
Abstract
Hydatid cyst disease is a health problem in some developing countries occurring in groups with permanent contact with dogs. It is a parasitic disease caused by Echinococcus Granulosus. The liver is the most common organ infected. If not treated appropriately; it may lead to developing life-threatening complications. Its rupture into bile ducts is the most frequent one, while hepatopulmonary fistula is a rare complication. We discuss the case of a child presenting those 2 complications as we emphasize the importance of early diagnosis and the role of the radiologist.
Introduction
Hepatic hydatid cyst is a common pathology caused by Echinococcus tapeworm. Cystic echinococcosis has a worldwide geographical distribution within the Mediterranean basin being an important endemic area. It is usually an asymptomatic disease that may get complicated with the formation of cysto-biliary communication (CBC), rupture into the peritoneal cavity, and bronchi. 1 The former is the most frequent one, while the latter is a rare complication. Imaging can help in diagnosing hepatic hydatid cysts due to their typical radiological findings. However, if the cyst is infected, no classical imaging signs may exist. In this case, serology can confirm the diagnosis since it’s usually positive. Our aim is to emphasize the importance of early diagnosis of this common pathology in developing countries especially in pediatric population.
Case Report
We report the case of a 7-year-old boy living in a village who had permanent contact with dogs. He presented to the emergency department 6 months ago with abdominal pain. Clinical examination was poor with only abdominal sensibility present in the right hypochondrium. Ultrasound and computed tomography (CT-scan) discovered 2 well-defined cystic masses within the liver with a positive hydatid serology. We concluded to hepatic hydatid cysts and the patient was put on medical treatment. Unfortunately, the patient had bad compliance due to poor social conditions, and came back 2 months later to the emergency department with jaundice, a chronic cough, and bile-stained sputum. Clinical examination found a jaundiced child with no fever but a diffuse sensibility of the abdomen. He had a respiratory rate of 17 breaths per minute and a normal level of oxygen. No other abnormalities were found. His blood count showed a hypereosinophily and his liver function test revealed an elevation (224 IU/L) of alkaline phosphatase (ALP) and an elevated bilirubin level of 2.2 mg/dL. Hydatid serology was also positive. C-reactive protein and white blood cells were normal. CT-scan showed multiple hepatic thick-walled cystic masses, enhanced peripherally after intravenous (IV) contrast located within (Figures 1 and 2):
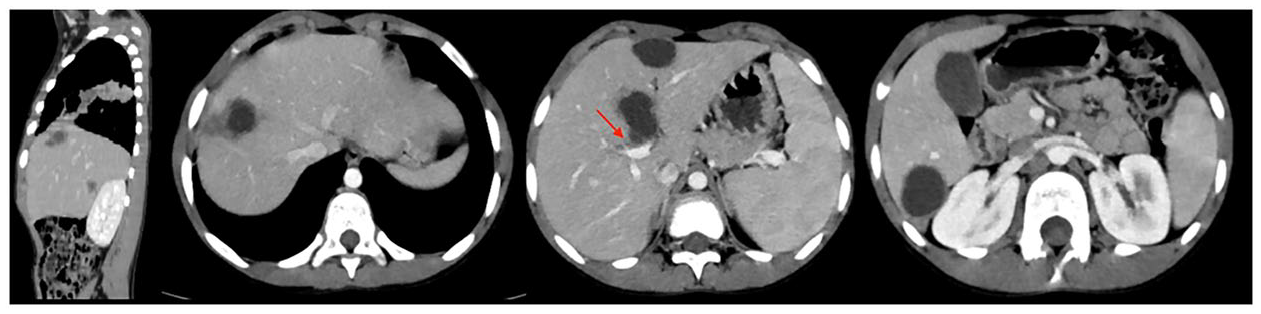
Axial planes and coronal reconstruction of an abdominal CT-SCAN with IV contrast showing multiple hydatid cysts: some with well-defined contours and others with irregular wall and peripheral enhancement. Note (red arrow) the interruption of the cyst wall adjacent to a bile duct suggesting cystobiliary communication.
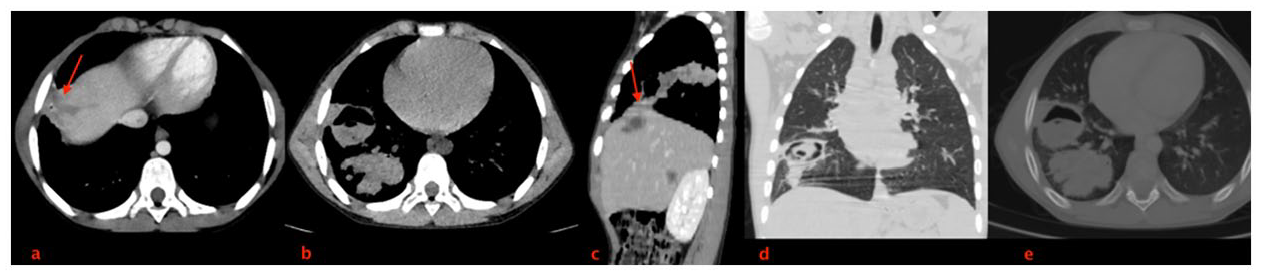
Thoraco-abdominal CT-SCAN with IV contrast: axial planes (a and b) and coronal reconstruction (c) showing the communication between the liver cyst and the intra-pulmonary masses (right inferior lobe) with irregular walls and gas-filled. Coronal (d) and axial (e) lung window showing the gas-filled masses, adjacent consolidation and an atelectatic band.
At the thoracic level, the scan showed 2 intra-parenchymal masses of the right inferior lobe, with a thin wall, not enhanced after IV contrast, surrounded by foci of condensation, sitting in the antero-basal segment, containing a hydro-aeric level and the right Fowler, gas-filled and coming into contact with the pleura. We concluded to multiple hepatic hydatid cysts with cysto-biliary communication and broncho-biliary fistula. The patient was put on Albendazole for 15 days for sterilization of the cyst and was due for a follow up consultation so that he can be scheduled for surgery. Unfortunately, he did not return for his follow up and we lost contact with him.
Discussion
Hydatid disease is caused by a parasite called Echinococcus Granulosus. Any body cavity, organ, or tissue can get infected. The cyst can cause pressure on the adjacent parenchyma and may rupture inside the biliary tree or develop a hepato-pulmonary fistula. 2 There are frequently a variety of symptoms and indicators present before a fistula forms. It can cause gastrointestinal pain, jaundice from a biliary obstruction, or respiratory difficulty. Patients typically exhibit fever, pain in the right upper abdomen, chest pain, jaundice, and sputum that is bile-colored. 3 The attentive clinician should nevertheless have a high index of suspicion when treating illnesses like right basal pneumonia or an infection of the biliary tree that could mask an underlying, developing fistulous disease. Once the fistula has developed, sepsis is typically present in the patient. There may be times when the patient coughs up bile-containing fluids or thick, purulent material. 4 This may also be accompanied by fever and weight loss, resembling other long-term diseases like tuberculosis or lung cancer. 2
Imaging is based on CT-SCAN and may show a fluid-density cyst. Frequently, there may be peripheral focal areas of calcification, which means no active infection (if completely circumferential). It may also visualize septa and daughter cysts.
A detached endocyst shows a floating, undulating membrane within the cyst, which gives the “water-lily sign.” We should note that the fluid is usually of variable attenuation, depending on the amount of proteinaceous debris. Imaging may also show a common complication which is intra-biliary rupture of hepatic hydatid cysts. Its radiological features can be classified into direct and indirect signs. Direct signs are mainly direct visualizations of cystobiliary communication. Indirect signs include a break in the cyst wall adjacent to a bile duct, biliary tree dilatation, cystic material within the biliary tree or gallbladder, and a distorted shape of the cyst (which represents a reduced intracystic pressure secondary to rupture). Other signs are the presence of gas-fluid or fat-fluid levels within the cyst and the beak-like projection of the cyst wall.
Intrathoracic rupture of hepatic hydatid cyst is a rare complication with several factors explaining it such as the negative intrathoracic pressure. The latter tends to aspirate the hepatic hydatid cyst. The other factor are mechanical compression by the cyst on the diaphragm leading to muscle erosion and muscle necrosis due to the cyst’s infection. 5 On the other hand, in the case of biliary fistulas, which typically affect young people due to the long-term evolution of a hydatid cyst of the hepatic dome, the caustic feature of the bile can induce a chemical erosion of the diaphragm, lung, and pleura.6,7 The pulmonary parenchyma will be damaged by the caustic action of this bile on the lung and bronchial tree, resulting in conditions ranging from simple hydatid pneumonia to the development of a cave. 6 Generally, it is a multiple or solitary cystic lesion of 1 to 20 cm in diameter. It is predominantly found in the lower lobes and can be unilateral or bilateral.
Uncomplicated cysts are well-defined, round or oval masses, enhancing after contrast injection with a hypodense content relative to the capsule, while complicated cysts may show meniscus sign or air crescent sign, cumbo sign or onion peel sign and consolidation adjacent to the cyst (ruptured cyst). 8
Surgery in pediatric population must be conservative. In non-complicated patients with less severe fistulas, noninvasive techniques such as cholangiopancreatography (MRCP), endoscopic retrograde cholangiopancreatography (ERCP) and percutaneous transhepatic cholangiography (PTCD) are preferable over traditional surgical techniques. 9 Frequently, the pulmonary lesions caused by hepatic hydatid disease are minimal and situated in the lower or middle pulmonary lobes. 5 This explains why doctors only use an abdominal approach to treat thoracic-involved hepatic hydatid cysts. When the hydatid disease is widely distributed or a complete resection of cysts is not feasible, medical adjuvant treatment is required. 7 In endemic areas, prophylactic measures should always be taken. The death and recurrence rates of this condition are significant despite advancements in detection and therapy approaches.
Conclusion
The incidence of hydatid disease in children increase with age and most frequently lungs and liver are involved. Hepatic hydatid cysts can have serious complications and its intrathoracic rupture is one that remains rare even in children. Early detection and initial treatment of hydatid illness are necessary for preventing this disease.
Footnotes
Acknowledgements
I would like to express my gratitude to my professors and all the colleagues who participated in the completion of this work.
Author Contributions
ELY: Contributed to conception and design; Contributed to analysis; Drafted the manuscript; Gave final approval; Agrees to be accountable for all aspects of work ensuring integrity and accuracy. CF : Contributed to conception and design; Contributed to analysis; Agrees to be accountable for all aspects of work ensuring integrity and accuracy. BN: Critically revised the manuscript; Gave final approval; Agrees to be accountable for all aspects of work ensuring integrity and accuracy. NA and LC: critically revised the manuscript; Gave final approval; Agrees to be accountable for all aspects of work ensuring integrity and accuracy. SEL: Contributed to acquisition, analysis, or interpretation; Critically revised the manuscript; Gave final approval.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed Consent
Written informed consent was obtained from the parents of patients for the publication of this case report.
Ethical Approval
Our institution does not require ethical approval for reporting individual cases or case series.
Guarantor of Submission
The corresponding author is the guarantor of submission