
Abstract
The interplay between Adverse Childhood Experiences (ACEs) and resilience on health in children is not well understood. Parents completed 3 questionnaires: ACEs, Child and Youth Resilience Measure (CYRM), and the Pediatric Symptom Checklist-17(PSC-17). BMI and blood pressure were measured. 19.8% of children had 4 or more ACEs, resilience ranged from 25 to 51, 14.3% had a positive PSC-17 score, 25.6% were obese, 3.1% had systolic hypertension, and 1.2% had diastolic hypertension. Higher ACEs (ACE OR: 1.398, 95% CI = 1.044-1.893, P = .026) and lower resilience (Resilience OR: 0.740, 95% CI 0.668-0.812; P = 1.13 × 10−9) were predictive of increased reports of behavioral health symptoms, but not obesity or hypertension. The personal resilience subscale was a predictor of positive PSC-17 score (OR 0.646, 95% CI = 0.546-0.749, P = 3.18 × 10−8); relationship subscale was not. Cultivating resilience, especially personal aspects, may provide an effective intervention for behavioral health symptoms in children.
Introduction
Adverse Childhood Experiences, or ACE’s, are traumatic events in a child’s life that can continue to have an impact on their health into adulthood.1-4 A score of 4 or more ACE exposures is often considered a critical threshold that has been shown to affect health.1,5,6 While initial research focused more on the negative physical and mental health diagnoses that manifest in adults, a growing body of research has shown effects may be evident even in childhood. 7 One systematic review found that most studies show an association between ACEs and childhood obesity and multiple ACES may cause a greater obesity risk. 8 Another longitudinal study found a significant association with 4 ACES experienced in early childhood and increased risk of obesity at age 11 years old. 9 Research examining the association among ACEs and behavioral and mental health outcomes in children has found ACE exposure was associated with long-term behavioral health problems, almost quadrupling internalizing and externalizing symptoms. 10 Children with greater ACE exposures have also been shown to have higher reports of attention problems, social problems, and aggression when evaluated by their kindergarten teachers. 11 Additionally, Kerker et al 12 found that for each additional ACE reported, the odds of a child having an abnormal score on a behavioral health symptom checklist increased by 32%. Of note, much of this behavioral health data has come from large national survey data sets of children already known to have trauma exposure, such as involvement with the child welfare system, as opposed to a cross sample of the general population.
In spite of this shown association between ACEs and health problems, not every child exposed to ACEs shows detrimental outcomes. The concept of resilience, defined by Windle et al 13 as “the process of negotiating, managing, and adapting to significant sources of stress or trauma,” has been proposed as a protective counter to the trauma of ACEs. Resilience is a dynamic process that can be learned and strengthened over time. Several factors have been found to promote resilience, some external, like a stable relationship with an adult caregiver, and positive cultural and faith traditions, while others are more internal concepts like building belief in one’s own capacity, and developing self-regulation and executive functioning skills.14-18 While it is thought that higher levels of resilience can counteract some of the negative effects of ACEs, the interplay between ACEs and resilience is still not very well understood. Because resilience is a multifaceted, more abstract concept, it can be challenging to measure in a standardized way making research in the area difficult. Fewer studies have examined resilience and health outcomes in children than have been done on ACEs and health outcomes. A systematic review of resilience and mental health found higher levels of resilience were related to fewer mental health problems, however, they did note difficulty with heterogeneity in the different instruments used to measure resilience as well as the study populations. They also noted the need for more longitudinal studies as resilience is a dynamic process. 19 One cross sectional study found if there were higher levels of family resilience, there were decreased odds of being in a higher weight category, despite having ACEs exposure. 20 Another study using National Survey of Children’s Health data found higher levels of resilience was associated with decreased risk of obesity. 21
The objective of this study was to investigate how ACEs and resilience impacted real-time parental reports of behavioral health symptoms as well as physical health measures in school aged children in an urban, underserved primary care pediatric population. Studying the interplay between resilience and ACEs informs how children respond and adapt to stressors and provides a framework for building better interventions for children and their families.
Methods
The Child and Youth Resilience Measure (CYRM) is a validated measure of individual, relational, communal, and cultural resources available to a child that are associated with increased resilience.23,24 The tool was developed in communities encompassing 11 different countries and languages. While initially developed as a tool for older youth it has been adapted as a parent report tool for younger children with 17 items included. A three-point scale was used with a minimum score of 17 and a maximum score of 51. The tool provides a total resilience score as well as 2 subscales. The personal subscale includes items like the child can finish what they start, they know what they are good at, and they can respond in positive ways when things don’t go their way. The relationship subscale includes items like does their caregiver provide for physical and emotional needs and does the child feel supported at home, at school, and in their community. While there are no reference cutoffs, higher scores are considered to infer higher resilience.
In addition to the completed surveys body mass index (BMI) and blood pressure data was also collected from the well visit vital signs. BMI greater than 95th% was classified as obese. 27 Systolic or diastolic blood pressure greater than 95th%, based on age, sex, and height, was classified as elevated blood pressure. 28
Results
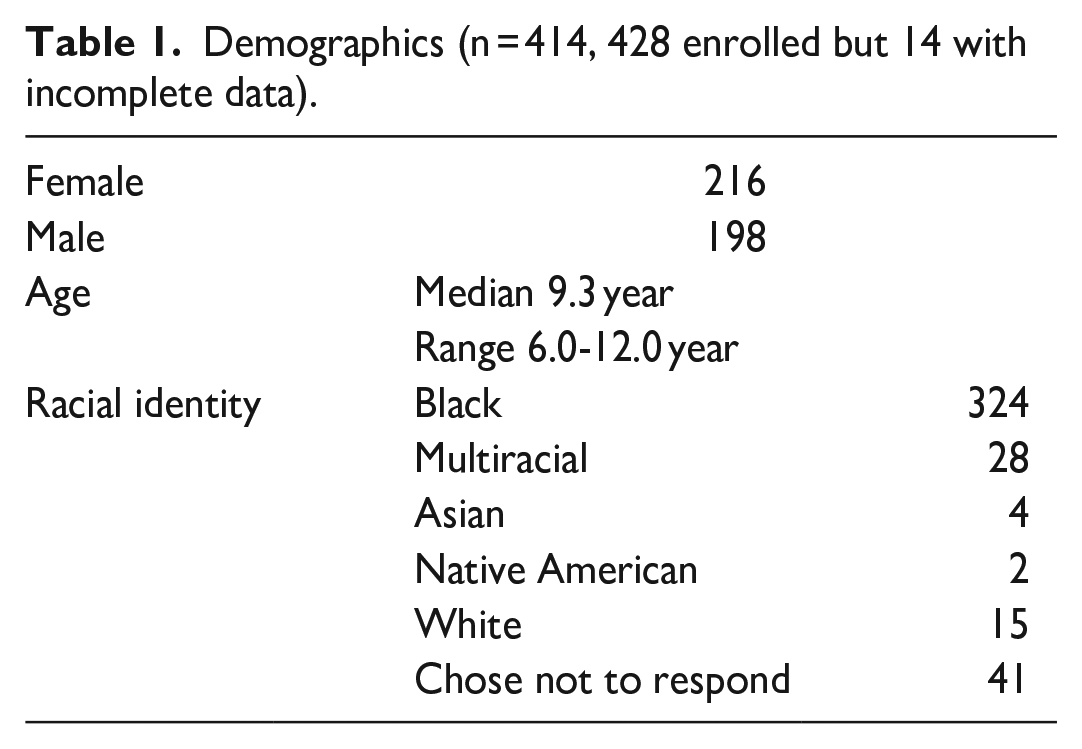
Four hundred twenty-eight children were enrolled with 14 excluded due to incomplete data, leaving 414 included for analysis. Two hundred sixteen participants identified as female, and 198 identified as male. They ranged in age from 6.0 to 12.0 year old with a median age of 9.3 years. Three hundred twenty-four identified as black, 28 identified as multiracial, 4 identified as Asian, 2 identified as Native American, 15 identified as white, and 41 chose not to respond (Table 1).
Demographics (n = 414, 428 enrolled but 14 with incomplete data).
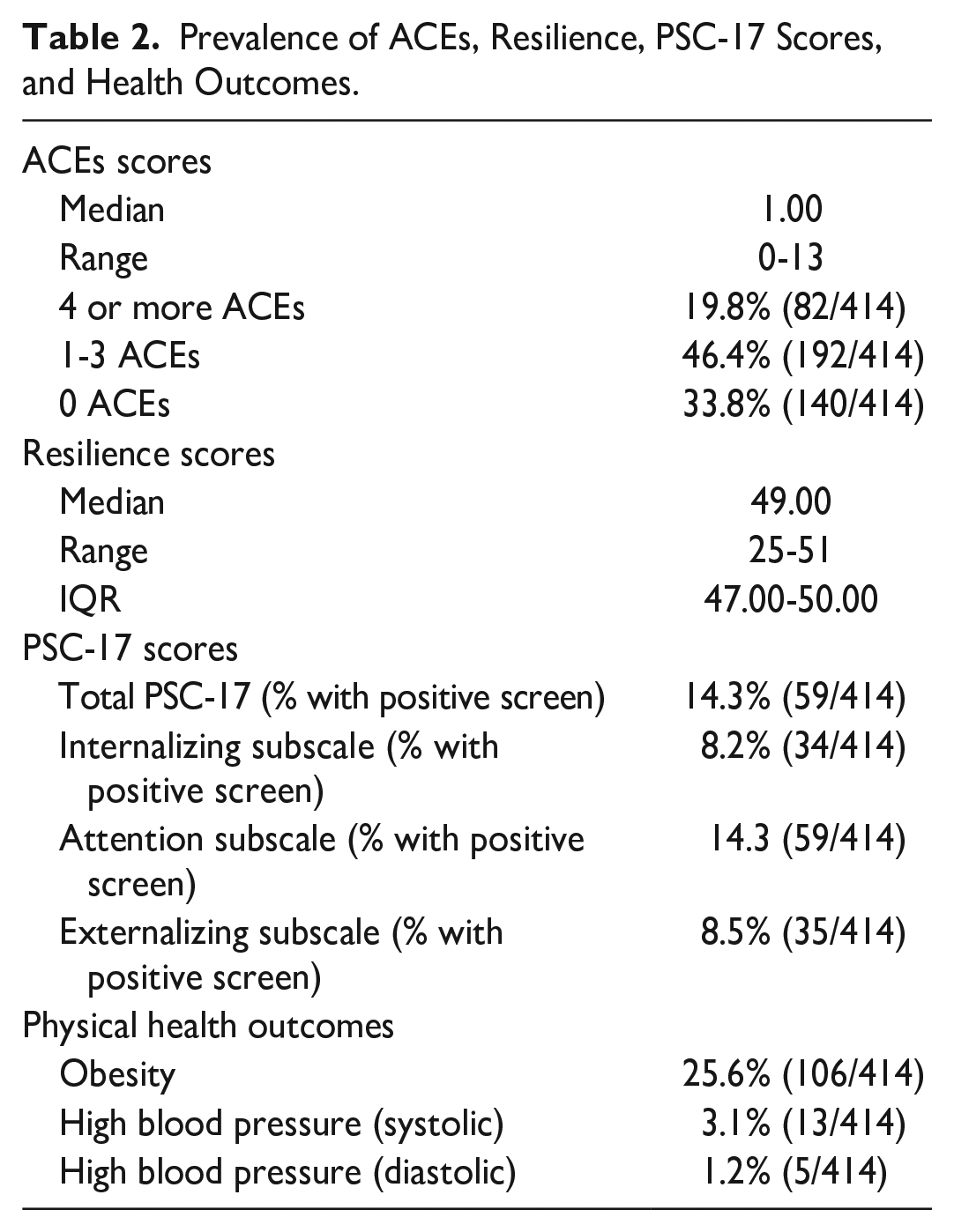
ACE scores ranged from zero to 13 with a median of 1.00. 19.8% of children (82/414) had total ACE scores of 4 or higher while 46.4% (192/414) had 1 to 3 total ACEs and 33.8% (140/414) reported zero ACEs. Resilience scores ranged from 25 to 51 with a median of 49.0 and an IQR of 47.0 to 50.0. 14.3% (59/414) of children had a positive PSC-17 score; 8.2% (34/414) had significant internalizing scores, 14.3% (59/414) had significant attention scores, and 8.5% (35/414) had significant externalizing scores. 25.6% (106/414) of children met criteria for obesity, 3.1% (13/414) met criteria for hypertension based on systolic blood pressure and 1.2% (5/414) met criteria based on diastolic blood pressure. (Table 2)
Prevalence of ACEs, Resilience, PSC-17 Scores, and Health Outcomes.
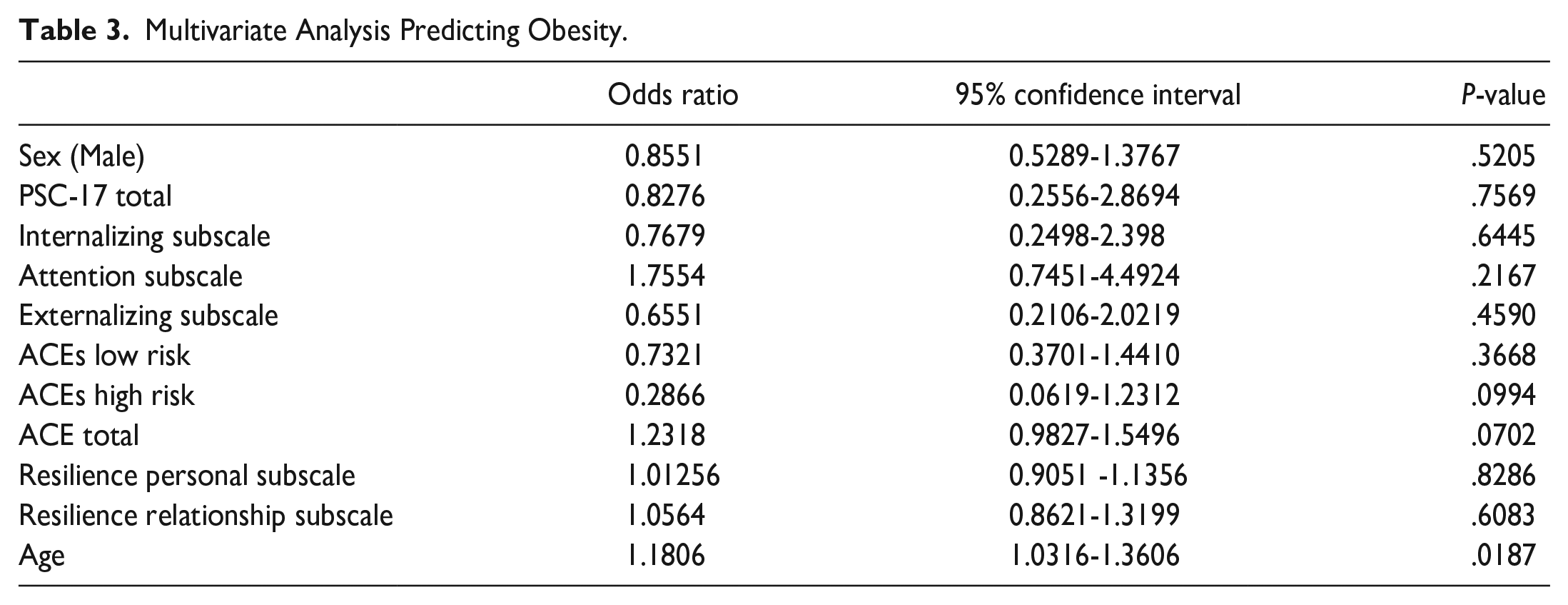
Physical health outcomes were examined individually in a multivariate analysis with age being the only predictor of obesity (OR 1.181, CI 1.032-1.361; P = .0187). (Table 3) There were no significant predictors of elevated blood pressure. Multivariate analysis was also done with a combined health outcome, including obesity and elevated blood pressure, and age was the only significant predictor (OR 1.185, CI 1.039-1.359, P = .013). ACEs and resilience were not predictors of either the individual physical health outcomes or a combined health outcome. (Table 4) Total ACE score and total resilience score were significant predictors of positive PSC-17 scores (ACE OR: 1.398, 95% CI = 1.044-1.893, P = .026; Resilience OR: 0.740, 95% CI 0.668-0.812; P = 1.13 × 10−9). Male sex was also a significant predictor of a positive PSC-17 score (OR: 2.816, 95% CI 1.39-5.94, P = .005). The personal resilience subscale was a significant predictor of a positive PSC-17 score (OR 0.646, 95% CI = 0.546-0.749, P = 3.18 × 10−8) while the relationship subscale was not significant. (Table 5) The PSC-17 subscales, internal, external, and attention were also examined in multivariate analysis with resilience being a significant predictor of all 3 subscales (internal: OR 1.414, CI 1.244-1.634; P = 5.33 × 10−7; external: OR 1.298, CI 1.181-1.440; P = 2.06 × 10−7; attention: OR 1.108, CI 1.024-1.199; P = .010). ACEs were found to be a significant predictor of only the internal subscale (OR 0.715, CI 0.505-0.998; P = .05). Male sex was a significant predictor of the attention subscale (OR 0.361, CI 0.187-0.674; P = .00174) (Table 6).
Multivariate Analysis Predicting Obesity.
Multivariate Analysis Predicting Physical Health Outcomes (obesity and high blood pressure combined).

Multivariate Analysis Predicting Negative Total PSC-17 Score (low risk).

Multivariate Analysis Predicting PSC-17 Subscales.

Discussion
Higher ACE scores as well as lower total resilience scores were independently associated with increased reports of total behavioral health symptoms. Previous literature has shown higher exposure to ACEs can lead to dysregulation of the autonomic nervous system, or fight or flight response, as well as cause changes in areas of the prefrontal cortex, the part of the brain responsible for executive functioning, decision making, self-regulation, and impulse control.29-34 These brain changes could lead to less constructive coping mechanisms manifested in internalizing, externalizing, and attention behavioral health symptoms. Lower resilience can be indicative of dysregulation in how a child reacts to situations, for example acting out in destructive ways or quitting. If there is a lack of external support around that child, another component of resilience, they also likely aren’t seeing modeling and receiving guidance on how to cope with these feelings and respond to them in healthier ways. In addition, if the parent also had high ACEs exposures and low resilience they may be lacking in their own coping and regulation skills.
Male sex was also associated with a positive behavioral health screen. Validation of the tool does not show any difference in sex, however, some literature has shown sex differences in risks of symptoms, with boys being higher risk for externalizing and attention symptoms and girls being higher risk for internalizing symptoms. 35 Additional studies have shown sex differences in the way ACEs can impact the development of self-control and impulsivity. 36 The symptom checker is parent-report so it’s possible that more disruptive symptoms like externalizing and attention symptoms, which can be more common in boys, are more noticeable and therefore reported more often than less noticeable internalizing symptoms, which can be more common in girls.
The personal resilience subscale was found to be a significant predictor of a positive behavioral health screen while the relationship subscale was not significant. The personal resilience subscale examines qualities like a child being able to finish what they start without quitting, being able to fix things when they don’t go their way without being destructive, and knowing the areas in which they excel. In our previous research, the relationship with their caregiver seemed to be a primary driver of the protective nature of resilience in adolescents. 37 In the adolescent age group the resilience questionnaire is self-report while in the school-age group it is a parent report tool. In this younger age group there may be reporting bias as a parent is commenting on their own perception of their caregiving relationship with their child. This may make it more difficult to fully assess how a younger child feels about the supportive relationships around them. Having a safe, stable caring adult is still absolutely important in younger elementary school aged children, however, interventions focused on cultivating some of these personal resilience attributes may be more beneficial in helping with behavioral health symptoms in this age group.
ACEs and resilience were not predictors of either obesity or elevated blood pressure. There were low numbers of children who met criteria for elevated blood pressure, therefore low incidence in younger children likely plays a role, however, around a quarter of children were classified as obese. Age was found to be the only significant predictor of obesity, so the older the child, the more likely to have an abnormal health outcome. These physical health markers may not show significance until adolescence or even later, as found in The Georgia Stress and Heart Study. They found individuals with multiple ACEs noted in childhood were noted to have a faster rise in BP levels than those without ACEs, but this was not seen until after 30 years old. 38
Analysis of the behavioral health subscales showed that resilience was a predictor for all the subscales with higher resilience being associated with lower likelihood of significant internalizing, externalizing, or attention symptoms. ACEs were only a significant predictor for the internalizing subscale. With smaller numbers of participants significant for each subscale, caution should be used when making conclusions, however, it would still be important to consider that resilience may be more useful to examine and target as intervention for behavioral health in children rather than using ACEs alone as a marker.
Our study does have limitations. As mentioned earlier, the questionnaires are parent-report so reporting bias must be considered. Certain behaviors that are more disruptive may be over reported while those that are subtler may be underreported. A parent’s own ACE exposure and resilience could also affect their own coping mechanisms and how they perceive different behavioral health symptoms in their child. Selection bias is also a limitation to consider. Parents who chose to participate may have been concerned about their child’s behavioral health symptoms. Parents of children who have experienced a high number of ACEs may opt to not participate due to the sensitive nature of traumatic experiences. In addition, our patient population is a fairly homogenous urban underserved community, therefore these relationships may not hold in different demographics. This data also looks at one point in time, while resilience has been shown to be a dynamic process over time. Follow up in 1,5, 10, or even 15 years would give more robust information on the dynamic nature of resilience.
We used a validated resilience screen with no normative cutoffs while a lot of literature has shifted to using positive childhood experiences, or PCE scores, that mirror the ACE scores with their critical cutoff values. PCEs, which were actually adapted from the CYRM, have been introduced to express a similar idea of a positive counter to the negative impacts of ACEs. 39 Both resilience and PCEs stress the importance of a supportive family, supportive peer relationships, and a sense of belonging in the community, aiming to shift to a more holistic view of health that is not just living in the absence of disease but thriving.40,41 Using PCEs could assist in building a larger more uniform body of literature on positive counters to the toxic stress of ACEs, however, it is not clear if resilience and PCEs are measuring the same outcome. Future research could further examine if both resilience and PCEs are predictors of the same outcomes.
Conclusions
Our findings serve to add further support to the literature showing higher ACE exposure is associated with higher behavioral health symptoms in children. In addition, it adds that higher levels of resilience are associated with lower reports of behavioral health symptoms. This data is from parent real-time report in a primary care setting as opposed to some of the other literature that has extrapolated from national survey data sets of children already known to have trauma exposure. In addition, enhancing the personal attributes of resilience may be effective in improving behavioral health symptoms in this age group, as opposed to what we found in adolescents where the relationship with their caregiver was a primary driver. This suggests that interventions to build resilience may need to focus on different facets of these protective counters to the toxic stress of ACEs, depending on the child’s age.
Footnotes
Acknowledgements
We acknowledge the support of the Temple Pediatrics clinic staff.
Author’s Contributions
AH and SA designed and developed the study. XW, MB, EK, EH, AL, PM, and ZS acquired and managed data and contributed to data analysis. SA analyzed data and SA and AH interpreted data. AH and SA drafted the manuscript and XW, MB, EK, EH, AL, PM, and ZS contributed to the final manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics Approval and Consent to Participate
This study was approved by the Temple University IRB (Protocol 24871). Parental written informed consent was obtained for all children participating. All methods were carried out in accordance with relevant guidelines and regulations.
Consent for Publication
Not applicable.
Availability of Data and Materials
The datasets used and analyzed during the current study are available from the corresponding author on reasonable request.