
Abstract
Bronchopulmonary dysplasia (BPD) is a complication of preterm and low birth weight infants. The incidence of BPD has not decreased over the past 20 years. Complications of BPD include rehospitalization, chronic lung disease, cardiovascular disease, and impaired growth and development which will affect the patient's quality of life. There are unfortunately limited data available regarding BPD in Indonesia. This study is expected to be a reference in taking preventive measures to reduce mortality and morbidity in preterm and low birth infants. This study aims to determine predictors of BPD in infants with birth weight less than 1500 g. We conducted a retrospective cohort study that included 116 infants with birth weight <1500 g. Twenty-two (19%) infants had BPD with the highest proportion (63.6%) in the 28 to 31 weeks of gestational age. Multivariate analysis showed mechanical ventilation in more than first 2 days of life (P = .008; HR = 7.7), hematocrit <39% (P = .001; HR = 12), and hemodynamically significant patent ductus arteriosus (hsPDA; P = .041; HR = 3.5) were significant predictors of BPD in infants with birth weight <1500 g.
Introduction
Bronchopulmonary dysplasia (BPD) is a clinical diagnosis based on persistent oxygen dependence for a period after birth. 1 The consensus held by the National Institute of Child Health and Human Development (NICHD) in 2001 divided BPD into 2 groups, that is, infants with gestational age <32 weeks and those with ≥32 weeks. The time to determine the diagnosis is at 36 weeks postmenstrual age (PMA) in infants with gestational age of <32 weeks. Meanwhile, it is at a chronological age of 28 to 56 days in infants with gestational age ≥32 weeks.
The global incidence of BPD in extremely preterm infants (<28 weeks of gestational age) is 10% to 89% (10%-73% in Europe, 18%-89% in North America, 18%-82% in Asia, and 30%-62% in Oceania). 2 Forty percent of extremely low birth weight infants (<1000 g) will develop BPD. 3 Studies about BPD in Indonesia are still rare. According to a study conducted in Bandung, Indonesia, 14.8% of preterm infants (28-34 gestation weeks) with respiratory distress syndrome (RDS) experienced BPD. 4 Unlike other complications of preterm birth, the incidence of BPD has not decreased over the past 20 years as reported by the NICHD Neonatal Research Network.
BPD remains a problem as the more very low birth weight neonates survive; the higher their survival rate, and the more likely the incidence of BPD to increase. 5 It is essential to identify predictors of BPD development, and preventative interventions should therefore be targeted at high-risk infants. Several studies indicated that the duration of mechanical ventilation,6-8 RDS,9,10 early onset sepsis,10,11 small for gestational age,12,13 patent ductus arteriosus,7,9,14 neutrophil lymphocyte ratio (NLR), 10 thrombocytopenia, 15 and anemia 8 were associated with the incidence of BPD. However, those studies showed inconsistent results. We would like to estimate the incidence of BPD among infants born with birth weight of less than 1500 g at our Neonatal Unit and to identify associated predictive factors.
Methods
Study Design and Population
We conducted a retrospective cohort study at the level II and III of Neonatal Unit of Dr. Sardjito Hospital Yogyakarta Indonesia, in the period between January 1st, 2017 and November 31st, 2021. All survived infants beyond 28 days after birth with birth weight <1500 g who were admitted to Neonatal Unit for the first 24 hours were recruited. The infants with major congenital malformations (congenital pulmonary airway malformation, congenital lobar emphysema, and critical congenital heart disease), post-surgery that affected the respiratory system such as diaphragmatic hernia, infants born to mothers with hemolysis, elevated liver enzymes, low platelets (HELLP), immune thrombocytopenic purpura (ITP), or systemic lupus erythematosus (SLE), and infants with incomplete medical records were excluded.
Data Collection
Data were obtained from a secondary database. The recorded predictors were mechanical ventilation, RDS, early onset sepsis, hsPDA, SGA, hematocrit level, platelet count, and NLR. Duration of mechanical ventilation was determined as either with intubation or nasal intermittent positive pressure ventilation (NIPPV) for more than first 48 hours of life. RDS was defined as respiratory distress with radiographic findings showing a uniform reticulogranular pattern, referred to as a ground-glass appearance, and was accompanied by peripheral air bronchograms. Hemodynamically significant patent ductus arteriosus (hsPDA) was defined as the ductus arteriosus which remains to open with a systemic-to-pulmonary shunt resulting in pulmonary hyperperfusion and systemic hypoperfusion. Diagnostic parameters for the hsPDA includes (1) precordial pulsation, (2) systolic murmur, (3) tachycardia (heart rate >160 beats per minute), (4) respiratory arrest or use of mechanical ventilation, (5) pulse bounding of femoral conditions, (6) hepatomegaly, (7) metabolic acidosis (pH <7.30) and base excess <−5, and (8) worsening respiratory function. HsPDA was confirmed if the score was ≥2 and/or confirmed by echocardiography performed by a pediatric cardiologist. Small for gestational age (SGA) was a birth weight below the 10th percentile; while percentile between the 10th and 90th was categorized into appropriate for gestational age (AGA) and >90th percentile was considered large for gestational age (LGA) based on the Yogyakarta Indonesian Newborn Curves. 16 Neutrophil lymphocyte ratio (NLR) was defined as the absolute neutrophil count divided by the absolute lymphocyte count measured for the first time within 24 hours postnatally. The NLR cut-off was 0.64. 17 Neonatal early onset of sepsis was defined as bacteremia occurring at ≤ 72 hours, which met 4 out of the following criteria, that is, temperature instability, central nervous system dysfunction, respiratory distress, cardiovascular disturbance, gastrointestinal symptom, renal insufficiency, and hematologic disorder. Platelet count was determined within the first 2 weeks of life, with cut-off less than 150 000/mm3. 15 Hematocrit was confirmed within the first 2 weeks of life, with cut-off less than 39%. 8
Statistical Analysis
Baseline characteristic predictors and outcome variables were compared between infants with birth weight <1500 g and those ≥1500 g. We performed a Kaplan-Meier curve to determine the mean time of BPD occurrence in each independent variable. Multicollinearity test was conducted on the independent variables that had similarities in regression model, namely early onset sepsis, platelet count, and NLR. Cox regression analysis was used to ascertain the magnitude risk of the variable on the incidence of BPD. To identify the most influential factor on the incidence of BPD; multivariate Cox regression was applied to the independent variables with P-value below .25. The data were shown as hazard ratios (HR) with 95% confidence intervals (CI). P-value of .05 was used to determine the statistical significance. Statistical analysis was carried out using a computerized data processing software.
Ethical Approval
The study was approved by the Medical and Health Research Ethics Committee of the Faculty of Medicine, Universitas Gadjah Mada/Dr. Sardjito Hospital Yogyakarta, Indonesia with number KE/FK/0108/EC/2022.
Results
We enrolled 116 neonates with the proportion of male and female 1:1.3. The highest proportion in the gestational age group was 28 to 31 weeks (Table 1). Out of all subjects, the incidence of BPD was 19%, for which the highest proportion was found in the <28 weeks of gestational age and <1000 g group.
Baseline Characteristics of the Subjects.

t n (%). :f:, mean (range) §, median (range).
Abbreviations: CPAP, continuous positive airway pressure; HsPDA, hemodynamically significant patent ductus arteriosus; PDA, patent ductus arteriosus.
The mean time to diagnose BPD in infants <1500 g was 65.6 days (Figure 1). In total, 22 out of the 116 infants whose birth weight was <1500 g developed BPD, with the incidence rate of 4.7 cases per 1000 person-days, or 1.7 cases per person-year. The mean BPD survival time of mechanical ventilation more than first 2 days, hsPDA, SGA, and hematocrit levels showed a statistical significant difference (Table 2).

Kaplan-Meier curve of BPD in infants with birth weight <1500 g.
BPD Survival Analysis on Predictors.
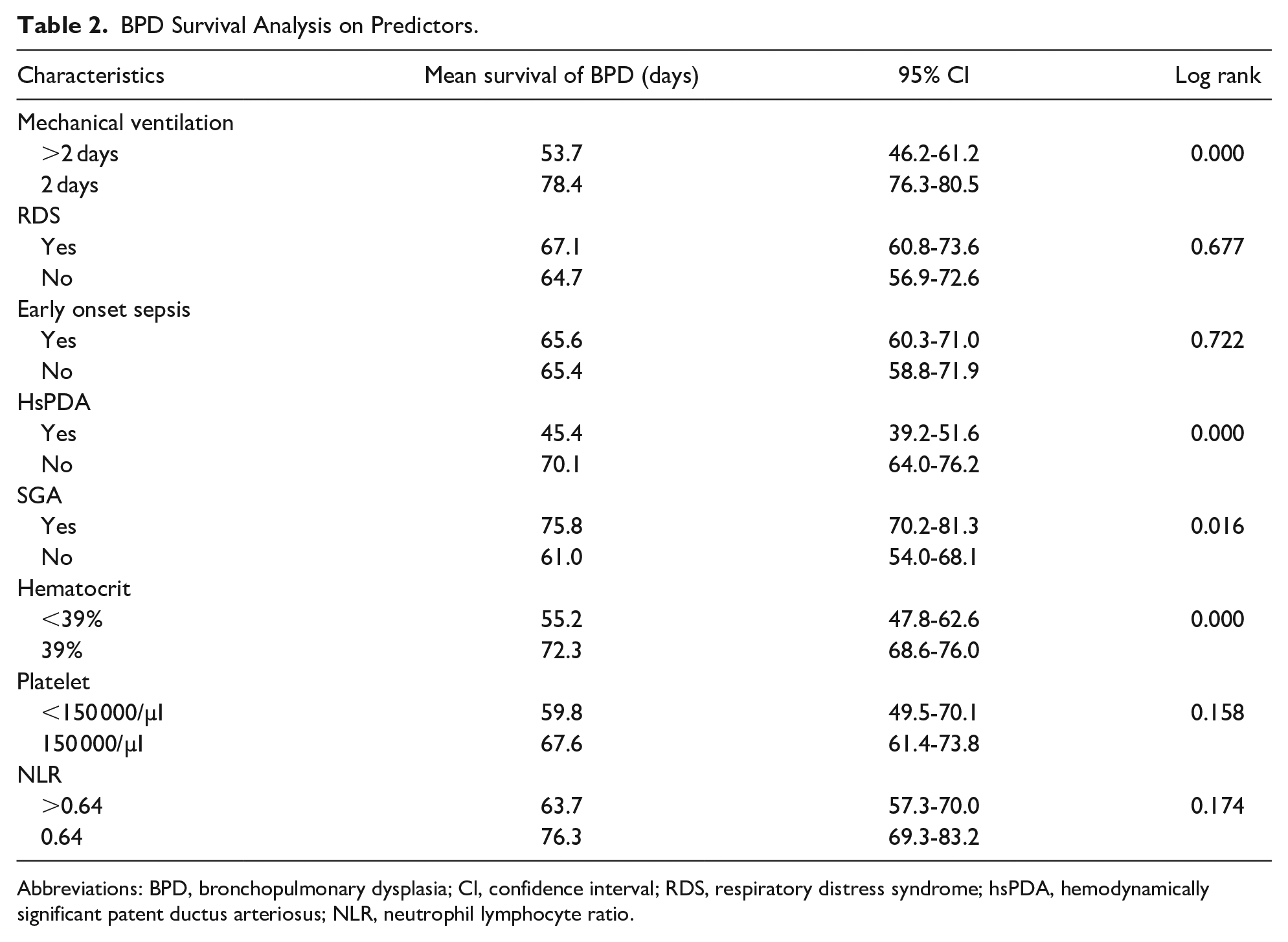
Abbreviations: BPD, bronchopulmonary dysplasia; Cl, confidence interval; RDS, respiratory distress syndrome; hsPDA, hemodynamically significant patent ductus arteriosus; NLR, neutrophil lymphocyte ratio.
Cox regression analysis was used to determine the magnitude of risk from each independent variable on the incidence of BPD. Bivariate analysis (Table 3) revealed that the use of mechanical ventilation for more than first 2 days of life significantly affected the incidence of BPD (P = .011, HR = 7.34; 95% CI 1.57-34.16), with the absolute risk difference of 47.3%. HsPDA significantly influenced the incidence of BPD (P = .026; HR = 4.11; 95% CI 1.18-14.26), with the absolute risk difference of 49.8%. Likewise, anemia with hematocrit level <39% also significantly prompted the incidence of BPD (P = .001, HR = 13.58; 95% CI 2.88-63.99), with the absolute risk difference of 44.9%. Multicollinearity test was performed on the independent variables of early onset sepsis, platelet count, and NLR. There was no multicollinearity among them.
Prediction of BPD.
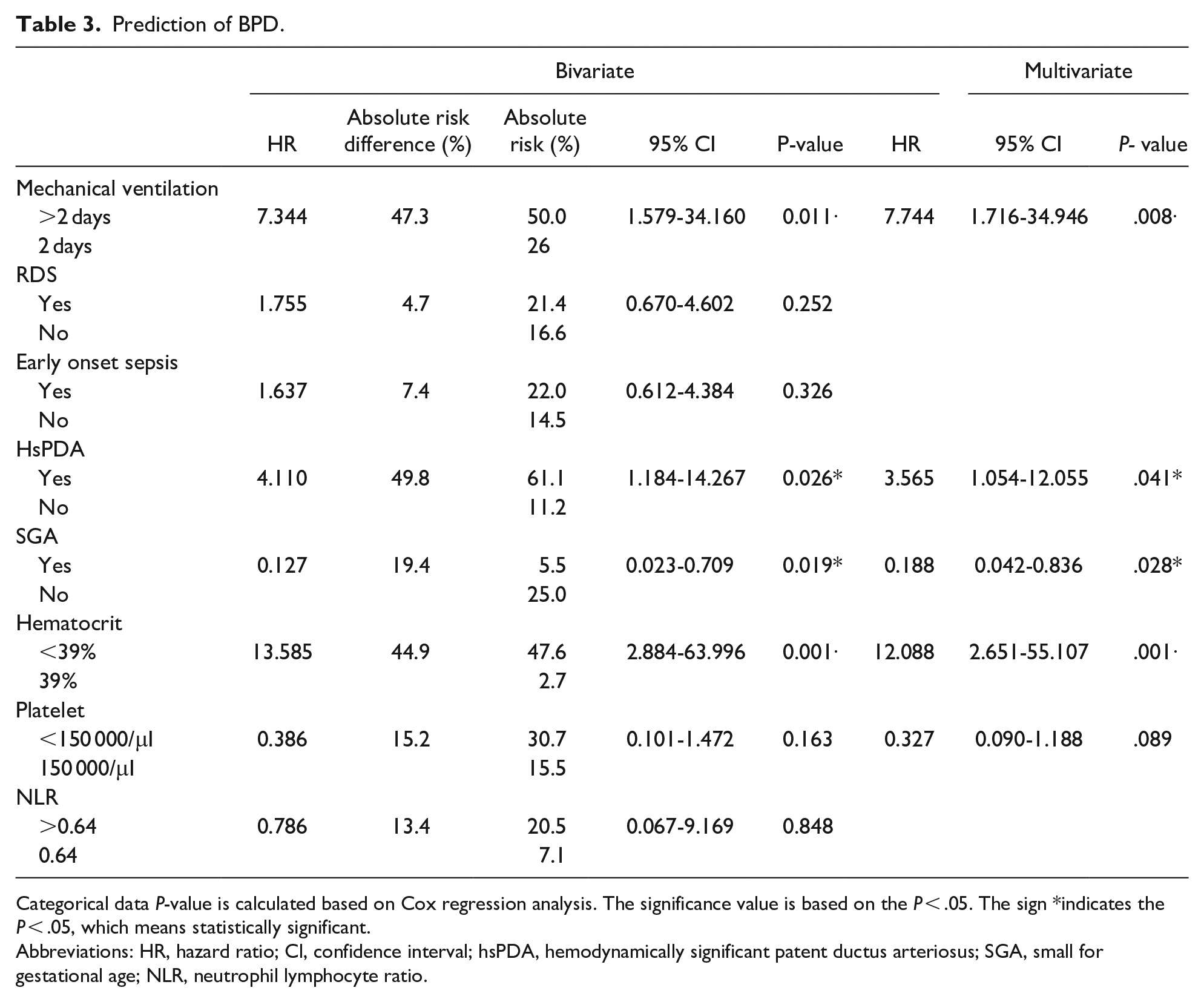
Categorical data P-value is calculated based on Cox regression analysis. The significance value is based on the P < .05. The sign *indicates the P < .05, which means statistically significant.
Abbreviations: HR, hazard ratio; Cl, confidence interval; hsPDA, hemodynamically significant patent ductus arteriosus; SGA, small for gestational age; NLR, neutrophil lymphocyte ratio.
Multivariate analysis included 5 variables out of 8 variables with P-value <.25 in bivariate analysis, that is, mechanical ventilation for more than first 2 days of life, hsPDA, SGA, hematocrit level, and platelet count. The significant predictor factors on the incidence of BPD were mechanical ventilation (P = .008; HR = 7.74, 95% CI 1.71-34.94), hsPDA (P = .008; HR = 3.56, 95% CI 1.05-12.05), and hematocrit level (P = .008; HR = 7.74, 95% CI 1.71-34.94; Table 3).
Discussion
The incidence of BPD in infants with birth weight <1500 g in our Neonatal Unit was 19%. It was lower than that of the South American Neocosur Neonatal Network study (25%) and Brener Dik et al 18 (29.7%). Another study reported the incidence of BPD in VLBW infants was 28.9%; 37.3% for moderate BPD and 62.7% for severe BPD. 19 We found BPD among infants aged ≤31 gestational weeks. The highest BPD proportion (61.5%) was found in <28 weeks of gestational age infants. A similar result was reported by Zhang et al 20 that BPD occurred in <28 weeks of gestational age infants. According to the birth weight, our study showed that BPD was found in 11 out of 21 (52.3%) <1000 g infants. Cunha et al 21 also described similar result. Our data showed that the incidence of BPD was proportional to the gestational age and birth weight. The younger the gestational age and the lower birth weight, the more likely BPD to increase.
The use of mechanical ventilation during first 2 days of life was the most significant predictor of BPD (P = .008). The proportion was 34.5% in infants with birth weight <1500 g. We observed a higher incidence of BPD in mechanical ventilation group (50% vs 2.6%). HsPDA condition also led to higher risk of BPD in our study. The absolute risk difference between hsPDA and non-hsPDA group was 49.8% (61.1% vs 11.2%). This result was consistent with the results of the studies by Nascimento et al 22 and Alonso et al. 23
The proportion of BPD in infants with RDS was 48.3%. The absolute risk of RDS infants was greater than that in the control group (21.4% vs 16.6%). However, there was no significant difference between the RDS group and non-RDS (P = .252). Additionally, Cokyaman 24 reported a different result in his study with a greater number of subjects, that RDS was an independent predictor for BPD. Besides, the antenatal steroid, surfactant therapy, and early CPAP as the prevention and treatment for RDS, may interfere with the BPD outcome.
The absolute risk of BPD was higher in the early onset of sepsis than in non-sepsis group (22% vs 14.5%). However, we observed no significant difference between the sepsis and non-sepsis group (P = .326). It was consistent with the findings of Cokyaman 24 and Hernández-Ronquillo et al. 25 In their studies, late onset of sepsis was the predictor of BPD. Studies by Lahra et al 26 and Eriksson et al 27 also showed that late onset of sepsis increased the risk of BPD when compared with early onset of sepsis. To the contrary, Klinger et al 11 reported that early onset of sepsis was the significant predictor for BPD. This discrepancy was due to the different operational definition. Early onset of sepsis in Klinger’s study referred to clinical criteria and a culture-confirmed bacterial infection of the blood.
Thrombocytopenia was identified to be high in BPD. The absolute risk of BPD in the thrombocytopenia group was greater than that in the control (30.7% vs 15.5%); however, it was not a significant predictor of BPD in this study (P = .163). A study by Wang et al 15 reported a different result. This was due to the different characteristics of subjects with a wider gestational age and birth weight, whereby the frequency of thrombocytopenia found in infants with birth weight <1000 and <750 g were 75% and 90%. Maternal factors (HELLP syndrome, ITP, SLE, and hypertension) may cause early onset thrombocytopenia. We had excluded those conditions in our study.
The absolute risk of BPD in the NLR >0.64 group was higher than in the control group (30.7% vs 15.5%). The multivariate analysis showed that it was not a significant predictor of BPD in infants with birth weight <1500 g (P = .848). This finding was different from the one in the study conducted by Ozdemir, 17 which reported that NLR >0.64 in the first 24 hours of age was an independent predictor factor for BPD. It was probably due to the different characteristics of subjects, in which they were in gestational age of <32 weeks and birth weight <2000 g. Also, maternal conditions (maternal hypertension, hemolytic anemia, and intrauterine viral infection such as Rubella and Cytomegalovirus) may affect the production of neutrophils. We observed maternal hypertension in 33.6% of subjects.
HsPDA was a significant predictor of BPD in infants with birthweight <1500 g (P = .008). The absolute risk of hsPDA group was higher than that in the control (61.1% vs 11.2%), which was consistent with the studies by Cokyaman, 24 Schena et al, 28 and Clyman and Hills. 29 There were 7 out of 18 subjects (38.8%) who received medical treatment for PDA closure in our study. There was 1 patient (5.5%) who underwent ductus arteriosus ligation therapy. A prospective cohort study by Liebowitz and Clyman 30 reported that indomethacin prophylaxis in hsPDA had a lower risk of BPD and was statistically significant when compared with the hsPDA conservative group. In contrast, a report by Benitz 31 showed that regular therapy (as prophylactic or in hsPDA) and early PDA closure (in the first 2 weeks of life) did not improve the long-term outcome of preterm infants.
Anemia with hematocrit level <39% was a significant predictor for the incidence of BPD. The anemia group had higher absolute risk of BPD than the control group (47.6% vs 2.7%). Studies by Duan et al 8 and Lee et al 32 had similar results, which showed that anemia was associated with increased risk of BPD. Different result was reported by Ming et al 33 that anemia was not a significant predictor for the incidence of BPD (P = .293), except for severe anemia (P = .013). It was due to different onset of anemia between the studies. We only observed the anemia that occurred in the first 2 weeks of life.
The risk of BPD between SGA and AGA group was statistically significant (P = .028). The absolute risk of BPD in AGA group was higher than that in SGA (25% vs 5.5%, respectively). This was different from the previous study by Charles et al 12 which revealed that the incidence of BPD was higher in SGA group (P = .025). The discrepancy was caused by the different characteristic of the subjects, which was limited to only ≤750 g and we did not observe the severity of BPD.
It was the first study regarding the predictors of the incidence of BPD in infants with birth weight <1500 g in Indonesia. The limitation of this study was the retrospective study design, for which the use of secondary data from medical records could lead to measurement bias compared with prospective study. This study did not differentiate the outcome of BPD based on severity. A research of the effect of early CPAP administration and management of PDA closure (medication or ligation) on the incidence of BPD needs to be conducted.
Conclusion
Mechanical ventilation use for more than the first 2 days of life, hematocrit <39%, and hsPDA were the significant predictors for the incidence of BPD in infants with birth weight <1500 g.
Footnotes
Author Contributions
GM Maytasari: Contributed to conception and design; Contributed to analysis and interpretation; Drafted the manuscript; Gave final approval; Agrees to be accountable for all aspects of work ensuring integrity and accuracy. EL Haksari: Contributed to conception and design; Contributed to analysis and interpretation; critically revised the manuscript; Gave final approval; Agrees to be accountable for all aspects of work ensuring integrity and accuracy. EP Prawirohartono: Contributed to conception and design; Contributed to analysis and interpretation; critically revised the manuscript; Gave final approval; Agrees to be accountable for all aspects of work ensuring integrity and accuracy.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.