
Abstract
Congenital facial palsy is a rare condition that can be categorized into traumatic and developmental etiologies. Trauma related congenital facial palsy represents by far the most frequent cause with a spontaneous complete recovery within weeks, contrary to developmental causes that can be syndromic or non-syndromic, and have a poor prognosis. We present the case of an 11-month-old boy who suffers a congenital facial palsy. He undergoes an MRI examination with the adapted sequences to assess the facial nerve, and a high-resolution CT scan that reveals a seventh cranial nerve agenesis.
Introduction
Congenital facial palsy is a rare disorder, with a rate of occurrence around 2 per 1000 live births, and it can be easily diagnosed. 1 It has a great impact on the newborn, mainly represented by nursing difficulty and incomplete eye closure, and later on verbal function, facial and emotional expressions and mastication. This condition can be caused by birth related trauma (78%-91%),1,2 or developmental etiologies. Knowing the cause of the seventh cranial nerve palsy is crucial since the underlying pathophysiology affects the prognosis and course of treatment. We present a case of an infant suffering a non-syndromic isolated agenesis of the right facial nerve diagnosed thanks to magnetic resonance imaging (MRI) adapted sequences and high-resolution computed tomography (CT) scan.
Case Presentation
An 11 months old boy, who was a healthy full-term infant born via vaginal delivery, with no birth trauma nor anterior medical family history, presented to pediatric medical consultation for an asymmetrical face. The patient had a normal mental and physical development.
The mother had noticed that her child could not completely close his right eye, even while sleeping, since birth.
Physical examination revealed a facial asymmetry, an incomplete right eye closure, a deviated mouth angle toward the left, and a right–sided effacement of the nasolabial furrow, a total paralysis graded VI on the house-brackmann grading system. The rest of the neurological examination was normal, indicating that there was no additional cranial nerve dysfunction.
The infant underwent an electromyography exam that showed a total denervation of the temporofacial branch and the cervicofacial branch, and the absence of the blink reflex which revealed a severe peripheral right palsy.
Standard MRI sequences with a 1.5 Tesla superconducting system were first performed, namely rapid spin echo T1 in the sagittal plane, T2 in the axial plane, 3-dimensional (3D) fluid-attenuated inversion recovery (FLAIR), and diffusion weighted imaging (DWI), to exclude an intracranial abnormality. To assess the facial nerve pathway and other cranial nerves, three-dimensional high-resolution T2 weighted sequence, gradient recalled echo, constructive interference in steady state (CISS), fast spin echo, Sampling Perfection with Application optimized Contrast using different flip angle Evolution (SPACE), 3D non-contrast T1 weighted imaging using the pointwise encoding time reduction with radial acquisition (PETRA), were also obtained.
On standard brain sequencing, no obvious abnormalities were found. However, the 3D CISS sequence revealed the absence of the protuberance of the right facial colliculus (Figure 1) and the right-sided facial nerve along its entire path, with the cisternal portion of the internal auditory canal containing the vestibulocochlear nerve solely (Figures 2, 3a and 4a). The facial nerve was visible on the left side (Figures 2, 3b, 4b, 5a and b). No pathological contrast uptake was found along the facial nerve. The remaining cranial nerves were present and had a normal aspect. Parotid glands had no obvious abnormality.

Axial image of high-resolution T2 weighted three-dimensional sequence, gradient recalled echo (CISS) showing a normal appearance of the left facial colliculus (arrow) and the absence of the protrusion of the right facial colliculus (head arrow).
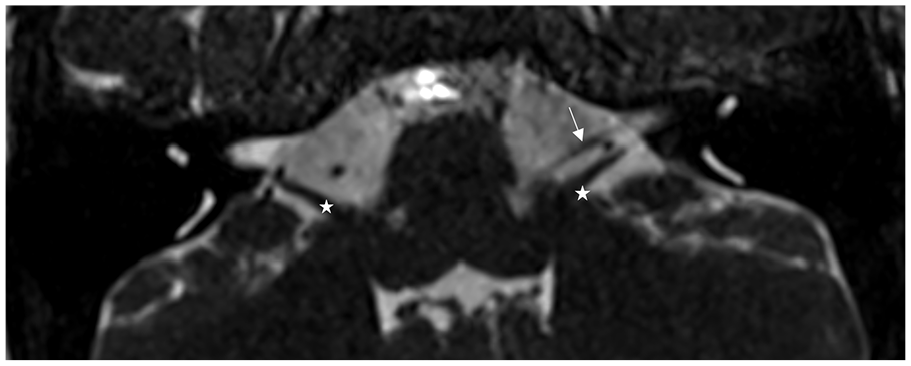
Axial image of high-resolution T2 weighted three-dimensional sequence, gradient recalled echo (CISS) image showing a normal aspect of the cisternal segment of the left facial nerve (white arrow), anterior to the cochleovestibular nerve (white star). Non visualization of the cisternal segment of the right facial nerve.

Axial image of high-resolution T2 weighted, gradient recalled echo (CISS) images. (a) Right side: Absence of the labyrinthine segment of the right facial nerve and the geniculate fossa (Asterix). (b) Left side: normal aspect of the labyrinthine segment of the left facial nerve and the geniculate fossa (white arrow).

Sagittal oblique T2 weighted high-resolution three-dimensional sequence, gradient recalled echo (CISS) images. (a) Right side: Emptiness of the antero-superior quadrant and absence of the facial nerve. Visualization of the superior and inferior vestibular nerves (double arrow) and the cochlear nerve (white arrow). (b) Left side: normal aspect of the sagittal oblique reconstruction image of internal auditory canal appearing as 4 dots. Intracanalicular segment of the facial nerve (head arrow), inferior vestibular nerves (double arrow) and the cochlear nerve (white arrow).

Axial image of T1 weighted imaging non contrast using the pointwise encoding time reduction with radial acquisition, known as PETRA (3D) showing the normal path and signal of the left facial nerve (head arrow): geniculate fossa (a), and the mastoid segment (b).
The CT scan did not show any abnormalities of the middle and inner ear structures except for an aplasia of the tympanic and mastoid facial canal segments (Figures 6 and 7), and the absence of visualization of the stylomastoid foramen (Figure 7) on the right side.

Axial high-resolution CT scan showing the normal path of the left facial nerve (head arrow). Geniculate fossa (a), tympanic segment in the fallopian canal (b) and mastoid segment (c). Absence of the right sided geniculate fossa, fallopian canal and mastoid segment

Coronal high-resolution CT scan showing the normal path of the left facial nerve (head arrow). Tympanic segment in the fallopian canal (a) and the stylomastoid foramen (b). Absence of the right sided fallopian canal and stylomastoid foramen.
Discussion
Congenital facial palsy (CFP) can be divided into traumatic and developmental categories, unilateral and bilateral, complete and incomplete. 3 The distinction between developmental and birth trauma-related causes of CFP is crucial for treatment planning and the prognosis. The diagnosis may be made based on the medical history and the physical examination of the patient, but occasionally, an MRI is necessary.
Birth trauma is the most common cause of congenital unilateral facial palsy, with an estimated frequency of 78 to 91%.1,2 Found particularly when there is a history of an extended labor, use of forceps, high birth weight, or periauricular ecchymoses. 4 Usually transitory, these facial palsies have a good prognosis and completely recover in few weeks, unlike the ones caused by a developmental abnormality that are permanent, and therefore have a poor prognosis.
Facial nerve aplasia or hypoplasia is rarely isolated and can be part of syndromic associations, such as: Moebius syndrome, which includes as major criteria the impairment of the sixth cranial nerve associated or not with additional cranial nerve paralysis, musculoskeletal abnormalities or orofacial deformities, 5 Poland syndrome which is characterized by absent major and minor pectoral muscles. CFP is rarely reported in the oculo-auriculo-vertebral syndrome, often referred to as the Goldenhaar syndrome. It is a deficiency in the growth of the first and second branchial arches that causes incomplete unilateral development of the ear, nose, soft palate, lip, and mandible. 6
The severity of the VII cranial nerve maldevelopment can be graded from 0 to 4: 0 indicates no abnormalities, 1 indicates unilateral hypoplasia, 2 indicates unilateral aplasia, 3 indicates bilateral facial nerve aplasia or hypoplasia, and 4 indicates facial nerve aplasia or hypoplasia linked to other cranial nerve palsies. 7 This case was a unilateral facial nerve aplasia and was therefore graded 2.
MRI has a major role in differentiating between developmental, and birth trauma related CFP, by analyzing the facial nerve segments and its brainstem nucleus, and detecting other cranial nerves impairment. For a proper interpretation of a facial nerve MRI, one must have a thorough understanding of the MRI protocol to perform, the regional lecture, and the anatomical findings.
The most important sequences to perform are the three-dimensional high-resolution T2 weighted sequence, providing an excellent contrast between the cerebrospinal fluid and cranial nerves: gradient recalled echo (CISS on Siemens, FIESTA on GE, and BFFE on Philips), and fast spin echo (SPACE on Siemens).
Although both are often employed, some studies favor 3D fast spin echo (FSE) for it reduces the susceptibility artifact created at the air-bone interfaces of the skull base and removes banding artifact. 8
In our institution, we use the pointwise encoding time reduction with radial acquisition, known as PETRA, ultrashort echo time. This sequence allows visualization of the facial nerve without using intravenous contrast from the brain stem, through the temporal bone, to the stylomastoid foramen. It reduces the air related artifacts coming from the mastoid cells and the middle ear cavity, thus providing a better analysis of the different segments of the facial nerve. 9
We also use the compressed sensing volume-interpolated breath-hold examination (CS-VIBE) 3D sequence post-contrast for its ability to detect facial neuritis with a comparable efficiency to the traditional T1 mprage, and a shorter scan time. 10
The intraparotid segment used to be very hard to distinguish in MRI images. However, thanks to some specific sequences developed lately like 3D turbo-spin-echo (TSE) sequence with short-term inversion recovery (STIR) black-blood sequence that uses a pseudo-steady state sweep in combination with a Motion Sensitized Driven Equilibrium pulse, also known as 3D crani, 11 CISS sequence on a 3T MRI machine, 12 we can visualize it and therefore analyze it.
As for the high-resolution CT scan, it provides an exceptional resolution of the temporal bone and fallopian canal in the bone, and detect cochlea-vestibular associated abnormalities.
A good understanding of facial nerve anatomy is crucial for a good interpretation. There are 3 brainstem nuclei from which the seventh cranial nerve develops: motor (the biggest), sensory, and parasympathetic. The motor fibers of the facial nerve circle dorsally around the sixth nerve nucleus in the lower pontine brainstem to create the facial colliculus, responsible for a protrusion in the floor of the fourth ventricle (Figure 1). At the ponto-medullary junction, which is located on the lower edge of the pons, the facial nerve leaves the brainstem. The facial nerve can now be divided into 5 intracranial segments (cisternal, intracanalicular, labyrinthine, tympanic, and mastoid) and one extracranial intraparotid segment. 13
The facial nerve’s cisternal segment is the section that travels through the cerebellopontine angle (CPA) cistern from the brainstem to the internal auditory canal’s porus acusticus. It is located anterior to the vestibule-cochlear. 13
At the medial side of the internal auditory canal, the intracanalicular segment begins in the porus acusticus. It is best seen on oblique sagittal T2 weighted high-resolution three-dimensional sequence, as an independent structure located superiorly from the cochlear nerve and anteriorly from the superior vestibular branch. 13
The facial nerve’s labyrinthine segment moves anterolaterally at an angle of 125º from the internal auditory canal while respecting its long axis, and ends in the geniculate fossa where the facial canal form an angle of 75º. 13
The facial nerve’s tympanic segment runs straight from the geniculate fossa to the posterior genu. It is situated below the lateral semicircular canal and above the oval window.
Then, it starts its second turn into the posterior tympanic wall behind the incus’ short process to create the posterior genu at an angle around 110º and form the mastoid segment.
The mastoid segment runs from the posterior genu to the stylomastoid foramen and connect medially to the jugular bulb. 13
the extracranial intraparotid segment is the last facial nerve portion and it divides into branches within the parotid gland. 13
The agenesis of the facial nerve has a poor prognosis. The cornerstone of treatment is physiotherapy where some patients regain some function, thanks to aberrant innervations of facial muscles by other adjacent cranial nerves, such as the 5th, 9th, and 12th nerves. 14
Conclusion
High resolution CT scan and MRI with adapted sequences are essential to differentiate between facial nerve aplasia or hypoplasia and other diagnosis. The absence or the thinning of the seventh cranial nerve confirm the diagnosis. These techniques help detect other abnormalities and suggest syndromic or non-syndromic etiologies, essential for a good clinical and surgical management.
Footnotes
Author Contributions
All the authors confirm their contribution to the paper for the following: study conception and design, data collection, analysis, and manuscript preparation
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics Approval
Our institution does not require ethical approval for reporting individual cases or case series.
Informed Consent
Written informed consent was obtained from a legally authorized representative(s) for anonymized patient information to be published in this article.