
Abstract
This study evaluated nutrition and growth in relation to plasma adipokine levels in 21 very-low-birth-weight (VLBW) children with radiographic bronchopulmonary dysplasia (BPD), 19 VLBW controls, and 19 term controls with a median age of 11.3 years. We took anthropometric measurements; assessed plasma levels of adipsin, resistin, adiponectin, and leptin; and analyzed the children’s 3-day food records. Children with BPD had a smaller age-adjusted head circumference and more microcephaly but no other significant growth differences. Daily recommended nutritional intake levels were poorly met but did not differ between the groups. Leptin levels correlated positively with the body mass index standard deviation score in VLBW children. No other associations between adipokine concentrations and growth were found. There were negative correlations between leptin concentrations and fat intake, resistin levels and carbohydrate intake, and adiponectin, adipsin, and leptin levels and energy intake.
Introduction
Because more immature neonates are surviving, the incidence of bronchopulmonary dysplasia (BPD) has not decreased. 1 BPD impairs early growth, 2 and prematurity is associated with altered eating habits in later life. 3 Inflammation, a key pathogenic factor of BPD, affects metabolism, nutritional requirements, and growth in the neonatal period, 4 but its association with later growth is less clear. Adipokines are inflammatory markers with known associations to lung and metabolic diseases. 5 Preterm infants have lower adiponectin levels compared with term children at term-equivalent age. 6 Growth 7 and nutrition 8 may affect adipokine levels. Whether the growth and nutrition of the school-aged survivors of very low birth weight (VLBW; birth weight <1500 g) and BPD affect their adipokine status is not known.
Our aim was to study nutritional intake and growth, with respect to plasma levels of adipokines and neonatal factors, in VLBW school children with and without severe radiographic BPD and term controls. Our hypotheses were that (1) BPD children and VLBW controls would present with similar growth parameters, but term children would demonstrate better growth than VLBW cases; (2) nutritional differences would exist between BPD children and controls; and (3) plasma adipokine concentrations would be associated with growth parameters in VLBW children at school age.
Patients and Methods
Patient selection has been described in detail previously. 9 Tampere University Hospital records were searched to find VLBW children born between January 1, 1995, and April 13, 2003, with severe, Northway grade III to IV 10 cystic radiographic BPD and age-matched controls without radiographic BPD. We examined 59 children 6 to 14 years of age, comprising 21 VLBW children with radiographic BPD, 19 VLBW children without radiographic BPD, and 19 children born at term. The median age of the study cohort was 11.3 years (range = 6.3-14.2), and 64% were boys. The age and sex profile of the 3 groups was similar, with the exception of a lower-than-average percentage of boys in the VLBW control group (58%). Data from hospital records were collected, and a parental questionnaire was completed. Parents were considered to be overweight if their body mass index (BMI) was more than 25 kg/m2.
The children were examined by a pediatrician (TK) who measured their height, weight, and head circumference, and their BMI standard deviation score (BMI-SDS) was determined according to Finnish age-specific and sex-specific references.11-13 Microcephaly was defined as a head circumference of less than −2SD and macrocephaly as a head circumference of more than +2SD. Overweight and underweight were defined as BMI-SDS of more than 1.16 and less than −1.65 in girls and more than 0.78 and less than −1.83 in boys. 11 Long-term illnesses, such as asthma, cerebral palsy, epilepsy, and short bowel syndrome, were recorded.
Thigh, hip, waist, and middle upper-arm circumferences were measured with a tape measure, and the mean of 2 measurements was recorded. Biceps, triceps, subscapular, and suprailiacal skinfold thicknesses were measured with a Harpenden skinfold caliper according to the guidelines of the manufacturer (Baty
The adiponectin, adipsin, resistin, and leptin levels in plasma were determined as previously described 9 ; adipokine concentrations did not differ between the groups, as reported earlier. 9 The parents completed a food record of everything the participants ate and drank over 3 consecutive days, and a trained nutritionist interviewed the families and calculated nutrient intakes with the Diet32 dietary analysis program (Aivo AB Sverige, Solna, Sweden). The nutritional intakes were compared with national age-specific recommendations and the upper level of tolerable intake for adults. 15 An energy intake that was up to 200 kcal above or below the age- and sex-adjusted estimated energy requirement was considered normal to cover different levels of physical activity.
The study complied with the 1964 declaration of Helsinki and its later amendments. The ethics committee of the hospital district approved the study protocol, and written, informed consent was obtained from the parents.
Statistics
SPSS Statistics for Windows, version 18.0 (SPSS Inc, Chicago, IL), was used for the statistical analyses. Independent-sample t-tests or 1-way analysis of variance were used for normally distributed variables, the Mann-Whitney U test or Kruskal-Wallis test for non-Gaussian variables, and the χ 2 test or Fisher’s exact test for categorical variables. Values of P < .05 were considered statistically significant.
In VLBW children, the correlations between adipokine concentrations, anthropometric parameters, and nutrient intake were studied using Pearson’s r correlation test for normally distributed variables and Spearman’s rank correlation coefficient (ρ) test for nonnormally distributed variables.
Logistic regression analysis was carried out among VLBW children to examine predictors for the lowest and highest quartiles of BMI-SDS and the lowest quartile of length for age and microcephaly. First, univariate analysis was carried out. Variables were then simultaneously entered into multivariate analyses in 2 categories. The first variables were birth weight, neonatal sepsis, radiographic BPD, severe intraventricular hemorrhage (IVH) of grade III or more, 16 or periventricular leukomalacia and Bell stage 2 or 317 necrotizing enterocolitis (NEC). The second variables were the intake of energy, fat, protein, and carbohydrates. The results were expressed as odds ratios (ORs) and 95% CIs.
Results
One child with radiographic BPD with a birth weight of less than −2SD was considered small for gestational age. Children with radiographic BPD had poorer initial weight gain and higher rates of IVH, sepsis, and NEC than the VLBW controls (Table 1). Three children with radiographic BPD with NEC had undergone bowel resection, and 1 had short bowel syndrome.
Characteristics of the VLBW Infants During Their First Hospitalization Period.
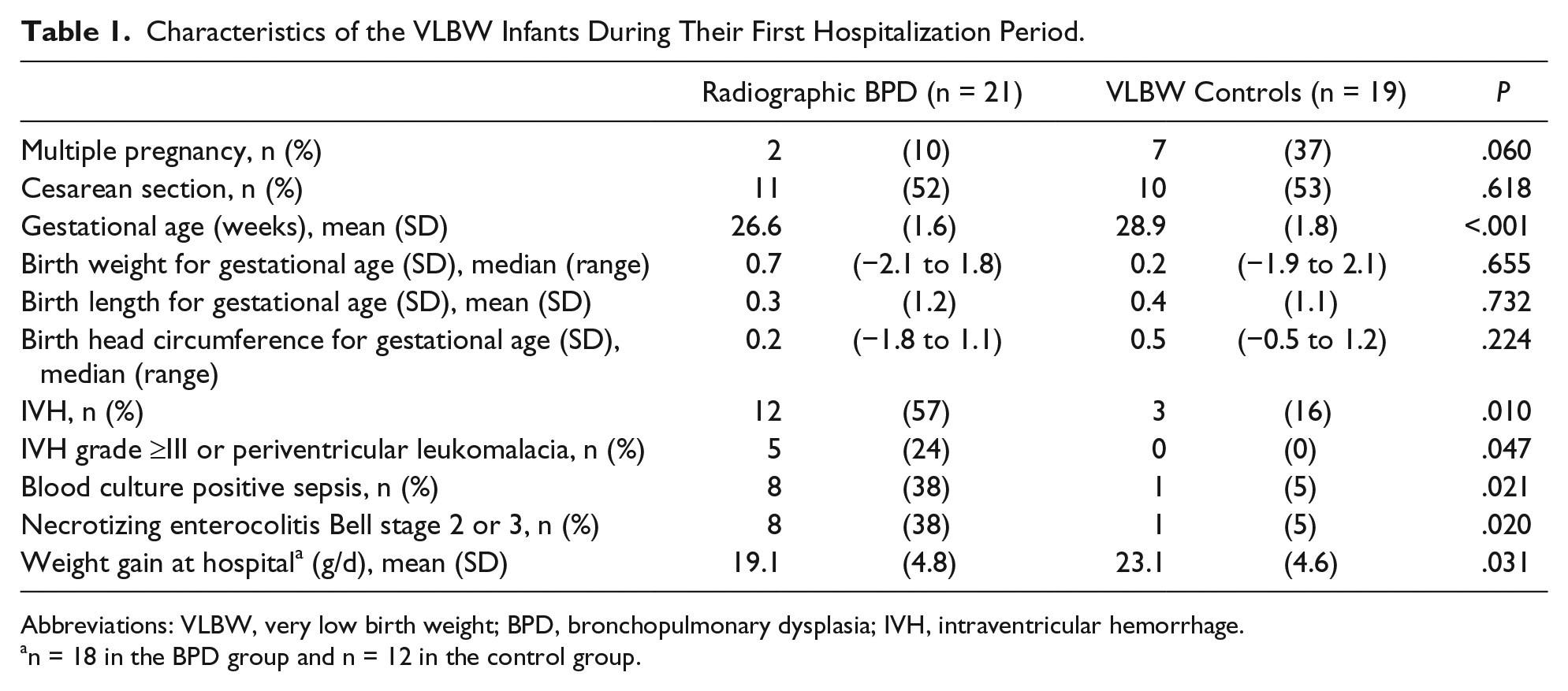
Abbreviations: VLBW, very low birth weight; BPD, bronchopulmonary dysplasia; IVH, intraventricular hemorrhage.
n = 18 in the BPD group and n = 12 in the control group.
At school age, the only anthropometric difference between the groups was in head circumference (Table 2). Children with radiographic BPD had a smaller age-adjusted head circumference and were more likely to have microcephaly than the controls (Table 2). In all, 8 VLBW children with microcephaly at school age had smaller age-adjusted head circumferences at birth, with a mean and SD of −0.5 (0.86) versus 0.39 (0.62), and their weight gain during initial hospitalization was poorer, with a median (range) of 14.8 g/d (14.3 to −20.4) versus 22.8 g/d (7.0 to −28.5), compared with VLBW children without microcephaly. The BMI-SDS and the height for age were similar in VLBW children with and without microcephaly.
Growth Statistics of the School-Aged Children.

Abbreviations: BPD, bronchopulmonary dysplasia; VLBW, very low birth weight; BMI-SDS, body mass index standard deviation score; HC, head circumference; MUAC, middle-upper-arm circumference; SFT, skinfold thickness.
n = 17.
NEC survivors had a smaller head circumference at school age than children without NEC, with a mean (SD) of −1.6 (2.8) versus −0.4 (1.3), but the other anthropometric parameters did not differ. One of the 5 children with severe IVH or periventricular leukomalacia and 2 of the 4 children with cerebral palsy had microcephaly at school age. In addition, 9 of the radiographic BPD and 4 of the VLBW control children with long-term illnesses had smaller waist-to-hip ratios compared with children without those conditions. Apart from that, the other anthropometric parameters did not differ. Parental height and BMI did not differ between the groups.
Plasma adipokine concentrations were similar in prepubertal and pubertal children, with girls having higher adipsin levels than boys, with a median (range) of 916 ng/mL (598-1264) versus 787 ng/mL (483-1409). The girls’ leptin levels were also higher, at 7.1 ng/mL (2.1-37.6) versus 1.8 ng/mL (0.5-50.0), than those of the boys, but the adiponectin and resistin levels were similar between the sexes.
Food records were not returned by the parents of 1 child with radiological BPD, 3 VLBW controls, and 1 term child. There were no differences between the groups in regard to nutritional intake (Table 3), but daily nutritional intake recommendations were poorly met (Table 4), with the exception of vitamin B12 and phosphate, which were adequate in all children.
Average Daily Intake of Nutrients.

Abbreviations: BPD, bronchopulmonary dysplasia; VLBW, very low birth weight; SFA, saturated fatty acids; E%, percentage of total energy intake; MUFA, monounsaturated fatty acids; PUFA, polyunsaturated fatty acids; α-TE, α-tocopherol equivalent, equals 1 mg α-tocopherol; Vitamin A retinol equivalent, 1 µg retinol, equals 12 µg β-carotene; niacin equivalent, 1 mg niacin, equals 60 mg tryptophan.
RDI of Energy and Nutrients Compared With National Recommendations. a
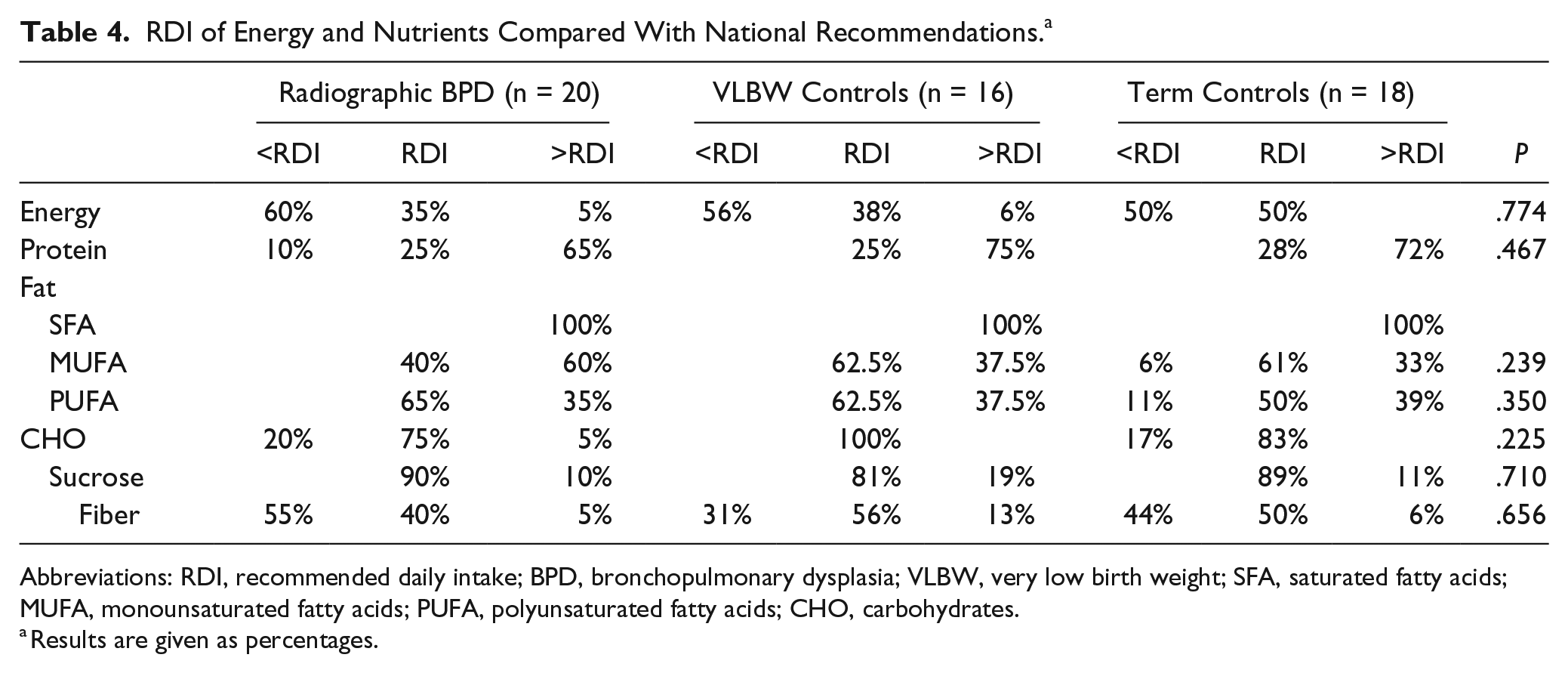
Abbreviations: RDI, recommended daily intake; BPD, bronchopulmonary dysplasia; VLBW, very low birth weight; SFA, saturated fatty acids; MUFA, monounsaturated fatty acids; PUFA, polyunsaturated fatty acids; CHO, carbohydrates.
Results are given as percentages.
Plasma leptin concentrations correlated positively with BMI-SDS (ρ = 0.57) and negatively with fat intake (ρ = −0.36). Adiponectin (ρ = −0.36), adipsin (r = −0.33), and leptin (ρ = −0.55) levels correlated negatively with energy intake, as did resistin levels with carbohydrate intake (ρ = −0.36). Birth length for gestational age correlated negatively with resistin levels (ρ = −0.32) and birth head circumference for gestational age with adiponectin levels at school age (ρ = −0.47).
In the univariate logistic regression analysis, radiographic BPD was associated with an increased risk of microcephaly, with an OR of 9.69 (95% CI = 1.06-88.65), and so was neonatal sepsis (OR = 11.25; 95% CI = 1.91-66.39). In addition, neonatal sepsis seemed to predict short stature at school age in the multivariate analysis (OR = 11.57; 95% CI = 1.01-132.40). When gestational age was entered into the multivariate model instead of birth weight, the association between neonatal sepsis and short stature was no longer significant. Neonatal dexamethasone treatment was associated with microcephaly at school age in the univariate analysis (OR = 8.63; 95% CI = 1.44-51.72) but not when entered into the multivariate analysis. Short stature was found to be negatively associated with the intake of protein (OR = 0.35; 95% CI = 0.14-0.85), fat (OR = 0.12; 95% CI = 0.02-0.79), and carbohydrates (OR = 0.37; 95% CI = 0.15-0.37) and positively associated with energy intake (OR = 1.38; 95% CI = 1.03-1.58).
Discussion
School-aged VLBW survivors with radiographic BPD had smaller head circumferences and were more likely to have microcephaly than VLBW and term controls, but no other differences were found in growth parameters or nutritional intake. BMI-SDS correlated with leptin levels, but no other associations between plasma adipokine concentrations and anthropometric parameters at school age were found. There were negative correlations between leptin concentrations and fat intake, resistin levels and carbohydrate intake, and adiponectin, adipsin, and leptin concentrations and energy intake.
School-aged VLBW children have been reported to have smaller head circumferences and higher levels of microcephaly than term controls. 18 BPD has been associated with small head circumference at school age, 19 but not in all studies. 18 Because BPD mainly affects the most immature infants, neonatal comorbidity is high, and the independent effect of BPD on growth is difficult to establish. None of the neonatal factors remained significant in our multivariate logistic regression analysis. Previous study suggests that poor postnatal growth does not alter the later head growth. 20 The sickest infants appear to have the slowest growth velocity. 20 In contrast, our children with microcephaly had poorer neonatal weight gain compared with the other VLBW children. Children with microcephaly at school age were the sickest infants and had NEC, sepsis, and pulmonary problems requiring steroid treatment. The initial illness probably affected their brain growth more than poor neonatal weight gain. The head circumference measurements between the birth and the study date were not available in our study, which is a weakness. Although children with microcephaly at school age had smaller age-adjusted birth head circumference than VLBW children without microcephaly, none had microcephaly at birth. A previous study estimates that the critical period of brain growth extends to late infancy, and after the first year of life, the small head circumference tends to persist. 21 Parental head circumference was not measured, which is a major limitation, because the hereditability of head circumference has been reported to be up to 88% in childhood. 22
Nutritional intakes at school age were similar in the VLBW and term children. Although most of the children reported a lower-than-recommended daily energy intake, only 4 were underweight. However, the amount of physical exercise was not recorded, and this may explain the adequate weight gain. Underestimating energy intake in self-reports is common. 23 All children reported an excessive intake of saturated fatty acids, whereas low intakes of fiber and micronutrients were common. Similar unfavorable dietary habits have been reported in young VLBW adults, 3 and because this increases the risk of later chronic diseases, counseling about healthier eating from childhood could be an important tool for preventing disease.
Recommended micronutrient intakes are set to the average requirement of +2SD, and therefore, a lower-than-recommended intake does not mean that there was an inadequate food supply. 15 We did not measure blood vitamin or mineral levels. Our food diaries can be regarded as reliable because they were checked with the nutritionist, but the food diaries only provide an estimate of short-term intake, with variability depending on the season and different food-related occasions.
The only correlation between plasma adipokine levels and growth parameters in school-aged VLBW survivors was between BMI-SDS and leptin levels. Greater weight has previously been associated with higher leptin and lower adiponectin levels in children. 24 It seems that the association between inflammatory marker levels and growth is not more marked in VLBW survivors than in other school children.
Lower leptin levels were correlated with a greater intake of energy and fats. In a previous study of obese adults, weight correlated positively with leptin and negatively with leptin receptor concentrations, and both leptin and leptin receptor levels correlated negatively with total energy intake. 20 That study highlighted the role of the leptin/leptin receptor levels in satiety control and total energy intake and the importance of the synergistic interrelationships between the adipokines. 20 Adiponectin and adipsin levels correlated negatively with energy intake in our VLBW children. Adiponectin has been linked to insulin sensitization, and adipsin to triglyceride storage, 21 and a decrease in energy intake has been associated with an increase in adiponectin levels in adults. 25 Levels of resistin, which have a controversial effect on glucose metabolism, 21 have been shown to correlate negatively with carbohydrate intake. In addition, a high-fiber diet has been shown to decrease resistin levels in children. 8 It seems that adipokine concentrations, and thus the risk of metabolic diseases, can be modified by a diet.
NEC survivors had a smaller head circumference than children who had not had NEC, and neonatal sepsis was associated with microcephaly and shorter stature at school age. Neonatal sepsis and NEC have been shown to increase the risk of growth impairment in toddlers, and the resulting systemic inflammatory response has been shown to activate a local inflammatory response in the brain, leading to impaired neurodevelopment and head growth. 26 Our results suggest that the impact of neonatal inflammation on growth, together with neurocognitive development as a result of microcephaly, may persist up to school age.
Head circumference at birth correlated negatively with adiponectin levels in VLBW children, as did birth length with resistin levels. Previous studies have found an association between low birth weight and low adiponectin levels at school age 27 and high leptin levels in adults. 28 Weight gain during infancy has been positively associated with leptin concentrations at school age 7 and negatively associated with adiponectin levels at 17 years of age. 29 It has been suggested that adipokine secretion is programmed in utero. 27
Previous data on the growth of modern age BPD survivors at school age have been relatively limited. Our study is a single-center study that minimized the effect of different neonatal treatment protocols on the results but was also limited by the number of patients that were available. The number of cases was not based on power analysis; instead, all available patients with severe radiographic BPD treated in our hospital during an 8-year period were studied. Based on small groups and wide 95% CIs, underpowering may be one reason for negative results. In the case of positive results, such as the statistically significant trend of more instances of microcephaly in BPD children, the power is sufficient, although the number of cases is small. Potential confounders, such as different gestational age, were considered in multivariate analyses.
Conclusions
Children with radiographic BPD presented with poorer head growth and a greater incidence of microcephaly at school age than VLBW and term controls. BMI-SDS correlated with leptin levels, but otherwise, adipokine levels at school age seemed to have no association with growth parameters in VLBW children. Plasma adipokine levels correlated with nutritional intake, and as a result, dietary counseling would be beneficial.
Author Contributions
PS: Contributed to acquisition, analysis, and interpretation; drafted the manuscript; agrees to be accountable for all aspects of work ensuring integrity and accuracy.
TK: Contributed to conception, design and acquisition; gave final approval.
PK: Contributed to conception, design, analysis, and interpretation; drafted the manuscript; gave final approval.
RN: Contributed to conception, design and acquisition; gave final approval.
EM: Contributed to conception, design and acquisition; gave final approval.
TL: Contributed to conception, design and analysis; gave final approval.
OT: Contributed to conception, design, analysis, and interpretation; drafted the manuscript; gave final approval.
Footnotes
Acknowledgements
The authors thank nutritionists Terttu Peltola, Heli Alden and Terhi Heino and laboratory technicians Petra Miikkulainen and Elina Jaakkola for their help with this study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study received financial support from the EVO funds of Tampere University Hospital and Päijät-Häme Central Hospital, and the Tuberculosis Foundation of Tampere.