
Abstract
Objectives:
In asthmatic patients, studies suggest that alexithymia leads to negative consequences and emotions that can affect physical, psychological, and social aspects of life. We designed this study to determine the frequency of alexithymia in Latin American patients with asthma, as well as to understand how this personality trait and each of its components interact with asthma severity and demographic variables, and their implications on treatment adherence and disease control under such setting.
Methods:
We conducted a cross-sectional study, involving 265 Latin American patients with asthma. Patient demographics and clinical characteristics were reported. The presence of alexithymia, asthma severity, and control, as well as treatment adherence, was analyzed. To assess the presence of alexithymia, the 20-item Toronto Alexithymia Scale was used. For the statistical analyses, we performed Kendall’s tau-b correlation coefficient, chi-square tests for association, and one-way analysis of variance.
Results:
A total of 265 patients participated in the study with a gender distribution of 69.4% female and an average age of 54.7 years. In total, 30.2% of individuals presented alexithymia. There was a statistically significant correlation between educational level and 20-item Toronto Alexithymia Scale categories (p < .001), as well as a higher proportion of severe (35.1%, p = .001) and uncontrolled (50.0%, p = .185) asthma in patients with alexithymia. A higher proportion of patients with some level of non-adherence was seen on those with uncontrolled asthma (68.5%, p = .008).
Conclusion:
Our results suggest that in our sample, 3 in 10 Latin American asthma patients have alexithymia, and such mental condition is more common in those individuals with lower educational levels. Individuals with alexithymia present with severe asthma more frequently than do patients with possible or no alexithymia and are also more likely to have their disease uncontrolled.
Introduction
Alexithymia is a disorder of affect regulation characterized by a reduced ability to recognize and describe internal emotions. 1 This personality trait has been associated with several mental and physical health problems, and it is now regarded as a factor influencing treatment response across various medical conditions. 2 Several theoretical mechanisms have been suggested to explain how alexithymia might be associated with the development of health problems. For instance, the impaired emotion processing and affect regulating capacities, together with the limited ability to adapt to stressful situations, can lead to unhealthy behaviors, such as substance abuse, sedentary lifestyle, and poor nutrition. 3 Furthermore, there is difficulty recognizing physical and emotional symptoms, thus leading to delays or excessive use of medical resources. 4 Even though there is no definitive answer yet on this condition as a prognostic risk factor for disease, in a brief review of prospective studies, Kojima found that approximately half of the analyzed studies reported statistically significant adverse effects on health outcomes related to alexithymia. 4
In asthmatic patients, studies suggest that alexithymia leads to negative consequences and emotions that can affect physical, psychological, and social aspects of life.5–8 For instance, asthma appears to be less controlled in alexithymic patients, and in the case of extremely severe or nearly fatal attacks, it has been associated with more disease exacerbations.6,9 Moreover, alexithymic patients with asthma were found to have a greater frequency of hospitalizations due to the disease, as well as being associated with poor treatment adherence and worse health-related quality of life (HRQoL).8,10 Empirical studies show a wide range of prevalence in which high levels of alexithymia have been evidenced in asthmatic patients (ranging from 10% to 60%). 11 This variation may be attributed to different sample composition, cultural and geographical differences, and methods of assessing alexithymia. 11 Consequently, the alexithymic trait appears to influence the course and management of asthmatic patients, but the exact extent of this personality trait on some regions with high prevalence of asthma and worse disease control is yet to be established.
In Latin America, there is a high prevalence of asthma compared to the rest of the world (15.9% versus 14.1%), with a recent systematic review suggesting that patients are inadequately managed and frequently overestimated their degree of disease control. 12 Still, studies on the subject of alexithymia and asthma are largely missing in Latin American countries. As such, we designed this study to determine the frequency of alexithymia in Latin American patients with asthma, as well as to understand how this personality trait and each of its components interact with asthma severity and demographic variables, and their implications on treatment adherence and disease control under such setting.
Methods
Study design
This is a cross-sectional study involving 265 asthmatics from outpatient centers at various Latin American countries (Argentina, n = 165; Peru, n = 15; Ecuador, n = 85), from January to September 2018. To participate in the study, patients had to be over 18 years of age, with a diagnosis of persistent asthma, according to the guidelines proposed by the Global Initiative for Asthma (GINA). 13 We excluded patients with psychiatric diseases, language impairment, history of recent hospitalizations related to asthma in the same year, patients with intermittent asthma, and those with difficulty viewing the survey. Patient demographics and clinical characteristics were reported. The presence of alexithymia, asthma severity and control, as well as treatment adherence, was analyzed.
For the purpose of the study, a better understanding of the variables is required; that is why the assessment tools, cut-off values, and categories are best described as follows. To assess the presence of alexithymia, the 20-item Toronto Alexithymia Scale (TAS-20) was used, which has been previously validated in Spanish.14,15 The TAS-20 is structured by three factors (Factor 1—difficulty identifying feelings; Factor 2—difficulty describing feelings; and Factor 3—externally oriented thinking) which are congruent with the alexithymia construct. 16 The TAS-20 cut-off scoring used was as follows: equal or less than 51, non-alexithymia; between 52 and 60, possible alexithymia; and equal or greater than 61, alexithymia.
With respect to asthma severity, the disease was classified based on the prescribed treatment step. 13 Given the fact that asthma severity is not a static feature which changes over months to years, physicians determined the disease severity according to the last treatment regimen prescribed. Steps 1–2 treatments were considered mild asthma; Step 3 as moderate asthma; and Steps 4–5 as moderate-to-severe asthma. Concerning disease management, the 5-item asthma control test (ACT) was applied to measure the degree of disease control under the prescribed medication. 17 Patients with a score equal or less than 19 were consistent with poorly controlled asthma/uncontrolled asthma, while those above 19 were considered to have a well-controlled asthma. 18 Patients achieving a perfect score of 25 were labeled as having completely controlled asthma. 17
Finally, the Morisky Green Levine Medication Adherence Scale (MGLS) was used to determine the degree of treatment non-adherence.19–21 We used a dichotomous definition of adherence, with 0 points denoting perfect adherence and points > 1 indicating some level of non-adherence. 22
Sample size
Sample size was calculated using G*Power version 3.0.10. Due to different statistical methods applied, we set the parameters for the test with the highest sample size requirement, that is, an X2 test. Setting a medium effect size (w = 0.3), an α-error probability of 0.05, a power of 0.80, and 8 degrees of freedom, the required sample size was 167 patients. To overcome type II errors (missing data, unbalanced groups, etc.), the sample size was further expanded to 265 patients, whose actual achieved power was 0.959.
Ethical considerations
This study was approved by the ethics committee Comité de ética e Investigación en Seres Humanos (HCK-CEISH), Guayaquil, Ecuador.
Statistical analyses
Descriptive statistics were performed for demographic and clinical variables, such as age, gender, years with disease, TAS-20 score, asthma severity, asthma control, and more.
A standard multiple regression was run to predict the TAS-20 score based on age, gender, education level, marital status, years with asthma, asthma severity, asthma control test score, and level of adherence.
Kendall’s tau-b correlation coefficient was used to measure possible associations between the TAS-20 score and continuous variables, such as age and years with disease. However, for nominal variables, chi-square tests for association were performed, as such possible associations between the TAS-20 categories (non-alexithymia, possible alexithymia, and alexithymia) and gender, educational level (no education, primary school, secondary school, and undergraduate/postgraduate), marital status (single, married, divorced, widow, and consensual union), asthma severity, and the degree of asthma control could be analyzed. A chi-square test for association was also performed between the treatment adherence dichotomy (perfect adherence and some level of non-adherence) and TAS-20 categories, disease severity, and degree of asthma control.
Furthermore, a one-way analysis of variance (ANOVA) was conducted to determine if each of the three TAS-20 factors’ scores were different for all the groups within the disease severity and degree of asthma control variables. To meet the assumptions, outliers were assessed by boxplots, distribution was assessed by Shapiro–Wilk test, and homogeneity of variances was analyzed with Levene’s test of homogeneity of variances. The Bonferroni procedure was applied as a post hoc test to further explore mean score differences between each of the categories of both variables, disease severity, and degree of asthma control.
Results
The sample comprised 265 patients with a gender distribution of 69.4% female and 30.6% male, whose average age and years with disease were 54.7 and 22.0 years, respectively. Out of all patients, 30.2% individuals presented alexithymia and 23.8% possible alexithymia (Table 1). The average TAS-20 score of the selected sample was 52.8, with externally oriented thinking representing the factor with the highest mean score (Table 2). With respect to disease severity, most patients presented either mild (43.0%) or moderate (36.9%) asthma. Concerning disease control and treatment adherence, 50.6% individuals were not controlled, and 59.2% presented some level of non-adherence. Descriptive statistics of other demographic and clinical variables are included in Tables 1 and 2.
Demographic and clinical information of surveyed population (n = 265).

TAS-20: Toronto Alexithymia Scale; ACT: asthma control test; MGLS: Morisky Green Levine Medication Adherence Scale.
Mean TAS-20, ACT, and MGLS scores of surveyed population.

TAS-20: Toronto Alexithymia Scale; ACT: asthma control test; MGLS: Morisky Green Levine Medication Adherence Scale.
Multiple regression
A multiple regression was run to predict TAS-20 score from age, gender, education level, marital status, years with asthma, asthma severity, asthma control test score, and level of adherence. Linearity was revealed through partial regressions plots and a plot of studentized residuals versus the predicted values. As assessed by a Durbin–Watson statistic of 1.913, there was independence of residuals. Moreover, homoscedasticity was assessed by visual inspection of a plot of studentized residuals against unstandardized predicted values. Through tolerance values greater than 0.1, multicollinearity was discarded. Studentized deleted residuals greater than ± 3 SD, leverage values over 0.2, and values for Cook’s distance above 1 were not found. Normality was observed through Q–Q plots. The multiple regression model statistically significantly predicted the TAS-20 score, F(8, 213) = 6.300, p < .0005, adj. R2 = .161. From the selected independent variables, only education level and ACT score added statistically significantly to the prediction, p < .05 (Figure 1; Supplemental Appendix Table S2). The proportion of the categories of the selected variables within the TAS-20 and MGLS is included in Table 3 and in the Supplemental Appendix, Table S3, respectively.

Regression coefficient plot with confidence intervals of standard multiple regression. Regression coefficients’ names are placed in the Y-axis and their corresponding values express the likelihood of increasing the TAS-20 score. Reference category for gender was “female”; for education level, “no education”; for marital status, “single”; for asthma severity, “mild asthma”; for level of adherence, “some level of non-adherence.”
Associations between alexithymia with demographic variables, disease severity, and asthma control.
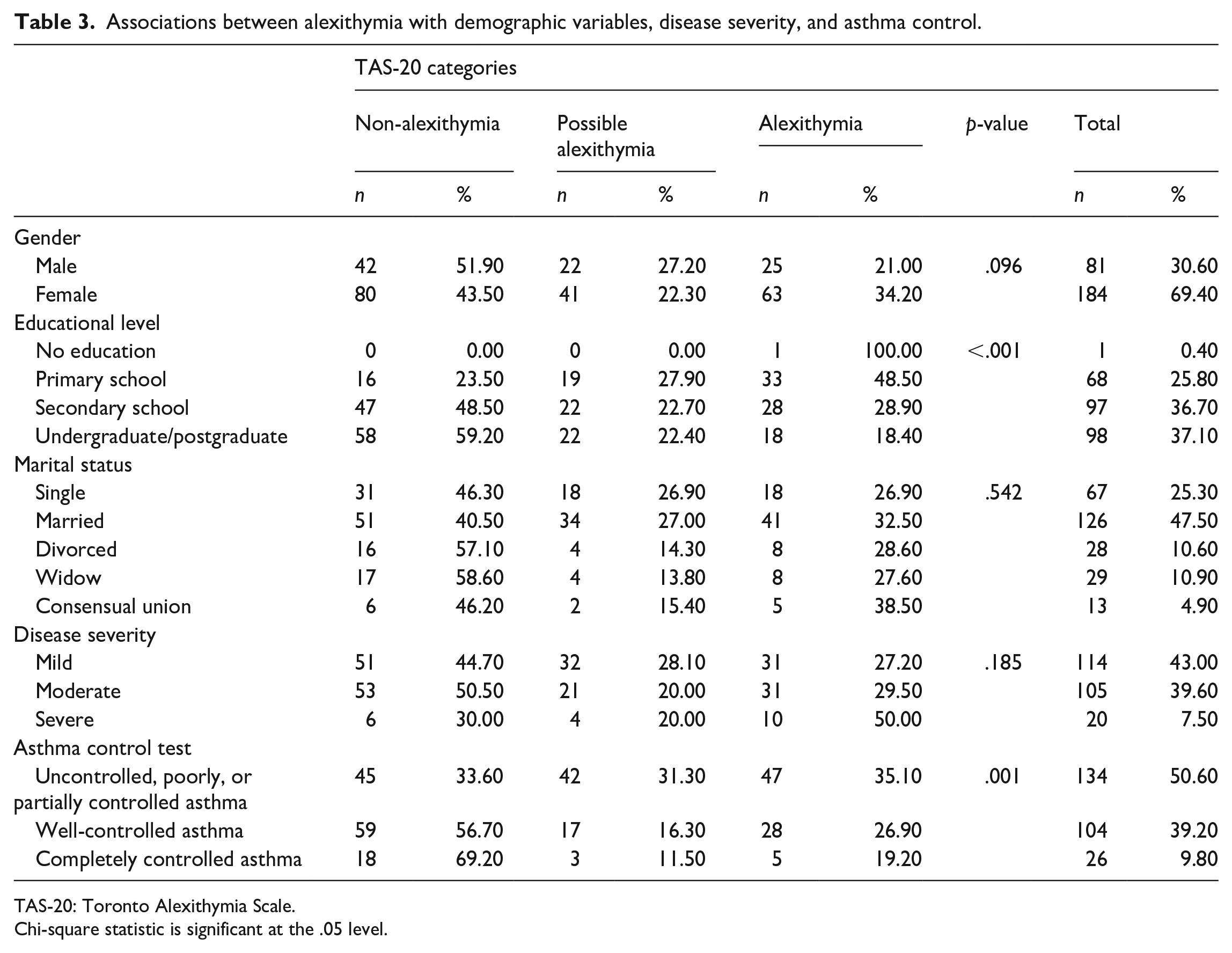
TAS-20: Toronto Alexithymia Scale.
Chi-square statistic is significant at the .05 level.
One-way ANOVA
Difficulty identifying feelings and difficulty describing feelings score differences were statistically significant between the disease severity and ACT groups (Supplemental Appendix Tables S4 and S5). Moreover, the Bonferroni procedure revealed that the “difficulty identifying feelings” score increase from both, mild (5.16, 95% CI (1.32–9.00), p = .004) and moderate disease (5.22, 95% CI (1.35–9.09), p = .004), toward severe asthma was statistically significant, as well as the “difficulty describing feelings” score increase from both, mild (2.66, 95% CI (0.09–5.24), p = .040) and moderate asthma (2.90, 95% CI (0.31–5.49), p = .022), toward severe disease (Figure 2(a)).

TAS-20 factors’ score by disease severity and degree of asthma control. (a) Overall comparison of TAS-20 factors’ scores distribution according to asthma severity groups. (b) Overall comparison of TAS-20 factors’ scores distribution according to asthma control groups.TAS-20: twenty-item Toronto Alexithymia Scale; ACT: asthma control test; Factor 1: difficulty identifying feelings; Factor 2: difficulty describing feelings; Factor 3: externally oriented thinking.
Furthermore, the “difficulty identifying feelings” score increase from well-controlled asthma (3.14, 95% CI (1.05–5.24), p = .001) and completely controlled asthma (3.84, 95% CI (0.41–7.28), p = .022) to uncontrolled asthma was statistically significant, as well as the “difficulty describing feelings” score increase from well-controlled asthma to uncontrolled asthma (1.55, 95% CI (0.15–2.95), p = .025) (Figure 2(b)). No other group differences were statistically significant.
Discussion
Alexithymia is a personality trait that appears to be associated with several pathologies, and it is considered an element of co-morbidity with increased risk of mortality. 23 The prevalence of alexithymia in the general population has been reported to be between 10%–13%, while in the setting of somatic or psychiatric/psychological disorders, it has been reported to be higher.24–29 Our results concur with these observations, since 30.2% of patients in our sample presented with alexithymia. However, it is not as high as observed in other publication with asthma patients were prevalence was 42%. 30 Interestingly, asthma patients seem to have a higher prevalence of alexithymia than other obstructive respiratory diseases, such as chronic obstructive pulmonary disease (COPD), where prevalence of alexithymia is equal to the general population unless the disease exacerbates.31,32
Understanding how alexithymia gives rise to chronic diseases is a subject of complexity. As a matter of fact, it is not certain if either alexithymia leads to chronic diseases or the contrary. Given its psychiatric nature, it has been proposed that alexithymia leads to or influences illness behaviors, affecting clinical- and patient-reported outcomes. 33 Whatever the scenario might be, it is certain that interactions between sociocultural and biological factors play a key role in the occurrence of both. For instance, alexithymia is known to be associated with poor education and low-income level, and it is commonly seen among unmarried individuals. 33 In our sample, lower education levels were associated with more alexithymia, while analysis concerning marital status showed no significant association. Moreover, even though alexithymia is more likely to present in older individuals, we could not find a statistically significant association between age and TAS-20 score, though the mean age in patients with alexithymia was higher than those with possible or no alexithymia. 33 Despite that medical literature has not established a clear influence of gender on alexithymia, a publication analyzing possible sociodemographic correlates in young adults reported alexithymia to be more prevalent in men, which contrasts with our data, where women presented a higher proportion of alexithymia. 34
With respect to disease severity and control, a publication addressing the impact of alexithymia on asthma management reported higher TAS-20 scores to be associated with decreased pulmonary function (p = 0.02) and worse asthma control score (p = 0.04). 30 This concurs with our results, where individuals with alexithymia had a higher proportion of severe disease as well as uncontrolled asthma than those with possible or no alexithymia. This is expected since alexithymia is a personality trait associated with poor emotional awareness and affect regulation, which, amid the setting of chronic disease, can be further conceived as the limited capability of properly recognizing symptoms. 35
As a matter of fact, in a publication involving 270 asthmatic patients during a severe attack, the authors concluded that alexithymic individuals do not recognize the physical and emotional factors during an exacerbation, which could possibly lead to a delay in seeking medical attention. 7 Such observation has also been reproduced in patients with acute myocardial infarction (AMI), where alexithymic patients show blunted perceptions in identifying AMI symptoms.36,37 Delaying medical attention and qualifying the treatment as unnecessary could possibly explain why half of the patients with alexithymia had severe asthma and why most of them were not controlled. It should be noted, however, that the differences in proportions of uncontrolled patients, between the alexithymic patients and those with possible or no alexithymia, were only slight. In part, this could be attributed to the fact that barely half of the patients had their asthma under control, meaning that poorly controlled asthma or uncontrolled asthma were a common trait in our sample, independently of TAS-20 score. Interestingly, the frequency of uncontrolled asthma was lower compared to what has been previously reported in Latin America by other studies.12,38
After understanding how the difficulty in identifying and communicating symptoms could be vital in asthma management, it is not surprising that Factors 1 and 2 in the TAS-20 questionnaire have been subject of interest for other research. For instance, in a publication involving patients with non-fatal asthma, authors concluded that the difficulty in both identifying and communicating feelings may be detrimental for asthma control. 6 In our study, individuals with severe disease and uncontrolled asthma had the highest mean scores in Factors 1 and 2. Such a concept can even be extrapolated to other diseases or medical conditions; for instance, in a publication involving 927 Japanese adults, difficulty identifying feelings scores in the third and fourth quartiles were more likely to present chronic pain than scores on the first quartile. 39 It would be safe to assume that since asthma control is deteriorated by the difficulty identifying symptoms and communicating them to physicians, patients with alexithymia should be more likely to present asthma exacerbations.
Finally, regarding treatment adherence, we found that roughly two-thirds of patients presented with some level of non-adherence; a finding that agrees with Latin American estimates on poor treatment compliance.12,40 Still, adherence to treatment remains a fundamental aspect for successful asthma control, which is still falling behind the goals set by international guidelines. 13 Further analyses revealed a statistically significant association between treatment adherence and asthma control, with uncontrolled asthma having the highest proportion for some level of non-adherence (p = .008). In this regard, while studies have clearly established the association between low levels of adherence to treatment and worse asthma control, the former can be the result of several factors, including mental disorders.9,41 In the case of alexithymia, it has been associated with lower treatment adherence due to poor communication between patients and healthcare providers. 42 However, we did not find any statistically significant associations between adherence and alexithymia, in which case the higher levels of low adherence might be related to the particular Latin American setting, where factors, such as socioeconomic status, cultural differences, and adverse effects might help to explain the finding. 12
Our study has several limitations. Namely, the study design was cross-sectional; thus, the reported results should only be interpreted as associations between alexithymia and the selected variables, where causality cannot be established. Disease severity was determined retrospectively under the consideration of the prescribed treatment and the step it belongs to. However, this method assumes that the asthma is under control, and since only half of our sample had controlled disease, it is likely that disease severity was underestimated in patients with uncontrolled or poorly controlled asthma. There was selection bias since the mean age in the studied sample was high, and alexithymia has been reported to be more prevalent with increasing age. 43 Moreover, since bronchial asthma in older individuals is more likely to be present in women, two-thirds of our sample belonged to such gender, which limits extrapolation of our findings to a population with equal gender distribution. 44 Concerning statistical methods, the assumption of normality was violated for some groups in the ANOVA test. Despite the robustness of the former analysis to non-normality, type I error might still be possible. To add, multiple comparisons/associations were carried, leading to an increase in familywise error and possibly type I error. Even though the Bonferroni procedure was carried as the post hoc analysis to adjust the mean comparisons, there was no adjustment for association/correlation analyses, for what we leave under the discretion of the reader the interpretation of statistical significance and the relative weight of the conclusions. Finally, we did not collected data on factors affecting individual behaviors (i.e. level of psychological distress, psychiatric comorbidities, or quality of life). However, one strength of the study is the considerable sample size (n = 265)., To our knowledge, this study is among the few to assess the frequency of alexithymia and its implications on asthma management in Latin American patients.
Conclusion
Our results suggest that in our sample 3 in 10 Latin American asthma patients have alexithymia, and such personality trait is more common in those individuals with lower educational levels. Patients with alexithymia present with severe asthma more frequently than do patients with possible or no alexithymia, and they are also more likely to have their disease uncontrolled. Such poor disease management is associated with some level of non-adherence. These findings can be explained, in part, due to the difficulty on identifying and describing symptoms, which leads to a low-quality communication between patients and physicians. The former statement is based on the high mean scores in Factors 1 and 2 observed in the context of severe and uncontrolled disease. Several questions are still unanswered regarding if alexithymia might be a causal factor for increased disease severity or poor management, as well as if psychotherapeutic treatment of alexithymia through medical counseling or group therapies can have a potential benefit in asthma control. Further prospective studies are required to answer such inquiries, which are of utmost interest in the Latin American setting where uncontrolled disease is the common denominator.
Supplemental Material
Supplemental_Appendix_Alexithymia_and_asthma_Latam_Rev_2 – Supplemental material for Influence of alexithymia on the management of Latin American patients with asthma: A cross-sectional study
Supplemental material, Supplemental_Appendix_Alexithymia_and_asthma_Latam_Rev_2 for Influence of alexithymia on the management of Latin American patients with asthma: A cross-sectional study by Emanuel Vanegas, Miguel Felix, German D Ramon, Orlando López Jove, Edgar Emilio Matos Benavides, Iván Tinoco-Morán, Jonathan A Bernstein and Iván Cherrez-Ojeda in SAGE Open Medicine
Footnotes
Acknowledgements
The authors thank the guidance and knowledge imparted by the MECOR Program for this study, especially from Sonia Buist, MD, Ana Menezes, MD, and Juliana Ferreira, MD. They also specially thank all the members of Respiralab Research Group. Finally, the authors express their gratitude to Universidad Espiritu Santo for their continuous support.
Author contributions
Authors have made substantial contributions to conception and design, acquisition, analysis, and interpretation of data and have been involved in drafting the article or revising it for critically important intellectual content. E.V. and I.C-O. designed and directed the study. G.D.R., O.L.J., E.E.M.B., and I.T-M. participated in the data recollection process. E.V. performed the statistical analyses and contributed to the interpretation of the results. E.V., M.F., J.A.B., and I.C-O. discussed the main findings and references to be included in the article. E.V., M.F., and J.A.B. contributed in the drafting and revision of the final version of the article. All authors read and approved the final version.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval and consent to participate
This study was performed in compliance with the World Medical Association Declaration of Helsinki on Ethical Principles for medical research involving human subjects and was reviewed by the Comité de ética e Investigación en Seres Humanos (CEISH) IRB. Ethical approval for this study was obtained from the ethics comittee “Comité de ética e Investigación en Seres Humanos” (CEISH), Guayaquil, Ecuador. (#HCK-CEISH-18-0060).
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was partially supported by an unrestricted grant from Universidad Espíritu Santo. The sponsor had no role in the design of the study or in the collection, analysis, and interpretation of data.
Informed consent
Written informed consent was obtained from all subjects before the study.
Data availability
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.