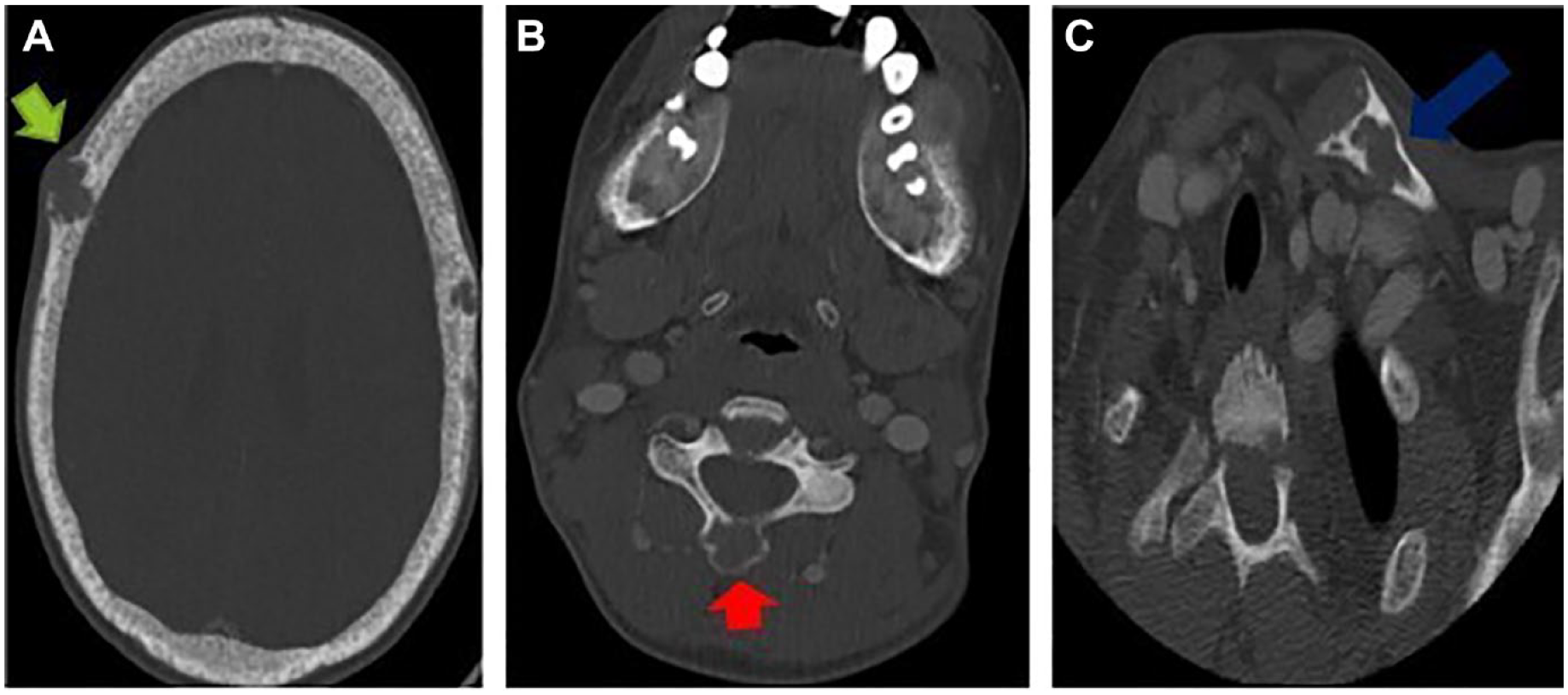
CT facial axial section showing a multiple lacunar foci of osteolysis involving vault (A: green arrow), the spinous processes of the cervical spine (B: red arrow), and the left clavicle (C: blue arrow).
Given the context of chronic renal insufficiency and the appearance on the scanner, a brown tumor was mentioned as part of secondary hyperparathyroidism with a low probability of fibro-cystic dysplasia, a parathormone assay is then requested and which came back greatly increased (2050 pg/mL; normal range 12-72 pg/mL), the biological assessment also showed a serum calcium level of 9 mg/dL (normal range, 8.8-11 mg/dL), phosphorus: 4 mg/dL (normal range, 2.5-5 .0 mg/dL), alkaline phosphatase: 1560 IU/L (normal range, 65-300 IU/L), and a 25-hydroxyvitamin D level of 18 μg/L (normal range: >20 μg/L)
The child received medical treatment (calicimimetics and vitamin D) to reduce the parathormone level and for the disappearance of the lesion, but the evolution is marked by the persistence of the brown tumor and the alteration of the general condition currently making surgical intervention impossible.
Discussion
The brown tumor is one of the clinical manifestations of hyperparathyroidism whether primary, secondary, or tertiary, it can affect any bone structure and be single or multiple. They are generally located on the long bones, pelvis, ribs, and collarbones. 1
When they develop in the facial region, the most affected bone is the mandibular bone. 2
Clinically, it is most often asymptomatic and the discovery is then fortuitous during the radiological examination, 4 or most often appears in the form of a more or less soft swelling.
Nowadays, with the improvement of exploration techniques and the early detection of hyperparathyroidism, brown tumors are becoming rare.
Early diagnosis of primary hyperparathyroidism is due to extensive use of biochemical screening in recent decades, which has made brown tumor a rare manifestation of primary hyperparathyroidism. 5
It is rare to diagnose a brown tumor before the first systemic signs of primary hyperparathyroidism, In return, the number of patients on hemodialysis having increased considerably, as well as their longevity, due to the improvement of techniques, has resulted in a much greater number of brown tumors due to secondary hyperparathyroidism. 5
On computed tomography scan, brown tumors appear as lytic lesions, more often multilocular, well limited, with scalloped outlines, which can thin the cortex or even interrupt it. 6
The radiological differential diagnosis between a brown tumor and other giant cell tumors is not simple, but generally, true giant cell tumors are more locally destructive than brown tumors, and their radiological appearance is more irregular. 7
Biopsy of the lesion is not necessary in the case where the patient presents with chronic renal failure, since the clinical history of secondary hyperparathyroidism usually establishes the diagnosis. In primary hyperparathyroidism, there is a need for a biopsy, especially because the brown tumor could be the first manifestation of the disease. 8
In this case it is characterized by a non-neoplastic reaction tissue made up of multinucleated giant osteoclastic cells, fibroblasts, bone microfractures, and hemorrhages with deposits of hemosiderin which give the lesion at the macroscopic level its characteristic brown color from which son name brown tumor. 7
Concerning the treatment of brown tumors, the resolution of the hyperparathyroidism is essential in order to hope for a resorption of the mass and if necessary to carry out an excision of this mass. 9 To do this, total or subtotal parathyroidectomy is indicated in particular in the event of parathyroid hyperplasia or adenoma depending on the number of affected glands .
For lesions due to secondary hyperparathyroidism, the treatment is mainly medical.10,11 It consists of reducing parathyroid hormone levels and therefore controlling the phosphocalcic balance. 11 Calcium carbonates, vitamin D, and calcimimetics can be used for medical treatment, 10 if necessary perform excision of this mass
Conclusion
A brown tumor is a benign focal bone lesion caused by localized and rapid osteoclastic turnover of bone, resulting from the direct effects of chronic excess parathormone (PTH). It presents particular radiological and histological characteristics allowing the establishment of the diagnosis and its management.
It can affect any bone structure, involvement of the facial region is rare
The resolution of the hyperparathyroidism is essential in order to hope for resorption of the mass and, if necessary, perform an excision of this mass.
Footnotes
Author Contributions
BK: contributed to conception and design; contributed to acquisition, analysis, and interpretation; drafted manuscript; critically revised manuscript; gave final approval; agrees to be accountable for all aspects of work ensuring itegrity and accuracy. BB: contributed to conception and design; contributed to acquisition, analysis, and interpretation; drafted manuscript; gave final approval; agrees to be accountable for all aspects of work ensuring itegrity and accuracy. SO: contributed to conception and design; contributed to acquisition, analysis, and interpretation; drafted manuscript; gave final approval; agrees to be accountable for all aspects of work ensuring itegrity and accuracy. SEH: contributed to acquisition, analysis, and interpretation; critically revised manuscript; gave final approval; agrees to be accountable for all aspects of work ensuring itegrity and accuracy. NA: contributed to acquisition, analysis, and interpretation; critically revised manuscript; gave final approval; agrees to be accountable for all aspects of work ensuring itegrity and accuracy. LC: contributed to acquisition, analysis, and interpretation; critically revised manuscript; gave final approval; agrees to be accountable for all aspects of work ensuring itegrity and accuracy.All authors contributed equally to this work.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
No ethical approval is required for de-identified single case reports based on our institutional policies.
Informed Consent
Written informed consent was obtained from a legally authorized representative.