
Abstract
Objective. We assessed the proportion of and factors associated with mothers initiating and continuing breastfeeding (BF) for ≥4 months in a rural town of the Dominican Republic. Methods. A survey was administered to 190 mothers of children cared for at a free clinic in Consuelo. Modified bivariate and multivariable Poisson regressions were utilized in data analysis. Results. BF was initiated in 89.5% of cases and continued ≥4 months in 81.7% of cases. Maternal education beyond secondary school [adjusted RR = 1.13, 95% CI: (1.04-1.24), 0.010], and visiting both public and private antenatal clinics [adjusted RR = 1.25; 95% CI: (1.10-1.37), 0.010] were associated with BF initiation. Public and private antenatal clinic attendance [adjusted RR = 1.01, 95% CI: (0.45-2.23), 0.020], Cesarean section [adjusted RR = 0.81, 95% CI: (0.68-0.98), 0.026], number of biological children [adjusted RR = 0.95, 95% CI: (0.90-1.00), 0.032] and maternal employment [adjusted RR = 0.89, 95% CI: (0.79-0.99), 0.048] were associated with BF continuation. Conclusions. These results provide valuable insights for targeting specific populations in future breastfeeding education interventions.
Background
Breastfeeding has multiple maternal and child health benefits, including strengthening the mother-child bond. 1 In addition to improving cognitive development and preventing the risk of obesity and diabetes, breastfeeding is associated with protection from childhood illnesses.2,3 Maternal benefits include reduced risk of stroke, heart attack and of developing breast and ovarian cancer.2,3 Breastmilk remains the healthiest and most accessible source of infant nutrition. 3
The World Health Organization (WHO) and United Nations International Children’s Emergency Fund (UNICEF) recommend that mothers initiate breastfeeding within 1 hour of birth and continue exclusive breastfeeding for the first 6 months.4,5 Globally, only about 40% of infants are breastfed in the critical first hour of life, and 44% of infants aged 0 to 6 months are exclusively breastfed.4,6 Factors contributing to low breastfeeding rates include unsupportive work policies and health center practices, problems with lactation and infant latching, cultural norms, infant nutritional concerns, and concerns about maternal medications while breastfeeding.7,8
The Dominican Republic (DR) has one of the lowest exclusive breastfeeding rates globally. 9 UNICEF reports that while on average 30% of infants aged 0 to 6 months are exclusively breastfed in the Latin American and Caribbean region, only 4% are in the DR. 10 Recent studies in the DR indicate that rates of exclusive breastfeeding (EBF) have been decreasing over time. 11 Demographic Health Surveys (DHS) from various Latin American countries, including Bolivia, Brazil, Colombia, Peru, and the DR, reveal that all countries exhibited increases in duration of breastfeeding except the DR. 11
More recently, early complementary feeding, including the introduction of water, milk, and formula, has been attributed to lower rates of EBF in the DR. 12 On the island of Hispaniola, 69.8% of infants in the DR have exposure to milk-based pre-lacteal feeds, while only 20.1% of Haitian infants are exposed. 13 The DR has experienced a rapid increase in Cesarean section prevalence, up to 63% in 2019. 14 Globally, a Cesarean section delivery is related to a lower rate of breastfeeding initiation within the first hour of life and an increased rate of early complementary feeding.15,16 We speculate that factors such as, maternal age, number of biological children, as well as employment status might be associated with lower initiation rates after a Cesarean section delivery.
There are multiple factors that adversely affect EBF rates in the DR. In urban settings, these include suboptimal EBF support at mother’s work, lack of information on the nutritional benefits of breastfeeding, and lack of breastfeeding support. 17 In rural settings, there are misconceptions of the quality and quantity of breastmilk. 18 National surveys reveal various misconceptions including that EBF is insufficient, inconvenient as compared to formula feeding, unsafe and may have negative physical impacts, such as altering breast shape in the mother. 11
This project from Consuelo, a rural town in the DR, aims to inform future interventions focused on the improvement of local breastfeeding rates. We describe the proportion of mothers who initiated breastfeeding within the first week of life, the proportion who breastfed for ≥4 months and factors associated with these 2 outcomes.
Methods
Study Design and Data Collection
In this cross-sectional cohort study, mothers of children aged 0 to 5 years cared for at Niños Primeros en Salud (NPS) clinic in Consuelo, DR were interviewed using a Spanish survey. The survey was developed following a literature review of breastfeeding in the DR19-22 and in consultation with NPS clinic healthcare providers. The survey contained 17 questions and collected sociodemographic, family, antenatal, birth, and breastfeeding information. Eligible participants for the study on breastfeeding initiation included mothers of children ≤5 years of age who lived in one of the 9 NPS neighborhoods at the time of the survey. Eligibility of participants for the continuation of breastfeeding study included mothers of children >4 months and <5 years of age who lived in one of the 9 NPS neighborhoods at the time of the survey. If participants had more than 1 child, they were asked to answer with their youngest child in mind.
Following verbal consent for this clinic quality improvement initiative, the survey was administered orally by a single person (AB) between July 17th 2021 and August 12th 2021 to participants following patients’ regularly scheduled clinic appointments. The survey was also administered in each of the 9 Consuelo neighborhoods served by the NPS clinic at the time.
Consuelo is a rural town with a population of approximately 60 000 located in the province of San Pedro de Macorís in the Eastern DR. The NPS clinic serves 9 neighborhoods in Consuelo, offering free evidence-based primary and preventative care and health education to children between 0 and 5 years of age and their families. The clinic partners with community health promoters, at least 1 per neighborhood, who focus on child health including breastfeeding practices. During survey administration, 490 children received care at NPS. The minimum and maximum desired sample sizes were 20% (n = 98) and 40% (n = 196) of the eligible study population (n = 490), respectively.
Eligible participants were identified by a registered nurse (RC). The survey administrator was trained in obtaining verbal consent, and verbally asking and recording written answers on a paper survey. The survey lasted 10 to 15 minutes. No follow up instructions were given in this cross-sectional cohort study.
Data collection was carried out in 2 parts—survey administration and patient chart review. Data extracted from the patient charts included maternal age, mode of birth, number of weeks of gestation, and family medical history.
Data Analysis
Descriptive data were summarized by breastfeeding status using standard descriptive statistics including the proportion of mothers who initiated breastfeeding and the proportion who breastfed for ≥4 months. The independent variables remained the same for both analyses, and included maternal age, age of most recent child, number of biological children, number of children in patient’s household, mode of birth, number of pregnancies, number of antenatal medical visits, health center visited during pregnancy, health center visited at birth, time between recent pregnancies, maternal pre-existing health conditions, employment status, educational level, and home neighborhood.
Data were analyzed using STATA/BE Version 17.0 (College Station, TX). Relationships between pairs of categorical characteristics, listed in Tables 1 and 2, are presented as a frequency (n) and percentage (%). The distribution of continuous patient characteristics were compared across categorical groups using Wilcoxon rank-sum test and described with total range, median and interquartile range (IQR).
Baseline Characteristics of Participating Children and Mothers in the Study—Whole Cohort and Then Summarized by Those Who Breastfed in the First Week or Did Not (n = 172 Unless Otherwise Noted).
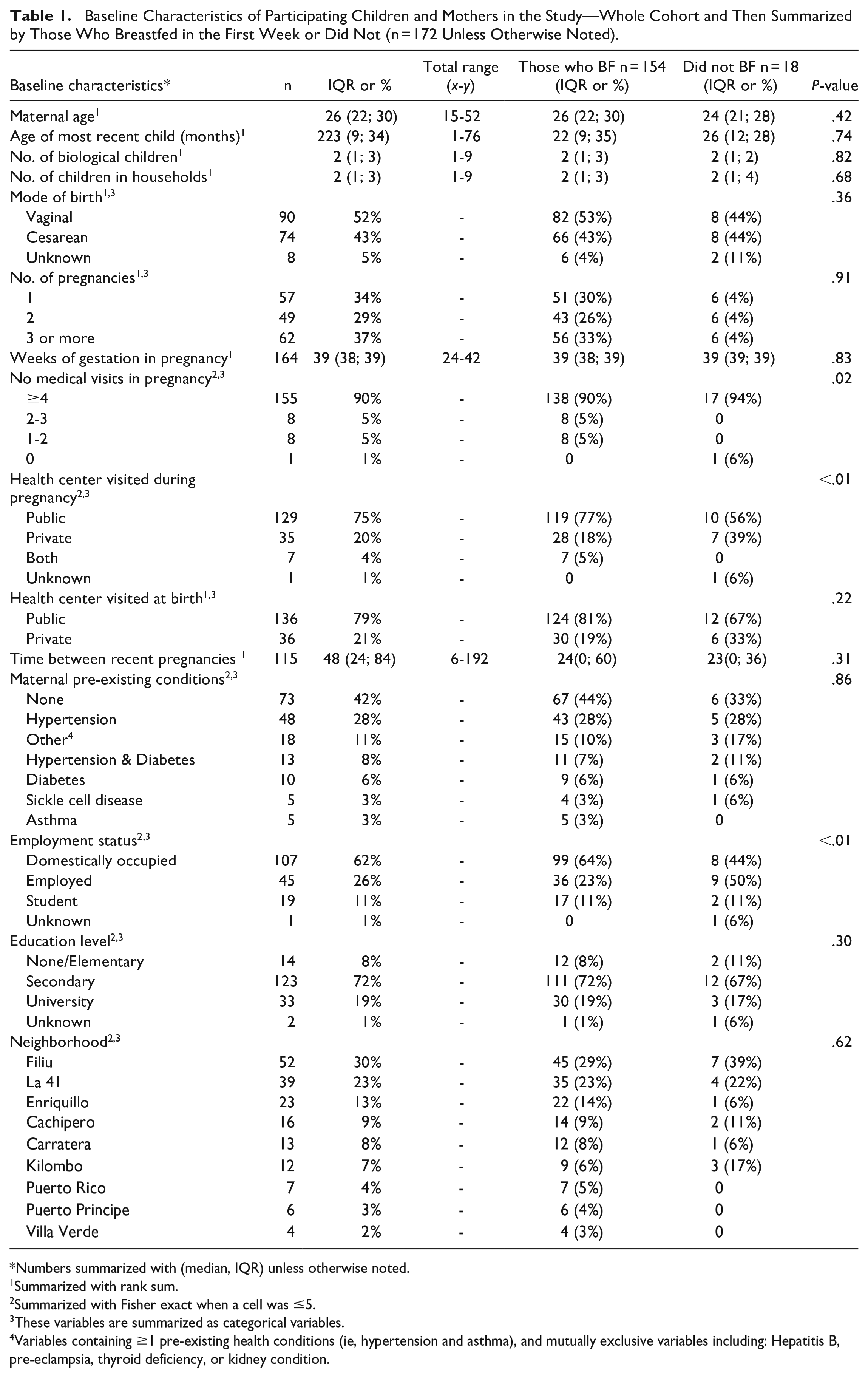
Numbers summarized with (median, IQR) unless otherwise noted.
Summarized with rank sum.
Summarized with Fisher exact when a cell was ≤5.
These variables are summarized as categorical variables.
Variables containing ≥1 pre-existing health conditions (ie, hypertension and asthma), and mutually exclusive variables including: Hepatitis B, pre-eclampsia, thyroid deficiency, or kidney condition.
Baseline Characteristics of Participating Children and Mothers in the Study—Whole Cohort and Then Summarized by Those Who Breastfed <4 or ≥4 Months (n = 153 Unless Otherwise Noted).

Numbers summarized with (median, IQR) unless otherwise noted.
Summarized with rank sum.
Summarized with Fisher exact when a cell was ≤5.
These variables are summarized as categorical variables.
Variables containing ≥1 pre-existing health conditions (ie, hypertension and asthma), and mutually exclusive variables including: Hepatitis B, pre-eclampsia, thyroid deficiency, or kidney condition.
Bivariate analyses were conducted using modified Poisson regression models to identify patient characteristics that had significant associations with outcome variables. A random intercept for neighborhood was included in each modified Poisson model to adjust the standard errors for similarity in outcomes between participants of the same neighborhood. All modified Poisson regressions were run using STATA’s meglm procedure. For each independent variable, unadjusted risk ratios (RR), 95% confidence intervals (CI), and P-values were reported. For categorical variables, the first category of each variable was used as a reference in the model. Following bivariate analysis, multivariable modified Poisson models were performed to get adjusted estimates of the variables found to have bivariate associations with the outcome. Variables in each multivariable model were included if their P-value from the bivariate model was <.20. Additionally, prespecified clinically significant variables such as maternal age, number of biological children and employment status were forced into the multivariable model. Adjusted risk ratios, 95% CI, and P-values were reported for all variables from the multivariable models. Variables with a P-value < .05 were considered statistically significant.
Ethics
All participants were ensured that participation in the survey was completely voluntary, and informed that the choice whether to participate would not affect the care of their child, and that there would be no consequences for their answers. Verbal assurance of the anonymity of their answers in potential publications of survey data was also given. This survey is part of ongoing quality improvement (QI) work in the NPS clinic which was reviewed by the Children’s Hospital of Philadelphia (CHOP) IRB. The study did not meet criteria as human subjects’ research, allowing for a waiver of written consent. The QI work reviewed by CHOP IRB includes both enhancing breastfeeding initiation in the first week of life and continuing breastfeeding for ≥4 months.
Results
A total of 190 participants were examined for study eligibility out of the 490 potentially eligible mothers whose children were enrolled in the NPS program. Of the 190 participants, 172 were confirmed for study eligibility (Figure 1a). The sample size represented 35% (172/490) of the study population. Analyses for those who did or did not breastfeed in the first week of life were conducted using the data collected from the 172 eligible participants. For participants ≥4 months, out of the 190 participants, 153 were confirmed to be eligible and included in this analysis (Figure 1b). The sample size represented 31% (153/490) of the study population. Tables 1 and 2 summarize the datasets for the analysis of the initiation and continuation of breastfeeding for ≥4 months, respectively.

(a) Enrollment diagram for breastfeeding (BF) in first week or never breastfed. (b) Enrollment diagram for those whose child was 4 months and older, and either did or did not breastfeed for at least 4 months.
Table 1 demonstrates that mothers who breastfed had a median age of 26 years, while those who did not breastfeed had a median age of 24 years. Both groups had a median of 2 children. Vaginal birth was more common among breastfeeding mothers (52%) compared to non-breastfeeding mothers (43%), but this difference was not statistically significant (P = .36). Regarding healthcare visits during pregnancy, 77% of breastfeeding mothers visited a public health center, while only 56% of non-breastfeeding mothers did so (P < .01). In terms of employment status, 23% of breastfeeding mothers were employed, while 50% of non-breastfeeding mothers were employed (P < .01). Education level and neighborhood did not show significant differences.
In Table 2, the baseline characteristics of mothers who breastfed for ≥4 months and those who breastfed for <4 months are described. The median maternal age was 26 years for both groups. Vaginal birth was more common among those who breastfed for more than 4 months (61%) compared to those who breastfed for ≤4 months (25%), and this difference reached statistical significance (P < .01). Furthermore, 81% of women who breastfed for ≥4 months visited a public health center during pregnancy, while only 43% of those who did not breastfeed for ≥4 months did so (P < .01). Similar patterns were observed for public health center visits at birth, with 84% of women who breastfed for ≥4 months visiting, compared to 54% of those who did not (P < .01). Employment status differed, with 34% of those who breastfed for ≥4 months being employed, compared to 46% of those who did not (P = .04). Education level also showed a significant difference, with 10% of those who breastfed for ≥4 months having no elementary education, compared to 4% of those who breastfed for <4 months (P = .02).
Tables 3 and 4 show the results from the bivariate modified Poisson models for breastfeeding initiation and continuation of breastfeeding for at least 4 months, respectively. In the bivariate analysis to identify factors associated with breastfeeding initiation, visiting a public antenatal site during pregnancy [unadjusted RR = 1.15, 95% CI: (0.94-1.42), P = .18], visiting both public and private antenatal sites during pregnancy [unadjusted RR = 1.25, 95% CI: (1.04-50), P = .02], time between most recent and previous pregnancy [unadjusted RR = 1.00, 95% CI: (0.99-1.00), P = .06], and having a university level education [unadjusted RR = 1.06, 95% CI: (1.00-1.12), P = .03] were the only variables found to have a potential association (P < .20) with outcome. These variables were included in the multivariable model (Table 5). In the analysis of factors associated with the continuation of breastfeeding for at least 4 months, Cesarean mode of birth [unadjusted RR = 0.77, 95% CI: (0.64-0.92), P = .01], unknown mode of birth [RR = 0.27, 95% CI: (0.07-1.02), P = .05], visiting a public antenatal site during pregnancy [unadjusted RR = 2.63, 95% CI: (1.22-5.20), P < .01], health center visited at birth [unadjusted RR = 1.49, 95% CI: (1.18-1.88), P < .01], time between most recent and previous pregnancy [unadjusted RR = 1.01, 95% CI: (0.99-1.03), P = .08], employment status [unadjusted RR = 0.87, 95% CI: (0.75-1.01), P = .07] and having a secondary [unadjusted RR = 0.89, 95% CI: (0.77-1.01), P = .07] and university education level [unadjusted RR = 0.83, 95% CI = 0.64-1.06)], P = .13] had potentially significant associations, and were included in the multivariable model analysis (Table 6).
Bivariate Analysis of Demographic and Clinical Factors Associated With Initiation of Breastfeeding in Week 1 (n = 172).
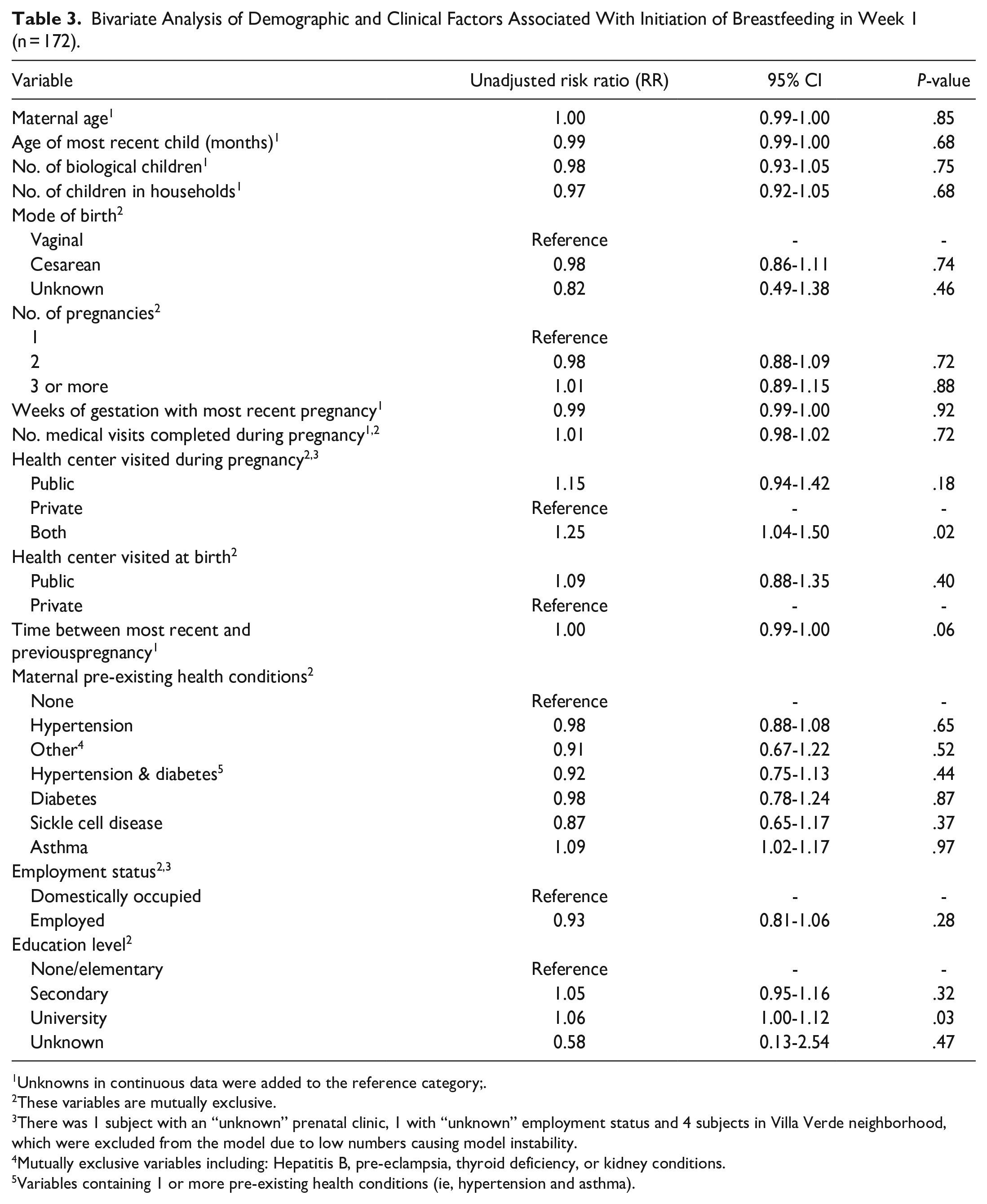
Unknowns in continuous data were added to the reference category;.
These variables are mutually exclusive.
There was 1 subject with an “unknown” prenatal clinic, 1 with “unknown” employment status and 4 subjects in Villa Verde neighborhood, which were excluded from the model due to low numbers causing model instability.
Mutually exclusive variables including: Hepatitis B, pre-eclampsia, thyroid deficiency, or kidney conditions.
Variables containing 1 or more pre-existing health conditions (ie, hypertension and asthma).
Bivariate Analysis of Demographic and Clinical Factors Associated With Those Who Breastfed <4 or ≥4 Months (n = 153).
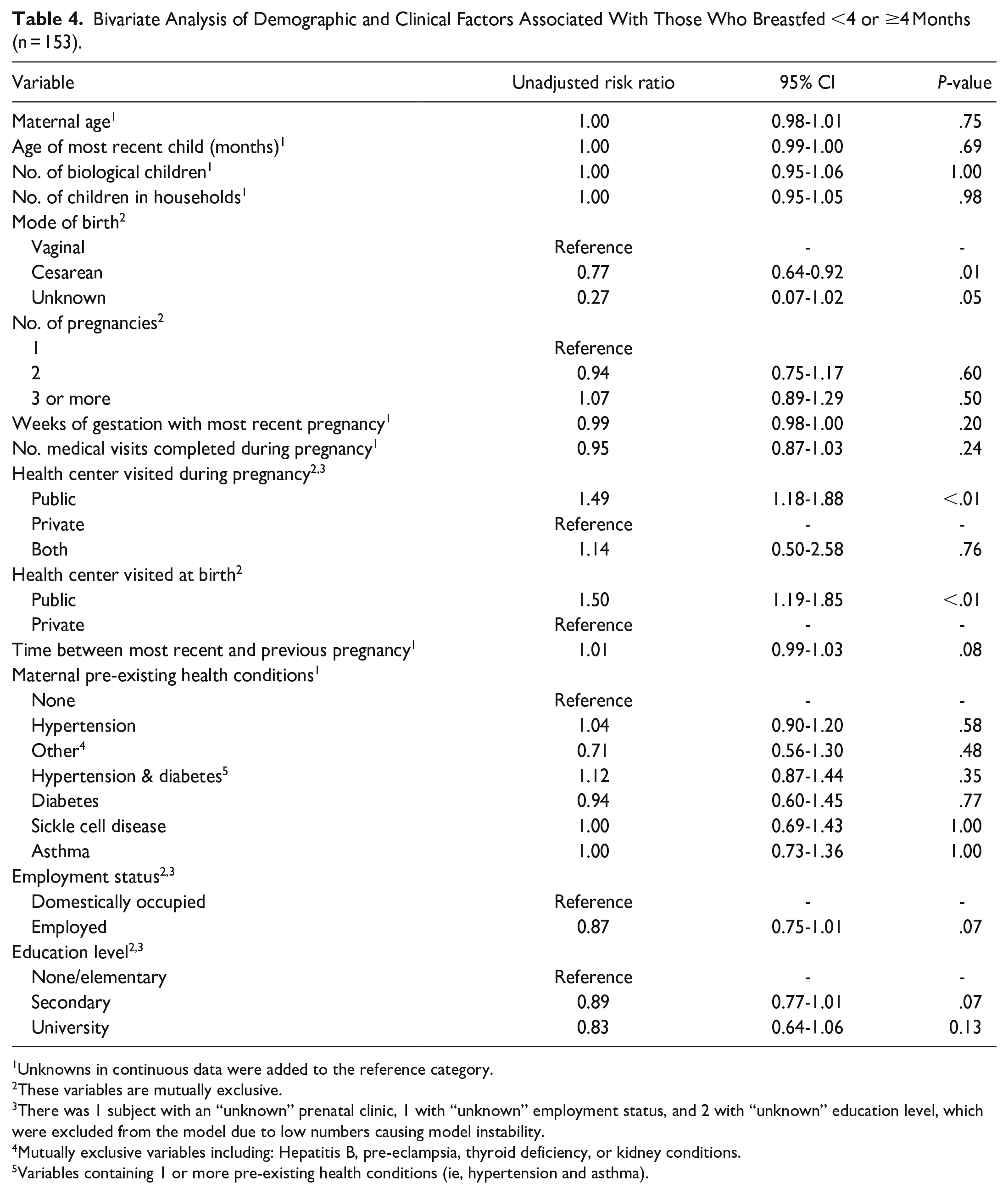
Unknowns in continuous data were added to the reference category.
These variables are mutually exclusive.
There was 1 subject with an “unknown” prenatal clinic, 1 with “unknown” employment status, and 2 with “unknown” education level, which were excluded from the model due to low numbers causing model instability.
Mutually exclusive variables including: Hepatitis B, pre-eclampsia, thyroid deficiency, or kidney conditions.
Variables containing 1 or more pre-existing health conditions (ie, hypertension and asthma).
Multivariable Analysis of Demographic and Clinical Factors Associated With Initiation of Breastfeeding in Week 1 (n = 170).
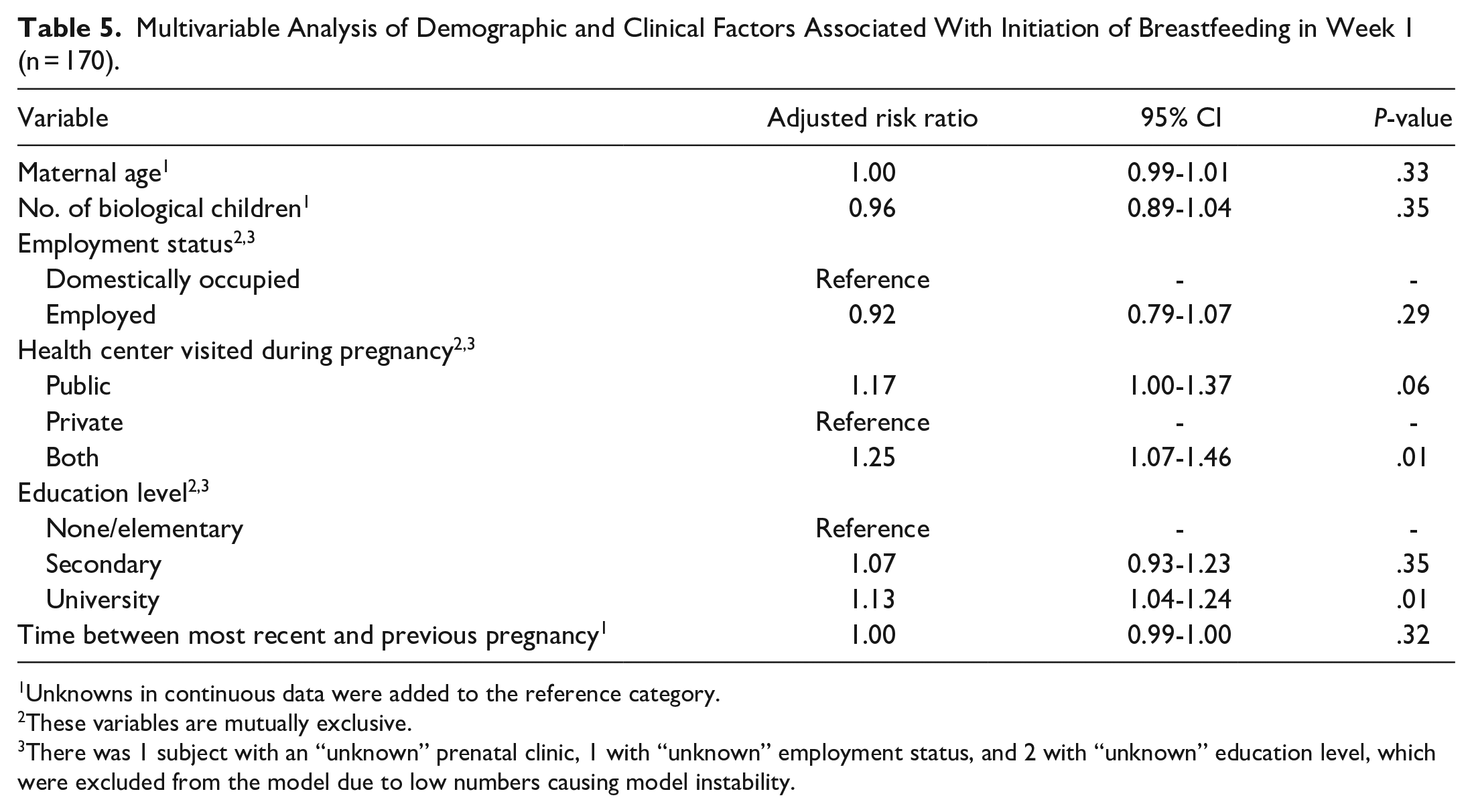
Unknowns in continuous data were added to the reference category.
These variables are mutually exclusive.
There was 1 subject with an “unknown” prenatal clinic, 1 with “unknown” employment status, and 2 with “unknown” education level, which were excluded from the model due to low numbers causing model instability.
Multivariable Analysis of Demographic and Clinical Factors Associated With Those Who Breastfed <4 or ≥4 Months (n = 151).

Unknowns in continuous data were added to the reference category;.
These variables are mutually exclusive.
There was 1 subject with an “unknown” prenatal clinic, 1 with “unknown” employment status, and 2 with “unknown” education level, which were excluded from the model due to low numbers causing model instability.
The results from the multivariable modified Poisson models are summarized in Tables 5 and 6. In the initiation of breastfeeding analysis, mothers who were educated beyond secondary school were more likely to initiate BF [adjusted RR = 1.13, 95% CI: (1.04-1.24), P = .01]. Mothers who visited both public and private health centers during antenatal medical visits were more likely to initiate breastfeeding and continue breastfeeding for ≥4 months than mothers who only visited private clinics [adjusted RR = 1.25, 95% CI:(1.07-1.46), P = .01] and [adjusted RR = 1.01, 95% CI: (0.45-2.23), P = .02], respectively.
For continuation of breastfeeding for ≥4 months, the multivariable model found that women who had greater number of biological children were less likely to continue breastfeeding ≥4 months [adjusted RR = 0.89, 95% CI: (0.79-0.99), P = .03]. Employment status was also potentially associated with a lack of breastfeeding continuation [adjusted RR = 0.89, 95% CI: (0.79-0.99), P = .05]. Women who had a Cesarean section were 19% less likely than women who had vaginal births to breastfeed for ≥4 months [adjusted RR = 0.81, 95% CI: (0.68-0.98), P = .03].
Discussion
The initiation rate of breastfeeding reported in this study (89.5%) is significantly higher than usually reported for the Dominican Republic (DR). From the DR’s UNICEF national database, breastfeeding initiation rates have decreased significantly from 58% in 1996 to 38% in 2014. 23 Exclusive breastfeeding (EBF) rates have also experienced a decrease from 11% in 1986 to 4.6% in 2014. 24 While the World Health Organization (WHO) and UNICEF recommend exclusive breastfeeding for 6 months, many programs target the 4 month window as a key milestone toward the 6 month mark.
The continuation rate of breastfeeding for ≥4 months was 82% in children ≥4 months of age. A study analyzing data between 1990 and 2013 from Bolivia, Brazil, Columbia, Peru and the DR used national Demographic Health Surveys (DHS) to describe duration of breastfeeding—a significant increase in the duration of breastfeeding occurred in all countries analyzed over time, except the DR. 25 The World on Breastfeeding Trends Initiative (WBTi) tool protects, promotes and supports breastfeeding. A higher score denotes a favorable national policy for infant-child feeding. Despite the DR having a high WBTi score of 61 in year 2012, this favorable policy environment has not had the desired effect on breastfeeding initiation or continuation. 25 The uncharacteristically and encouragingly high rates of breastfeeding initiation and continuation for ≥4 months observed in Consuelo may be attributable to the NPS program’s decade-long multi-pronged breastfeeding initiatives, including antenatal community health visits and postnatal education by nurses and health promoters.
Study results depict a number of factors potentially associated with breastfeeding initiation and continuation. In multivariable analysis, mothers educated beyond secondary school were more likely to initiate breastfeeding than mothers with no formal education (Table 5). Previous studies in low-and-middle income countries (LMICS) have found an association between lack of maternal formal education and lower breastfeeding rates.26,27 In regions where formal maternal education levels are low, community and local health center led breastfeeding education initiatives and support groups may be important interventions to explore. Breastfeeding education interventions have been successful in improving breastfeeding rates in LMICS.21,28
Mothers visiting both a public and private antenatal clinic were more likely to initiate breastfeeding and continue breastfeeding ≥4 months, compared to those visiting a private clinic alone (Table 5). Differences in availability and quality of breastfeeding education at public and private centers could be a contributor to this discrepancy in breastfeeding rates. 29 A study from 1997 examining 1991 DHS data in the DR noted that women who gave birth at private clinics were more likely to breastfeed for a shorter duration than women who gave birth in public locations or at home.30,31 In 1993, the World Bank used data from the US Agency for International Development to examine demand for healthcare in urban regions of the DR and El Salvador. 32 The study found that public as compared to private maternal and child services tended to be more comprehensive in Santo Domingo, due to more policymaker support for these services. 32 A 2018 examination of 12 DHS surveys, including the DR, conducted between 2012 and 2014, corroborated the finding that public child health services are heavily supported by policy makers. 33 In the DR and El Salvador, private services may be more expensive than public healthcare, but low-income populations still utilize these services at a comparable rate to higher income populations—15% to 25% of the poorest quintile in Latin America use private services.32,33 Ensuring quality health care in both public and private settings is important.
Multivariate analysis also indicated that mothers who had a Cesarean section were 19% less likely to continue breastfeeding practices ≥4 months than those who delivered vaginally (Table 6). Previous studies indicate that an increasing prevalence of Cesarean section correlates with both a decrease in initiation and continuation of breastfeeding for ≥4 months. 15 Worldwide Cesarean section rates have increased dramatically from approximately 7% in 1990 to 20% in 2014, with Latin America experiencing one of the fastest growth rates. 34 In the DR these trends are even more dramatic with 63% of infants born by Cesarean section in 2019. 15 Studies in the DR have found that women of lower socioeconomic status are at greater risk of introducing milk-based pre-lacteals after Cesarean delivery, due to a lack of breastfeeding support. 35 These findings indicate the necessity for further research on the impact of having a Cesarean section on breastfeeding continuation rates and better follow up with women having Cesarean sections to optimize time breastfeeding.
Other factors found to have a potential association with decreased breastfeeding continuation rates include number of biological children and maternal employment status (Table 5). Concerns about pregnancy or desire to become pregnant have been recorded as reasons for breastfeeding cessation. 1 Maternal concerns about pregnancy risks may present a possible explanation for the association between number of biological children and decreased breastfeeding continuation rates. Limited family child support, economic burden, and cultural perceptions in LMICS may also be related to these findings and should be explored further. 36
The results indicate that mothers who were employed were 21% less likely to breastfeed ≥4 months (Table 6). Maternal employment in LMICS has been linked to lower rates of breastfeeding continuation in previous studies.37,38 Previous literature suggests an increase in breastfeeding support for formally employed mothers to promote breastfeeding continuation for the WHO recommended timeframe.39,40
Study Limitations
This study has some limitations. Participants were from a single center, potentially limiting generalizability. However, to maximize statistical power of the study, over 30% of the potential study population were surveyed using a questionnaire administered by the same interviewer. A sample size calculation was not performed. The survey was conducted verbally, as a series of closed and open-ended questions. Structured questionnaires may introduce respondent bias. 41 However, to mitigate this, participants were verbally reassured that responses would have no negative impact on care their children received at the clinic. A pilot conducted prior to the study clarified survey questions and determined options for the closed questions. All closed questions included an option designated “Other” to record all potential answers.
Conclusions
We report high rates of both initiation and continuation of breastfeeding for ≥4 months from a primary care pediatric clinic in a rural town of the DR. These high rates likely reflect the impact of over a decade of community work on breastfeeding education. Receiving an education beyond secondary school was a potential indicator of higher breastfeeding initiation rates. Factors associated with the initiation and continuation of breastfeeding included receiving antenatal care in the public sector. Mothers who had a Cesarean section were less likely to breastfeed for ≥4 months in comparison to those who had a vaginal birth. Other factors potentially associated with breastfeeding continuation include number of biological children and maternal employment status. Further studies across the country and globally should confirm these findings and interrogate the relationship between the indicated risk factors and breastfeeding, with a focus on maternal breastfeeding education.
Supplemental Material
sj-docx-1-gph-10.1177_2333794X231200207 – Supplemental material for Factors Associated With Initiating Breastfeeding and Continuing it for At Least 4 Months in Consuelo, a Rural Town in the Dominican Republic
Supplemental material, sj-docx-1-gph-10.1177_2333794X231200207 for Factors Associated With Initiating Breastfeeding and Continuing it for At Least 4 Months in Consuelo, a Rural Town in the Dominican Republic by Anjalee Bhuyan, Anabel Fernandez, Jennifer A. Faerber, Ingrid Japa, Angie Alvarez, Ramona Cordero, Ivelisse Tavarez, Nahara Saballos and Andrew P. Steenhoff in Global Pediatric Health
Footnotes
Author Contributions
AB, AF and APS wrote the manuscript. AB conducted patient interviews. AB, JAF and APS completed the statistical analyses. IJ, AA, RC, IT and NS worked on project conceptualization and methodology. All authors reviewed the final manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The project was funded by the CHOP Global Health Center.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.