
Abstract
The aim of this study was to characterize the acute complications that required hospitalization in children under 5 years with Sickle Cell Disease. The population included 70 patients, 64% of African ascendency and 95.7% homozygotic for the HbS. We analyzed data from 337 hospitalizations. The first hospitalization occurred before 12 months in 38.6% and the average hospital admission per child was 3.92. The mean duration per hospitalization was 5.36 days. The most common diagnosis was vaso-occlusive crisis (36.8%) followed by fever, upper airway infections, bacterial pneumonia and splenic sequestration. Hemoglobin values at admission were between 6 and 7 g/dL in 22.3%, with 44.2% requiring at least 1 blood transfusion. There are several acute complications of SCD, being vaso-occlusive crisis the most common. Splenic sequestration generally occurs during the first 2 years and is associated with the need of transfusion. They represent a significant burden, with each child spending approximately 3 weeks hospitalized.
Introduction
Sickle cell disease (SCD) is a group of genetic blood disorders caused by sickle hemoglobin (HbS), with 2 key features: chronic hemolytic anemia and vaso-occlusion.1,2 Chronic but stable anemia is common, with basal hemoglobin value of 6 to 10 g/dL. The major causes for an acute drop are aplastic crisis and splenic sequestration, both potentially life-threatening situations. 3
Acute painful events, one of the most common complications, are the main reason for these patients to go to the hospital.4,5 The first episode often occurs in the small bones of hands and feet. Vaso-occlusive crises (VOCs) are triggered by infection, dehydration, emotional stress and exposure to cold, wind, or high altitude. 6
Another complication is splenic infarction which renders patients functionally asplenic by 2 to 4 years of age, which increases the risk of serious infection by encapsulated organisms.7,8
Stroke is a major and severe complication of SCD, primarily occurring during childhood.
In this study, the authors describe a population of children up to 5 years who were hospitalized due to acute complications of SCD, with the goal of characterizing those hospitalizations and, if possible, their correlation with age of diagnosis, type of SCD and compliance to medication and vaccination.
Methods
This is a descriptive retrospective study (January 1, 2010-December 31, 2019) at a level II Hospital in the region of Amadora and western Sintra in Lisbon, corresponding to a total population of 568 069 with 90 761 children under 15 years old. 9 It serves a foreign resident population (8.65% in Sintra, 10% in Amadora), corresponding to 55.6% and 62% African residents, so this area is particularly interesting for the study of SCD. Computerized records of children (<5 years of age) with a diagnosis of SCD and hematologic follow-up were reviewed.
The exclusion criteria were children with less than 2 years of pediatric hematology follow-up or admission in another hospital.
The analyzed data included: demographic data (age, gender, date of birth, and family’s birthplace), type of SCD, age, and context of diagnosis; age of first complication, number of hospitalizations per children and their respective diagnosis and approach, regular follow-up and the compliance to medication, and vaccination.
Statistical analysis was performed in SPSS statistical software version 23.0. A P-value < .05 was considered statistically significant.
Ethics permission for the study was obtained from the Ethics Committee of the hospital.
Results
Between 2010 and 2019 our hospital followed 86 children under the age of 5 years with SCD. Of these 86 children, 16 (18.6%) did not have any hospitalization until 5 years of age. A study population of 70 children, 50% female and 64% of African ascendency was analyzed.
Regarding the type of SCD, the majority were homozygous for the HbS (n = 67, 95.7%). Only one case of the following were identified: Hemoglobin SC (1.4%), Hb Sβ+-Thalassemia (1.4%), Hb Sβ0-Thalassemia (1.4%). We analyzed baseline hemoglobin (Hb) levels by framing them at 1 g/dL intervals, with 41.4% (n = 29) having a basal hemoglobin value between 7 and 8 g/dL.
Concerning the context in which the diagnosis was established, 47.1% (n = 33) were diagnosed through neonatal screening (hemoglobin electrophoresis at birth), 34.3% (n = 24) during hospitalization and 15.7% (n = 11) in a medical appointment. In 2 children (2.9%) we could not access data regarding this parameter (diagnosed in African countries). The median diagnosis age was 6 months (interquartile range 1-12 months) with 95.7% being diagnosed until 2 years.
Considering just children born after 2013, the year that selective neonatal screening started at our hospital, 71% (22 of 31) were diagnosed trough this method. Thus, the median age at diagnosis of children born after 2013 is 2 months (interquartile range 1-10 months).
The vaccination status was analyzed and 97.1% were compliant with the Portuguese National Vaccination Program. The complete immunization adherence rate, including recommended vaccines not included in the National Vaccination Program (Pneumococcal polysaccharide, Influenza, Meningococcal B, and Meningococcal ACWY) was 54.3% (n = 38).
Regarding treatment, all children took folic acid supplementation, 99% were under daily prophylactic amoxicillin and 8.6% (n = 6) underwent hydroxycarbamide therapy.
During the study period, we analyzed data from a total of 337 hospitalizations.
Considering the 70 children that were hospitalized, each child had on average 4.81 hospitalizations (standard deviation 4.17; minimum 1; maximum 25) and the mean duration per hospitalization was approximately 5.36 days (standard deviation 5.7; minimum 1; maximum 73 days).
The age of the first hospitalization for each child occurred before 12 months of age in 27 children (38.6%), in 20 children (28.6%) between 1 and 2 years, in 11 children (15.7%) between 2 and 3 years, in 7 (10%) between 3 and 4 years and in 5 children (7.1%) after 4 years (Table 1).
Frequency of First Hospitalization Per Age Group.

We analyzed the total number of hospitalizations, number of children hospitalized, and the total duration of hospitalization according to the age group (Table 2). The age group with a higher number of hospitalizations and children hospitalized was between 2 and 3 years (n = 87 hospitalizations; n = 40 children), followed by the age group of 1 to 2 years (n = 82 hospitalizations; n = 36 children), with the lowest number of hospitalizations and children hospitalized being observed before 12 months (n = 41 hospitalizations; n = 26 children).
Number of Hospitalizations, Number of Children Hospitalized, Total Days of Hospitalization and Their Respective Mean Per Age Group.

Four children had more than 10 hospitalizations during the study period and had their last hospitalization at the age of 4 years (Table 3).
Children with More Than 10 Hospitalizations and Their Respective Diagnostics.

The most common diagnosis was vaso-occlusive crises (VOC) verified in 36.8% of hospitalizations (n = 124) (Table 4). Concerning the localization of each VOC, the majority were abdominal (n = 45, 36.3%), followed by lower limbs (n = 32, 25.8%), upper limbs (n = 15, 12.1%), lumbar (n = 10, 8.1%), dactylitis (n = 8, 6.5%) and thoracic (n = 3, 2.4%). In 10 VOCs there was reference to more than 1 location (abdominal and lower limbs in 3.2%; abdominal and lumbar in 2.4%; upper and lower limbs in 1.6%; and lumbar and lower limbs in 0.8%).
Absolute Number and Relative Frequency of Each Diagnosis in Hospitalizations.

Considering hospitalizations with the diagnosis of VOCs by age group, these were more frequent between 2 and 3 years (n = 38), with lower limbs being the most frequent localization followed by abdominal; the second age group was between 4 and 5 years (n = 36), of which the majority were abdominal and lumbar. The age group with less than 12 months was the one with less hospitalizations due to VOCs (n = 5), being dactylitis the most frequent (Table 5).
Absolute Number of Hospitalizations Due to VOCs and its Location by Age Group.

From the 70 children hospitalized, 64% (n = 45) had at least 1 VOC and of these 37.8% (n = 17) had 1 episode; 1 child had 6; 6.7% (n = 3) had 7; and 1 child had 11 VOCs (Table 6). Approximately a third of the VOCs (n = 40, 32.3%) were associated with fever or an infectious condition.
Number of Children According to the Number of VOCs.

The second most frequent diagnosis was fever (n = 71, 21.1%), followed by upper airway infections (n = 53, 15.7%), bacterial pneumonia and splenic sequestration each with 10.7% (n = 36) and worsening of anemia (n = 32, 9.5%) (Table 4).
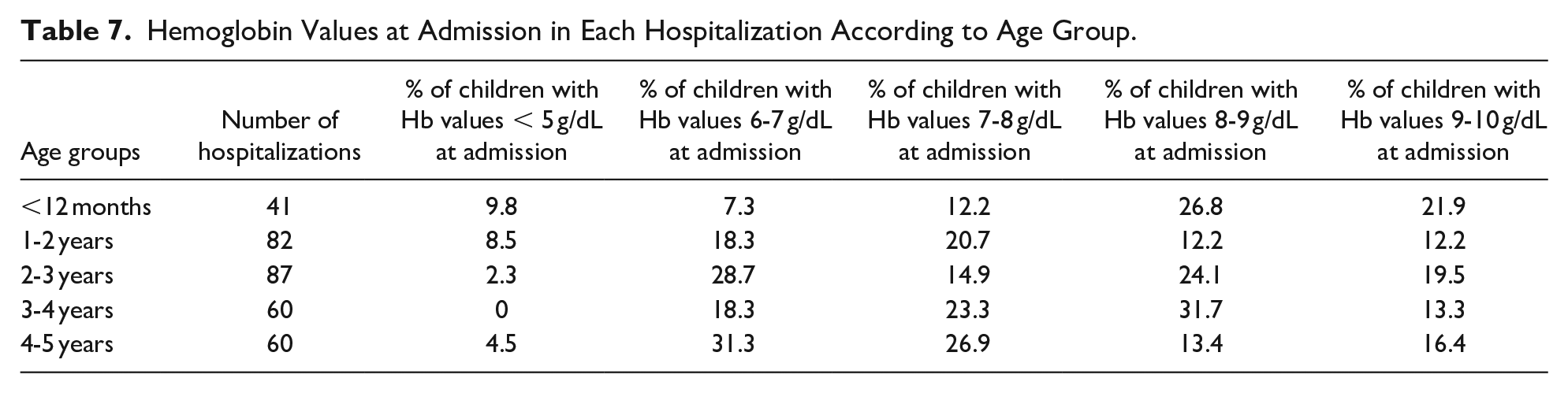
The Hb values at admission were between 6 and 7 g/dL in 22.3% (n = 75), 8 to 9 g/dL in 20.9% (n = 70), 7 to 8 g/dL in 19.9% (n = 67), 9 to 10 g/dL in 16.3% (n = 55) and below 5 g/dL in 4.8% (n = 16). We also analyzed the Hb values at admission according to the age group (Table 7). In the 41 hospitalizations during the first 12 months%, 26.8% (n = 11) had an Hb between 8 and 9 g/dL and 9.8% (n = 4) had an Hb value lower than 5 g/dL, which was associated with splenic sequestration. Of the 82 hospitalizations between 1 and 2 years, the most common Hb value at admission was between 7 and 8 g/dL in 20.7% (n = 17) and in 8.5% (n = 7) was lower than 5 g/dL. These 7 hospitalizations matched 5 children, 4 of them with splenic sequestration and 1 child with complicated bacterial pneumonia. From the 87 hospitalizations between 2 and 3 years, 28.7% (n = 25) had Hb values between 6 and 7 g/dL and 2 children (2 hospitalizations) had Hb values below 5 g/dL due to splenic sequestration. Between 3 and 4 years there were 60 hospitalizations, 31.7% (n = 19) having an Hb value between 8 and 9 g/dL, with no child presenting Hb values below 5 g/dL. From the 60 hospitalizations between 4 and 5 years, the Hb values at admission were between 6 and 7 g/dL in 31.3% (n = 21) and inferior to 5 g/dL in 4.5% (n = 3). These 3 hospitalizations were associated with aplastic anemia, VOC and splenic sequestration.
Hemoglobin Values at Admission in Each Hospitalization According to Age Group.
Two children were submitted to splenectomy. The surgery was postponed until 2 years of age and both had multiple hospitalizations due to splenic sequestration.
Regarding the therapeutic approach during hospitalization, 60.2% of children (n = 203) required symptomatic treatment, which involved fluids and analgesics, and 38.3% (n = 129) underwent antibiotic treatment.
Blood transfusions occurred in 39.5% of hospitalizations (n = 137). Of the 70 children hospitalized, 37 (52.9%) needed at least 1 blood transfusion and 9 (24.3%) underwent 5 ou more transfusions. We analyzed the diagnoses associated with transfusions and 27% (n = 36) were associated with splenic sequestration, 24.1% (n = 32) with worsening anemia and 19.5% (n = 26) with VOC. Before 12 months, 13 of the 27 children required blood transfusions, corresponding to 14 of the 41 hospitalizations and the most common diagnosis was splenic sequestration. Between 1 and 2 years, 18 of 35 children needed at least 1 blood transfusion. We highlight a child that had 16 admissions, with 15 requiring blood transfusion, the majority (n = 9) due to splenic sequestration. Between 2 and 3 years, 18 children (42.9%) required blood transfusions, representing 31 of the 87 hospitalizations. The most frequent diagnoses were worsening of anemia (n = 11), VOCs (n = 9), upper airway infections (n = 8) and splenic sequestration (n = 6). Between 3 and 4 years, 9 of 33 children required transfusions, accounting for 17 of the 60 hospitalizations and the main acute complication was VOC. Between 4 and 5 years, 16 of 32 children needed at least 1 blood transfusion, representing 30 of the 67 admissions, with the main acute complications being VOC and bacterial pneumonia.
We highlight 2 children that received 23 and 24 blood transfusions. One child had 24 hospitalizations, mainly due to splenic sequestration during the first 2 years of life. The other child had 16 hospitalizations, 10 after the first 3 years of life and almost all related to VOC and worsening of anemia.
In 23 hospitalizations (6.8%) a CVC was needed and the main diagnoses were bacterial pneumonia (n = 7) for antibiotic administration, osteomyelitis (n = 6) due to the need of long duration therapy and splenic sequestration (n = 6) regarding its severity and requirement of a central line to manage fluids and blood transfusions. Two children with sepsis and one child with meningitis also required placement of CVC due to the severity of the presentation and hemodynamic compromise requiring fluids and antibiotic treatment.
Respiratory support was needed in 7.1% hospitalizations (n = 24). The majority (91.6%) required simple oxygen therapy, mainly due to a respiratory infection. One child needed intubation and other required non-invasive ventilation due to splenic sequestration.
Five children (7.1%) needed social support and the main reason was economic shortage.
There were no sequelae or deaths.
With the data provided, the authors tried to perform statistically significant correlations.
The first correlation we tried to find was between the different contexts of diagnosis (neonatal screening, hospitalization and consultation) and the number of hospitalizations but, as shown in the boxplot (Figure 1), it was not possible to establish a significant variance between the 3 groups.
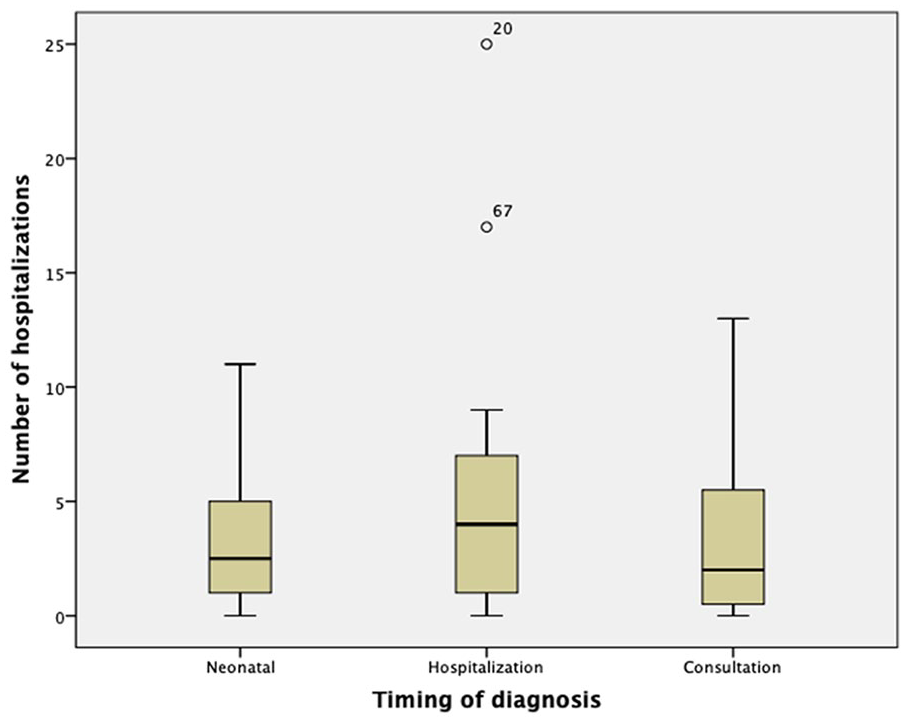
Comparison between the number of hospitalizations and the timing of diagnosis (boxplot).
Another correlation was between age of diagnosis and the number of hospitalizations through the use of ANOVA test (Figure 2), but it was also not possible to establish a significant correlation (P-value .333).

Correlation between number of hospitalizations and age of diagnosis, in months (ANOVA test).
Discussion
The vast majority of children in our study were homozygous for HbS (HbSS), which is the most prevalent form of SCD, and were of African descent, which is also in agreement with the literature.
A large number of children were diagnosed through selective neonatal screening, an essential tool that, since 2013, has been performed at our hospital. If we only consider the diagnoses established from that time, the percentage of children diagnosed through neonatal screening rises. This shows that more frequently the diagnosis is establish earlier and this is of paramount importance since an early diagnosis allows a sooner intervention and follow-up. The median diagnosis age was 6 months, with only 3 children being diagnosed after the age of 2 years (children that came from African countries and arrived in Portugal after 2 years old undiagnosed). This highlights the disparity of resources between develop and underdeveloped countries, as can be seen in a study recently published by a sickle cell center in the Democratic Republic of Congo, where the median diagnosis age was 2 years (IQR: 1-5), with only 37% being diagnosed under 12 months, with no neonatal screening. 10
It was not possible to correlate the age of diagnosis and the number of hospitalizations, although it would make sense that an earlier diagnosis would be associated with fewer hospitalizations. This was not possible probably due to the small sample and the criteria established.
Regarding hospitalizations, each child had an average of 4.81 hospitalizations with a mean duration of 5.36 days. This means that until the age of 5, each child spends approximately 3 weeks of their life hospitalized. In the majority of cases, the first hospitalization occurred before reaching 2 years.
The most frequent reason for hospitalization was VOCs, which is in accordance to the 58% of VOCs reported by Neonato et al in a study conducted in 299 patients with homozygous sickle cell anemia from 4 Parisian specialized centers, and the 90% reported by Brozović et al in a study of 221 British patients with SCD.11,12 The majority of children hospitalized in our study had at least 1 VOC and there were 4 children with 7 or more VOCs. VOC is usually associated with extreme pain and has a great impact in the quality and daily life of these children.
In our study, the most common location of VOC was abdominal followed by lower limbs. In a study reported by Brozović et al the location of VOC was divided in to 2 groups and per age group (<5 years; 5-16 years; >16 years). The limb pain was the most frequent in children under 5 years and included long bones, hip, and shoulder joints while the trunk pain was less frequent and referred to the vertebrae, pelvis, ribs, and abdomen. 11 In our study, we have 49.2% children with trunk pain versus 46% with limb pain, which is not in accordance to what was reported in the previously study, if we consider the same age group (<5 years). There is not a lot of research regarding this aspect, so further studies are required to assess the most frequent locations of VOC, specially per age group.
Approximately a third of the VOCs were associated with fever or an infectious intercurrence, which makes sense considering that infection is one of the main triggers for this complication. 8
Fever, upper airway infection and bacterial pneumonia were the next most frequent complications. Children with SCD have splenic dysfunction since early ages which makes them more susceptible to infections and this is in accordance with the obtained data. 8
Splenic sequestration was present in 10% of hospitalizations and it is a potential life-threatening complication that usually occurs in the first years of life, which reinforce the need to suspect this diagnosis and also the importance of parent education in this field.
The most frequent hemoglobin values at admission were between 6 and 9 g/dL, with 5% below 5 g/dL. The criteria to perform blood transfusion according to the guidelines were an acute drop of 2 g/dL from the baseline or the presence of hemodynamic instability. The majority of children in our study had at least 1 blood transfusion. In a study performed in the United States where the goal was to access the need of transfusion per hospitalization in children under 18 years with SCD from 1997 and 2009, it was possible to verify an increasing trend in blood transfusions amongst hospitalized children, with 26.6% requiring a red blood cell transfusion in 2009 compared to 14.2% in 1997. The most common diagnosis was VOC (56%). 13 In our study, the main acute complication related to the need of transfusion was splenic sequestration, mainly during the first 2 years. After that period, worsening of anemia due to an infectious condition and VOC were the most common causes. This difference between studies probably translates the age group studied.
Red blood cells transfusions are critical in managing acute complications in SCD patients, however they can lead to certain complications namely alloimmunization, infections and hemosiderosis. Clinical and laboratory manifestations of hemosiderosis can be seen after 20 blood transfusions and we highlight 2 children in this study that had already undergone more than 20 transfusions.
During the study period, a small percentage of children (6.9%) were under hydroxicarbamide therapy. This is one of the only treatments available and the indications for its use have been changing in the recent years, with the most recent studies suggesting its introduction at 9 months of age. Considering that our study began in 2010, the majority of children did not fulfill the criteria needed. More recently, new research and studies reveal its potential to minimize complications and therefore hospitalizations, being a safe and efficient medication. It would be interesting to evaluate these conclusions in the following years.
Conclusion
SCD is a complex disease that is associated with multiple and varied complications, some life-threatening, with potential sequelae, and for this reason it is of utmost importance to have an early diagnosis which allows an earlier use of medication and vaccination, and therefore, a more controlled disease with, hopefully, fewer complications and comorbidities.
The authors performed this study in a developed country with easy access to regular follow-up, treatment and a high rate of immunization and even though no child presented with serious sequelae or deaths, the acute complications requiring hospitalization were frequent. Therefore, SCD carries a significant psychosocial burden not only for the patient but also their caregivers and family, so it is very important to know what patients/caregivers feel about this disease and their quality of live. It is also important to mention the economic burden for the family and the national public health service. Social support is crucial in this disease and should be available and provided.
Footnotes
Authors’ Note
It was presented as an online poster at the 15th Annual Sickle Cell and Thalassemia & 1st EHA European Sickle Cell Conference.
Author Contributions
All authors are responsible for the reported research and have participated in the concept, design, analysis and drafting of the manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.