
Abstract
Hydatid disease is a zoonosis caused by a larva of the tapeworm Echinococcus. All organs can be involved, but it is frequently located in liver for adults and lung for children. The clinical features are nonspecific. Imaging findings has an important place in the diagnosis and the follow-up. Rupture is the most common complication of a hydatic cyst and has a variety of imaging findings depending on the ruptured layer, the amount of air within the cyst and the type rupture. We report the case of a 10-year-old boy presenting shortness of breath and fever among other symptoms revealing by chest X-ray and thoracic CT scan, a lung ruptured hydatic cyst to the pleural cavity causing a tension hydro-pneumothorax and a superadded infection.
Introduction
Hydatid disease is a zoonosis that mostly causes cystic lesions which can be simple or complicated. The most common complication is the rupture of the cyst layers, responsible for a variety in the clinical and the radiological features, hence the importance of knowing some characteristic radiological signs that makes the diagnosis more accurate. We present a case report of a tension hydro-pneumothorax caused by the rupture of hydatic cyst in the pleural cavity complicated with superadded infection.
Case Report
A 10-year-old boy who lives in a rural area and had no medical history, was admitted to the emergency department for shortness of breath, coughing, vomiting and abdominal pain evolving for 1 month. These symptoms worsened in the couple of days before his consultation with the onset of fever. The general physical examination found a conscious patient with a high respiratory rate 37 cpm, pulmonary examination suspected a pleural effusion in the left lung.
Laboratory test result showed white blood cell count (WBC) 16 300/mm3, C-reactive protein 109 mg/dl, hydatid serology ELISA test 31,55 DU and indirect hemagglutination test positive at 1/2560.
Chest X-ray revealed a hydro-pneumothorax with a mass effect on the trachea and mediastinum pushed back to the contralateral side (Figure 1).

Chest X-ray revealed a hydro-pneumothorax with a level air fluid, a mass effect on the trachea and mediastinum pushed back to the contralateral side.
An abdominal ultrasound revealed the presence of a cystic lesion in the liver suggesting an hydatic cyst (Gharbi 1).
A thoraco-abdominal computed tomography (CT) scan showed a pulmonary hydatic cyst ruptured in the pleural cavity. The cyst in the left lung, contains floating membranes and air, making the appearance of “whirl sign.” Large hydropneumothorax containing floating membranes, thickness of the pleural wall with a contrast uptake. Collapse of the entire left lung and rightward mediastinal shift deviation (Figure 2a and b). No other lesions were found except an uncomplicated hydatic cyst in the liver.
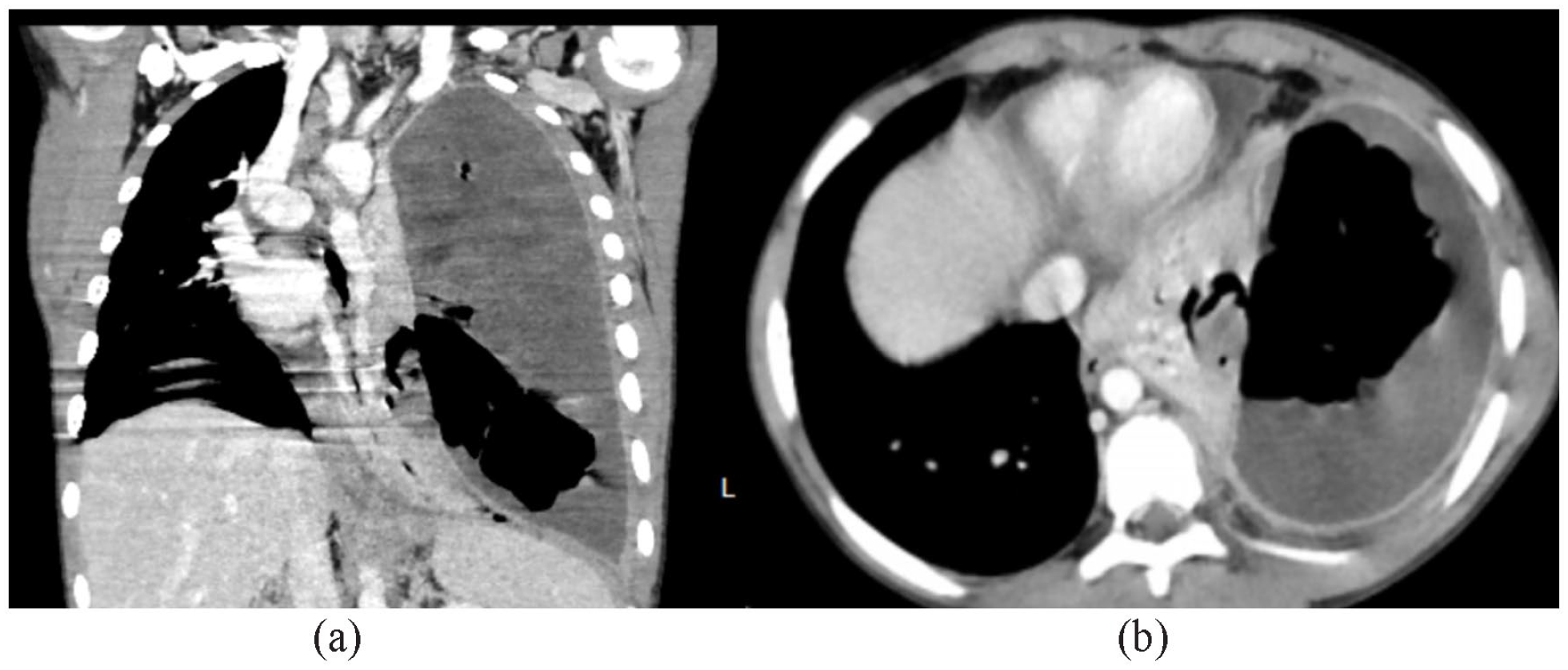
Coronal (a) and axial (b) CT images C+ venous phase: cyst containing floating membranes and air “whirl sign.” Large hydropneumothorax containing floating membranes, thickness of the pleural wall with a contrast uptake. Collapse of the entire left lung and rightward mediastinal shift deviation.
The patient received intravenous antibiotics, cephalothin and gentamycin, and was programed for a thoracoscopy procedure that revealed a pleural-thoracic empyema, the presence of the germinative membrane, a collapsed left lung and a bronchopleural fistula. The procedure consisted on the removal of the germinative membrane, the evacuation of the infected pleural fluid, and positioning a chest tube in pleural cavity.
Follow-up procedures were marked by the improvement of the patient’s respiratory condition and disappearance of the fever. Chest X-ray was preformed after the procedures revealed size regression of the hydropneumothorax (Figure 3).

Post-operative chest X-ray regression of the hydro-pneumothorax size, a collapsed left lung but no mass effect on the mediastinum or the contralateral lung, chest tube in the pleural cavity.
Discussion
Hydatid disease is a zoonosis caused by a larva of the tapeworm Echinococcus. All organs can be involved, but it is frequently located in liver for adults and lungs for children. 1
The hydatic cyst contain 2 layers, an outer though layer (pericyst) and an inner membrane of germinal epithelium (endocyst), and has within a clear fluid. 2 Rupture is the most frequent complication due to several factor (age, defense mechanism of the host, chemical reactions) that are responsible for the degeneration of cyst membrane and therefore its rupture. 3 The risk increases with the size and the number of cysts. 4 Three types of rupture have been described 5 : contained rupture is a detachment of the pericyst from the endocyst; communicating rupture of the cyst with the bronchus that causes expectoration of hydatic sand and membranes; and a direct rupture that consists on the rupture of all membranes and the release of its content.
Uncomplicated hydatid cysts are usually asymptomatic and diagnosed incidentally by imaging examination such as a chest X-ray or a CT scan. While complicated cysts are usually revealed by nonspecific symptoms such as cough chest pain hemoptysis fever or anaphylactic choc, which suggest cyst rupture. The clinical diagnosis can be made if there are expectorations of membranes and hydatid sand. 6
A ruptured hydatic cyst have different radiological appearances depending on the ruptured layer, the amount of air and the rupture type.
It starts when the hydatic cyst erode a bronchus and causes air between the endocyst and the pericyst which appears as a radiolucent rim around the cyst on X-ray as known as the “crescent sign,” easily seen on CT scan. Occasionally air may be present only on the posterior of the cyst with no anterior extension, called “the inverse crescent sign,” or a small air focus between the 2 layers can be seen, known as “air bubble sign” (contained rupture).
Due to the presence of air between the 2 layers, the endocyst gets more fragile and causes its rupture. Therefore, air will be present within the endocyst and a crescent of air between the endocyst and the pericyst resulting an “onion peel appearance” or “the cumbo sign.”
The complete rupture of the endocyst lead to the accumulation of more air, the spillage of the fluid contained and the shrinking and collapse of membranes, that have the appearance of a whirl hence the “whirl sign” or of membranes floating on fluid called “water lily sign.” The membranes can appear as a mass within the cyst when settled in one part of the cavity. A complete spillage of the membranes and fluid result the appearance of a cyst filled only with air called the “dry cyst sign.” 6
The pleural rupture of the cyst can cause a tension hydrothorax such this case, simple or tension pleural effusion or empyema. 7 Sometimes the membranes that have been spilled out of the cyst can be seen floating in the pleural cavity which make the diagnosis more accurate.
A ruptured cyst is at high risk of superadded infection 8 and have the same clinical and radiological features as a lung abscess. Therefore, the importance of knowing some imaging features that can lead to this diagnosis. The first common sign seen is the ring enhancement sign, which is a thickened wall with a contrast up-take. Also the presence of an air fluid level or air bubbles within the cyst can indicated superadded infection. 6
Conclusion
Hydatic disease is worldwide zoonosis responsible for simple and complicated cyst that can be located in all organs. The lung is the most frequent location for children. The clinical features are nonspecific. However, the diagnosis is suspected upon certain radiological appearances and biological findings. The rupture of the hydatic cyst is the most common complication, have a variety of imaging findings depend on the ruptured layer, the amount of air and the rupture type.
Footnotes
Author Contributions
All authors contributed equally to this work.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.