
Abstract
Background
The National Vital Statics defines neonatal birth trauma (NBT) as “an injury of the neonate’s body function or structure due to an adverse event that occurred at birth.” Neonatal birth trauma is usually discussed interchangeably with the term “birth injury,” which is used to describe minor skin lacerations to severe life-threatening conditions such as subgaleal hemorrhage, which is responsible for morbidity and mortality.1-4
NBT is a significant factor that increases the burden of morbidity and mortality. 5 For example, of the 2.4 million neonates who died in 2019, birth trauma accounted for 10% of deaths. 6 According to the 2018 World Health Organization (WHO) ranking report, NBT causes 0.13 to 33 per 100 000 population in low- and middle-income countries. 7 Deaths due to birth trauma accounted for 16.25 per 100 000 population in Ethiopia. 7 Moreover, NBT is a significant cause of short- and long-term deformities and disabilities. 8
The magnitude and risk factors for NBT vary from nation to nation; more importantly, it is determined by the availability of standardized obstetrical care. 9 For instance, the magnitude of the NBT ranges from 12.3% to 24.7% in Ethiopia.10,11 Studies have identified the factors associated with NBT in different countries. These risk factors can be classified into maternal, fetal, or obstetric complications and lack of poor obstetric care processes, such as lack of antenatal care follow-up, maternal diabetes mellitus, prolonged and obstructed labor, macrosomia, instrumental delivery, malpresentation, maternal age that is less than 16 or greater than 35 years, prematurity, skilled health professionals, low birth weight, malposition, oligohydramnios, and multiple pregnancies.3,12,13 Despite the Federal Ministry of Health in Ethiopia implementing interventions to decrease neonatal mortality and improve survival, less than half of the deliveries are conducted by skilled health professionals, and a high number of deaths are reported due to NBT.14,15
Although studies on the magnitude and risk factors for NBT among neonates exist, there is a paucity of data regarding NBT and its predisposing factors in eastern Ethiopia. Understanding the contextual risk factors for NBT helps in designing appropriate interventions to reduce the burden of NBT. Hence, this study aimed to investigate the magnitude and predisposing factors for NBT in public hospitals in eastern Ethiopia.
Methods and Materials
Study Setting, Design, and Population
A multicenter, cross-sectional study design was conducted among newborns admitted to the neonatal intensive care units (NICUs) of public hospitals in eastern Ethiopia. Hiwot Fana Comprehensive Specialized University Hospital (HFCSUH) is a teaching referral hospital of Haramaya University and Jugol General Hospital are located in Harar Town and serves more than 6 million people in eastern Ethiopia. Approximately 1900 neonates are admitted to the NICUs annually. Dilchora Referral Hospital and Sabina General Hospital are governmental hospitals located in Dire Dawa, serving more than 1 million people. Approximately 1200 neonates are admitted to the NICUs per year. All neonates who were admitted within 28 days of neonatal life to the NICUs from April 1 to June 30, 2022, were included. However, neonates born at less than 28 weeks of gestational age and with major congenital anomalies were not included in this study.
Sample and Sampling Procedure
The sample size was calculated using EPI-Info version 7.2.5 software with the following assumptions: the proportion for the residential distance from health facilities (exposed) was 46.6%, and power was 80% with a 95% confidence interval (CI). 11 A 10% was added for the nonresponse rate. Then, the final sample was 492. The calculated sample was proportionally allocated to the selected hospitals following the estimated patient flow on admission for the previous 3 months (January to March 2022) in all four selected hospitals (n = 1030) as the sampling frame, and a systematic random sampling technique was used to select participants from each hospital with every kth value = 2 to select the final sample (n = 492).
Data Collection
We collected the data using a structured interviewer-administered questionnaire that was adopted from different literature and a pretested structured validated data abstraction checklist.16-18 The checklist contains information on the sociodemographic conditions of the mother and neonate, obstetric factors, treatments received, and neonatal status. Neonatal birth trauma was defined as neonates with one of the physical injuries during the birth process that was evaluated by physicians or clinicians on admission and admitted with at least one of the following diagnoses: extracranial trauma, cephalohaematoma, subgaleal hemorrhage, musculoskeletal injuries, neurological trauma, brachial palsy, Kulmpke’s palsy, soft tissue injury, and abdominal visceral injury.17-19 Perinatal asphyxia is defined as clinical evidence of neonate failure to initiate spontaneous breathing, the need for resuscitation after birth, an Apgar score of less than 7 at the 5th minute, or neonates with clinical evidence of hypoxic encephalopathy. 36 Birth weight was categorized as low, normal, or large if birth weight was <2500 g, 2500 to 3999 g, and ≥4000 g, respectively. 35 Gestational age was classified as early preterm (less than 34 weeks) “preterm” if delivery was before 37 complete weeks of gestation, “term” if the baby was born at 37 to 42 completed weeks of gestation, and “post term” if the baby was born after 42 completed weeks of gestation.
Data Quality Management
The questionnaire was pretested on 5% of the sample at Haramaya General Hospital, which was not included in the final analysis. Moreover, data collectors and supervisors were trained for two days. The overall data collection process was closely supervised, and the completeness of each questionnaire was checked daily. During data cleaning, we applied a logical checking technique to identify errors. Finally, we performed double data entry to countercheck the data consistency.
Data Processing and Analysis
Data were entered into Epi data version 3.1 and analyzed using Statistical Package for the Social Sciences (SPSS) version 26.0. We described the characteristics of the participants using tables, figures, and text. We applied a binary logistic regression model to determine the predisposing factors associated with NBT. Variables with P values ≤.25 in the bivariable analysis were transferred into the multivariable analysis to control for confounding factors. We tested the goodness of fit of the model using the Hosmer–Lemeshow test (>0.05). A multicollinearity test was performed to determine the correlation between independent variables using variance inflation factors (VIF > 10). The adjusted odds ratio (AOR) with a 95% CI and a P value <.05 were considered statistically significant.
Ethics Approval and Consent to Participate
This study was performed according to the Declaration of Helsinki. We conducted this study after ethical clearance from the Haramaya University College of Health and Medical Science Institutional Health Research Ethical review committee (IHRERC) (Ref. no: IHRERC/065/2022). Then, an official letter of cooperation was sent to each hospital. Written informed consent was obtained from all parents of the newborns. The participants’ information was kept confidential.
Results
Maternal Sociodemographic Characteristics
Four hundred ninety-two neonates with mothers participated in this study, with a 100% response rate. The mean and SD for maternal age was 24.12 ± 4.61 years. Of these, 189 (38.4%) mothers were aged 20 to 24 years, and 138 (28%) were 25 to 29 years. Four hundred sixteen (84.6%) participants were married. Two hundred seventeen (44.1%) mothers had no formal education. The mean and SD body mass index (BMI) and height of the mothers were 20.2 ± 2.49 SD kg/m2 and 1.63 ± 0.08 SD meters, respectively. Nearly half (54.7%) of the mothers were urban dwellers (Table 1).
Socio-Demographic Characteristics of Mothers Whose Neonates Admitted to NICUs at Public Hospitals in Eastern Ethiopia, 2022 (n = 492).

Maternal Obstetric and Medical-related Characteristics
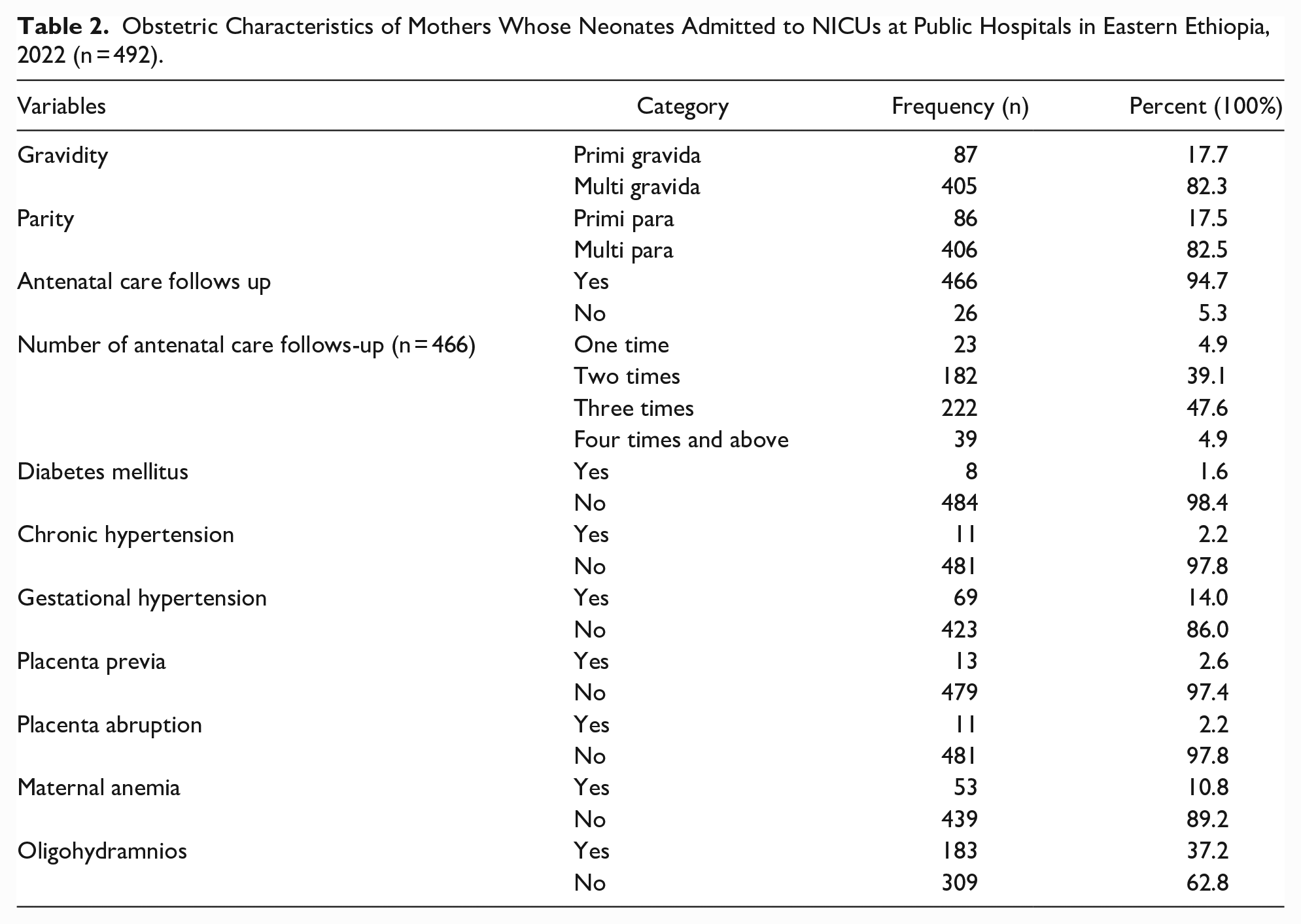
Of the total, 406 (82.5%) mothers were multiparous. Four hundred sixty-six (94.7%) mothers had antenatal care follow-ups, and of these, 39 (4.9%) had at least 4 antenatal care visits. Regarding the medical illness of the mothers, 183 (37.2%) mothers had oligohydramnios, 69 (14.0%) had pregnancy-induced hypertension, and 53 (10.8%) were anemic (Table 2).
Obstetric Characteristics of Mothers Whose Neonates Admitted to NICUs at Public Hospitals in Eastern Ethiopia, 2022 (n = 492).
Intrapartum-Related Characteristics
Four hundred nineteen mothers (85.2%) gave birth in the hospital, while only 26 (5.3%) mothers were delivered at home. Three hundred ninety-nine laborers were followed using a partograph. Vertex fetal presentations accounted for 387 (78.7%) deliveries, and 255 (51.8%) deliveries were spontaneous vaginal deliveries. The study showed that the prolonged duration of labor was 180 (36.6%), while normal labor was 312 (63.4%). Seventy (14.2%) deliveries were assisted with a vacuum, whereas 58 (11.8%) were assisted with forceps. Three hundred nine (62.8%) deliveries were attended by midwives (Table 3).
Intrapartum-Related Factors of Mothers Whose Neonates Admitted to NICUs at Public Hospitals in Eastern Ethiopia, 2022 (n = 492).

Neonatal-Related Characteristics
Of the total admitted neonates, 420 (85.4%) were an early neonatal age. The mean ± SD of gestational age was 36.98 ± 2.31 weeks, and the mean ± SD of birth weight was 2801 ± 789 g. The head circumference of 212 neonates (43.1%) was measured at less than 32 cm. There were 317 (64.4%) male neonates. Approximately 283 (57.5%) newborns had a first-minute Apgar score between 4 and 7, and 20 (4.1%) had a score less than 3 (Table 4).
Neonatal-Related Characteristics of Neonates Admitted to NICUs of Public Hospitals in Eastern Ethiopia, 2022 (n = 492).

Magnitude of NBT
The overall magnitude of NBT was 83 (16.9%) (95% CI: 13.7-20.5%). The common types of NBT were extracranial trauma (73, 88%), soft tissue trauma (58, 69.9%), musculoskeletal trauma (16, 19.3%), and neurological trauma (12, 14.5%). Extracranial trauma: Forty (48.2%) neonates were diagnosed with cephalohaematoma. Twenty-three (27.7%) neonates had subgaleal hemorrhage. Among soft tissue traumas, facial and skin bruises accounted for 18 (21%). Of the neurological traumas, facial palsy occurred in 5 patients (6%) (Table 5).
Types of NBT Among those Admitted to NICUs at Public Hospitals in Eastern Ethiopia, 2022 (n = 492).

Others: organ injuries in the abdomen and others.
Predisposing Factors for Neonatal Birth Trauma
Regarding predisposing factors, in the multivariable binary logistic regression analysis, NBT was associated with facility-based delivery, instrumental delivery, fetal presentation, early preterm birth, birth weight (>4000 g), and male sex. Neonates who were delivered through instrumental delivery were 7.4 times (aOR = 7.40; 95% CI: 3.25-16.80) more likely to suffer from NBT than caesarian-delivered newborns. Newborns delivered in early preterm (<34 weeks) were 3.5 times (aOR = 3.5; 95% CI: 1.34-9.04) more likely to have birth trauma than term neonates. Macrosomia neonates had a 3.65-fold (aOR = 3.65; 95% CI: 1.42-9.41) increased risk of NBT compared to normal birth-weight babies. Furthermore, face presentations were 4.1 times (aOR = 4.1; 95% CI: 1.37-12.25) more likely to have neonatal birth injuries compared with their counterparts. Being a male neonate was 2.14 times (aOR = 2.14; 95% CI: 1.14-4.02) higher risk for NBT compared with female. However, neonates delivered in hospitals (aOR = 0.19; 95% CI: 0.062-0.57) and health centers (aOR = 0.96; 95% CI: 0.022-0.42) were less likely to suffer from NBT than home-delivered newborns by 81% and 4%, respectively (Table 6).
Factors Associated With Neonatal Birth Trauma Among Neonates Admitted to NICUs at Public Hospitals in Eastern Ethiopia, 2022 (n = 492).

Abbreviations: COR, crude odds ratio; AOR, adjusted odds ratio; NBT, neonatal birth trauma.
Statistically significant in COR. **statistically significant in aOR at P-value ≤ .05.
Discussion
NBT is among the top 10 causes of neonatal morbidity and mortality. 5 The morbidity and mortality rates of neonates with birth trauma vary worldwide. Obstetric and neonatal services that are provided during antenatal care, delivery, and admission are crucial to reducing the burden of NBT. Therefore, this study aimed to investigate the magnitude and predisposing factors for NBT in public hospitals in eastern Ethiopia.
In the present study, the magnitude of NBT was 16.9% (95% CI: 13.7-20.5%). This finding is in agreement with the finding from Jimma, Ethiopia (15.4%). 10 However, it is slightly higher than other studies in Addis Ababa Ethiopia (12.3%), 11 (9%) 20 , and India (11.76%). 21 Moreover, the present finding was significantly higher than many studies conducted in Finland (1.6%), 9 India (1.54%), 22 Bangladesh (4.9%), 23 Australia (2.2%), 24 Pakistan (4.11%), 14 Iran (2.2%), 17 (2.7%), 25 Cameroon (1.84%), 16 Western Iraq (1.74%), 8 and Ghana (3.66%). 13 The possible justification for variations in the magnitude of NBT in the current study might be the different in the sample size, study setting (ie, the current study was conducted in a multicenter facility-based study), the infrastructure of health care facilities, skills of birth attendants to attend labor and delivery process, duration of the study period, and inclusion home-based delivery.
However, this study finding is lower than the studies carried out in different countries such as Southern Ethiopia (24.7%), 19 Southwest Nigeria (67.2%), 16 Israel (24.3%) 26 , and the United States (23%). 18 The possible reasons might be variations in sample sizes (ie, in Nigeria’s study, 134 of 90 (67.2%) participants had birth trauma), the experience of health personnel, and data coverage, such as a nationwide survey. It may also be related to variations in the diagnosis of birth trauma and maternal and neonatal care during the delivery process in these countries.
In the present study, the predisposing factors significantly associated with NBT were facility-based delivery, instrumental delivery, fetal presentation, early preterm birth, birth weight (>4000 g), and male sex. Neonates delivered by instrumental delivery were 7.40 times more likely to suffer from birth trauma than those delivered by the caesarian section. The current finding is supported by other studies in different countries, such as Ethiopia,10,11,27 India 22 Nigeria, 28 and Pakistan. 29 This might be related to the application of instruments such as forceps and/or vacuum on the fetal head during delivery, which may expose it to NBT.
Moreover, malpresentation was 4.1 times more likely to increase the risk of NBT than normal vertex presentation. This is because malpresentation exposes newborns to birth injuries compared with normal presentations during delivery. This finding is in line with studies conducted in different settings, such as Ethiopia,10,11 America 2 , and India. 30 Likewise, places of delivery such as hospitals and health centers reduce the risk of NBT by 81% and 4% when compared to home delivery, respectively. This result is in agreement with a study finding in Ghana 13 that home-delivery neonates were more affected by NBT than hospital and health center deliveries.
Furthermore, gestational age at birth as early preterm was more likely to be exposed to NBT than term gestational age. This study was supported by other studies in Iraq, 17 Southwest Nigeria, 16 Pakistan 14 , and Iran. 30 This is because preterm neonates are physically and physiologically immature, which exposes them to extracranial brain hemorrhage.
In the current study, neonates who delivered with a birth weight greater than 4000 g had a 3.65 times higher risk of NBT than normal-weight babies. The present finding is in agreement with studies in different settings, such as Ethiopia, 20 Tanzania, 31 India, 32 Pakistan, 30 Indonesia 33 , and Nigeria. 16 This is because a large baby is difficult to deliver via spontaneous vaginal delivery and is traumatized by instrumental devices during health workers’ assistance. In addition, male neonates were 2.14 times more likely to suffer from NBT than female newborns. This association is supported by other studies in Iran 17 and Enugu Nigeria. 34
Limitations
Our study has some limitations. First, an institutional-based study is not generalizable to the entire population. Second, the study was conducted in hospitals that had too many neonatal admissions, which might overestimate the magnitude of NBT. Third, the present study was cross-sectional in design and did not indicate a cause-effect relationship.
Conclusions
The magnitude of the NBT was relatively high. Facility-based delivery, instrumental delivery, malpresentation, gestational age less than 34 weeks at birth, birth weight (>4000 g), and male sex were predisposing factors independently associated with NBT. Promoting health facility-based delivery, the prevention of preterm birth, intrauterine weight estimation, and early decisions to minimize instrumental deliveries are important to reduce the burden of NBT. Ministry of Health, regional health offices, and healthcare providers should give attention to NBTs.
Footnotes
Acknowledgements
We thank Haramaya University for its technical support. We would also extend our gratitude to the head and staff of Hiwot Fana Comprehensive Specialized University Hospital, Jugol Hospital, Dilchora Referral Hospital, and Sabian Primary Hospital, study participants, data collectors, and the supervisor for their collaboration.
Author Contributions
GT, AD, and NA conceived and designed the study. MK drafted the manuscript. AD, NA, AAL, and MK extensively reviewed the manuscript and incorporated intellectual input. All authors read, provided feedback, and approved the final version of the manuscript.
Availability of Data and Materials
All data of this study are available from the corresponding author upon reasonable request.
Consent for Publication
Not applicable
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by Haramaya University, Ethiopia. This organization had no role in study selection, data collection, analysis, conclusion, and interpretation.