
Abstract
Introduction. Childhood illnesses not only affect the child, but also the family members. Objective. The purpose of this study was to investigate the guilt, uncertainty, education needs, and knowledge of mothers with children experiencing precocious puberty. Methods. Data were collected in August, 2017. The participants of the study were the mothers of children experiencing precocious puberty. A total of 111 copies of questionnaires were collected. Descriptive statistics, independent t-test, one-way ANOVA, Pearson’s correlation coefficient were used for the analysis, using the SPSS 24.0 program. Results. Mothers of children experiencing precocious puberty require psychological interventions that can alleviate their guilt and uncertainty, as well as enhance their knowledge of the emotional support needed by their children. Conclusion. Mothers with children experiencing precocious puberty had a high level of education needs to know, but the knowledge they knew was insufficient. Future studies need to focus on developing education programs for mothers dealing with their child’s precocious puberty.
Introduction
The rising incidence of precocious puberty is attributed to the growing rate of childhood obesity, environmental pollution, and disruptions of the endocrine system resulting from a heightened exposure to environmental hormones 1 . In South Korea, the number of children undergoing treatment for precocious puberty has increased in the past 5 years, from 55 333 in 2012 to 86 352 in 2016, implying an annual mean increase of 11.8%. Additionally, the costs of medical treatment increased by 10.6%, from 24 745 762 dollars to 36 949 152 dollars (about 1.5 times higher), over the same time period. 2
The definition of precocious puberty is the development of secondary sexual characteristics (onset of telarca in girls and increase in testicular volume >3 ml in boys) before 8 years of age in girls and 9 years in boys. 3 It may seem to be a temporarily accelerated pubertal development, but this closes the growth plate early, inhibiting the chances of reaching the mid parental height. 3 Such children appear more mature than their peers, their physical growth is faster than their mental maturity. They experience psychological problems such as depression, 4 high anxiety levels, and negative body image. 5 They have an increased probability of problematic behavior like aggression, conflict with parents, and school maladjustment.6,7 It is therefore important for parents to carefully monitor their children, to identify the symptoms of precocious puberty early and seek appropriate treatment.
Symptoms of Pp not only affect the child, but also the family members. 8 Children and their parents are equally uncomfortable with the unexpected accelerated puberty.7,9,10 Dealing with symptoms exhausts family members, and uncertainty in the course of treatment 11 eventually increases stress levels. Amongst the family members, it is the mother who is the primary caregiver, playing the most important role in the child’s care and greatly influencing the child’s growth and development. 8 Mothers too have to endure the manifestations of the child’s physical symptoms and secondary sexual characteristics, as well as the process of the treatment. 12 They feel guilty for not doing their part well 13 and experience anxiety and depression about an uncertain future. 14
Although the mothers’ difficulties are heightened, as more number of children are being diagnosed with precocious puberty, the related research is insufficient. Most previous studies were mainly about the diagnoses of and treatment for the condition,11,15 the causes and characteristics,11,16 and the risk factors of precocious puberty. 17
Children experiencing precocious puberty spend lots of their time at home, in their mothers’ care while undergoing outpatient care according to the treatment plan. For this, it is necessary to identify the characteristics of mothers with such children and investigate their expectations from the education. The purpose of this study is to identify the psychological characteristics of mothers with children experiencing precocious puberty and to analyze the degree of knowledge and education they want to know. This aims to provide basic data on precocious puberty education programs.
Methods
Research Design and Participants
This is a descriptive research. The participants of this study were mothers whose children were experiencing precocious puberty. These were children admitted to the outpatient clinic of pediatrics and adolescence at a university hospital in South Korea. The selection criteria were: (1) mothers of children diagnosed with precocious puberty and who had no problems in deciphering the Korean language, (2) who understood the purpose and contents of the study, and (3) who agreed in writing, to participate. The sample size of the participants, needed for the correlation analysis was calculated using the G*Power3.1.9.2 program according to Cohen’s formula. 18 The minimum sample size was 109 when set to 2 tailed, α = .05, 1 − β = .9, and medium effect size was 0.3. Thus, 120 mothers were surveyed, including the dropouts. A total of 111 mothers (93%) were factored in for the final analysis, except those with insufficient responses.
Research Tools
Guilt
The tool for measuring the guilt of the mothers was developed by Kwon et al 19 , to measure the guilt of the mothers of children with rare genetic metabolic disorders. 19 We did so, after receiving the permission through an email.
This tool categorized based on the 4 concepts of blame, responsibility, punishment, and impotence. The contents include, “It seems to be my fault that my child is sick,” implying blame; “Sometimes I feel like there is something that I have done wrong,” implying responsibility; “At times I think that I am being punished because I have sinned,” implying punishment; and “There are times when I think that there is not much I can do for a sick child,” implying impotence. Thus, a total of 4 items were used for the guilt measurement, with a 5-point Likert scale. The higher the score, the more the guilt. In Kwon et al ’s 19 study, the reliability of the tool was Cronbach’s α = .88. In this study, it was Cronbach’s α = .86.
Uncertainty
The measuring tool for uncertainty used in this study was translated, modified, and supplemented by Oh 20 from Mishel’s 21 Parent Perception of Uncertainty Scale (PPUS). Permission was granted via an email.
The measurement tool consisted of 3 sub-domains and 18 items in total, with 10 items for ambiguity, 5 for unpredictability, and 3 for reliability of the medical staff. This tool measured using a 4-point Likert scale. The higher the score, the higher the uncertainty. The reliability of the tool was Cronbach’s α = .83 in Oh’s 20 study and Cronbach’s α = .82 in this study.
Education Needs
The tool for measuring the education needs was developed by the researcher due to the lack of an already existing one. Unlike the previous studies, open ended questions were put forth, to investigate the education needs. The tool was developed as follows:
Step One
The data on what the mothers wished to learn were derived through interviews, prior to which, the purpose of the interview was explained and the written consents were collected. A total of 15 mothers who agreed to this procedure were interviewed. Participants answered the open question “Please write freely about any education or programs needed for children and mothers experiencing precocious puberty.” The researcher developed the questionnaire based on these interviews and the completed open-ended questionnaires.
Step Two
Based on the data collected in step one, the items were listed. A professor of Child Nursing, a pediatric doctor, and a pediatric nurse chose 19 items with the Content Validity Index (CVI) 0.8 or higher, after reviewing the validity of the contents. The education needs tool was then classified into 4 sub-domains: “disease information,” (5 items); “health care method,” (5 items); “treatment information,” (5 items); and “emotional support” (4 items). A 5-point Likert scale was used. The reliability of the tool was Cronbach’s α = .93.
Knowledge
The knowledge of the mothers needed to be analyzed along with their education needs so that a desirable educational program could be developed in the future. Thus, their knowledge was measured using the same items as their education needs. Hence, this tool also had 19 items, with 4 sub-domains namely, “disease information,” (5 items); “health care method,” (5 items); “treatment information,” (5 items); “emotional support,” (4 items) using a 5-point Likert scale. The reliability was Cronbach’s α = .96.
Data Collection
Preliminary Investigation
A preliminary survey was conducted in May, 2017 with 15 mothers, for developing a tool for this study (Education needs and Knowledge). The preliminary survey was conducted after the researcher directly explained to the participants, the purpose, procedure, withdrawal of the study, and received their written consent. The interview for the preliminary survey was conducted in a counseling room, for comfort and privacy. Each interview lasted for approximately 20 minutes.
Main Investigation
Data were collected through questionnaires in August, 2017, from those mothers whose children visited a clinic of pediatrics and adolescence in a university hospital, as outpatients. Before the survey, the researcher thoroughly explained the purpose and necessity of the research, the time required for the questionnaire (about 15 minutes), and the ability to withdraw at any time. The data were collected by 1 researcher, utilizing the hospital’s counseling room.
Data Analysis
The collected data were coded and analyzed using IBM SPSS Statistics, 23.0 version. The participants’ general and disease related characteristics, guilt, uncertainty, education needs, and knowledge were analyzed using descriptive statistics. Their differences in guilt, uncertainty, education needs, and knowledge based on their general characteristics were analyzed using the independent t-test or 1-way ANOVA, and the post-hoc test was analyzed with Tukey’s test. The correlations among guilt, uncertainty, education needs, and knowledge were analyzed using Pearson’s correlation coefficient.
Ethical Consideration
Informed consent was obtained from all subjects involved in the study. The participants were well-informed about the purpose and contents of the study, the right to reject participation, and how their data would be protected. Their personal information (like, telephone and mobile phone number) and the study-related information obtained from them, was used for research purposes only. Data were collected only after an approval from the Bioethics Committee of the researcher’s institution.
Results
General Characteristics of the Participants
The average age of the mothers was 41 years. The average education level was college (73.0%), and the ratio of working mothers (64.0%), was high. Their average age of mothers’ menarche was 13 years (Table 1). The mean age of participant of this study was 9.89 years. And 91.0% for girls and 9.0% for boys. Based on the age-based obesity index, there were 52.3% overweight and 47.4% normal weight children. The average time for treatment was 13.7 months, and 10.8% were cases with a family history in precocious puberty. Out of them, 10.8% of the patients received other therapies (oriental medicine, folk remedies). Out of the participants, 38.7% were actively helped by their families in dealing with precocious puberty, and 61.3% of them were not (Table 1).
Differences in Guilty and Uncertainty According to General and Disease Related Characteristics (n = 111).
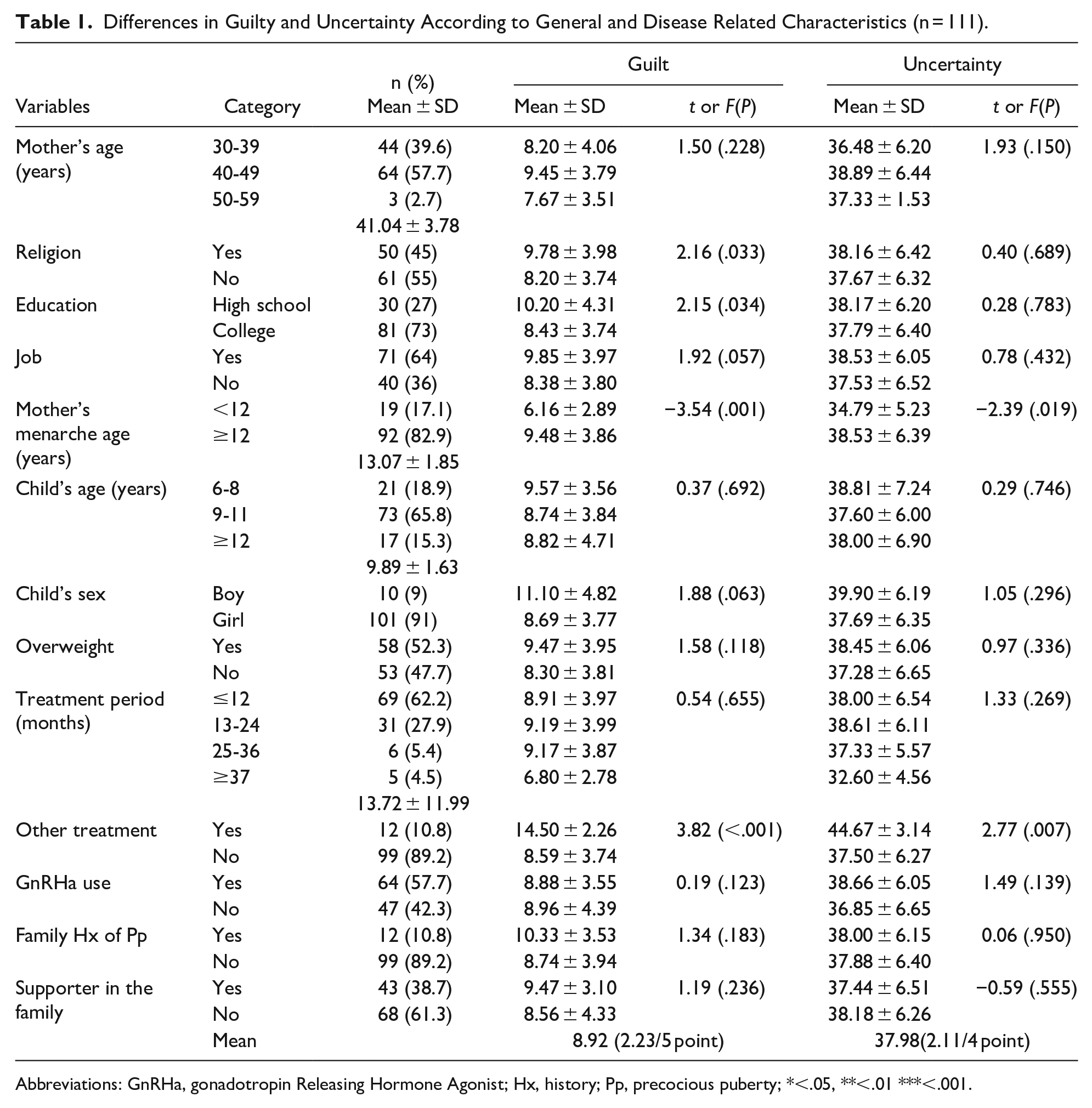
Abbreviations: GnRHa, gonadotropin Releasing Hormone Agonist; Hx, history; Pp, precocious puberty; *<.05, **<.01 ***<.001.
Differences in Guilt and Uncertainty According to General and Disease related Characteristics of the Participants
The mothers were significantly more likely to have guilt when they were religious (t = 2.16, P = .033) and the education level being high school (t = 2.15, P = .034), compared to the ones who were religion-free and graduates, respectively. The guilt (t = −3.54, P = .001) and uncertainty (t = −2.39, P = .019) were significantly higher in mothers with a menarche age more than 12 years, compared to the ones with menarche age less than 12 years. The guilt (t = 3.82, P < .001) and uncertainty (t = 2.77, P = .007) were significantly higher for the mothers whose children were treated with oriental medicine or folk remedies, compared to those whose did not. The mean guilt stood at 2.23 (±0.98). The uncertainty was at an average of 2.11 (±0.35) (Table 1).
The education needs of those mothers were significantly higher (t = 2.43, P = .017), whose children were treated with oriental medicine, or folk remedies. The cases with children experiencing precocious puberty had a duration of at least 37 months (F = 3.95, P = .010), and the cases wherein the family actively helped (t = 2.53, P = .013), the mother’s knowledge was significantly higher (Table 2).
Education Needs and Knowledge, Based On General Characteristics.

Abbreviations: GnRHa, gonadotropin releasing hormone agonist; Hx, history; Pp, precocious puberty; abelow 12 month, b13-24 month, c25-36 month, dabove 37 month; **p<.01; a,c<d** Group d is significantly higher than group a and group c.
Tukey.
Education Needs and Knowledge of the Participants
The average education needs of the mothers was 4.05 points (out of 5). The average sub-domain scores were, 4.23 for “emotional support,” 4.21 for “treatment information,” 4.10 for “health care method,” and 3.71 for “disease information.” For the detailed items the scores starting with the highest, under education needs were, 4.43 for “safety of precocious puberty medicine.” The mean score for the knowledge of the mothers was 2.48 (out of 5). The mean scores for knowledge by sub-domains, starting with the lowest, were 2.08 for “emotional support,” 2.46 for “treatment information,” 2.63 for “health care method,” and 2.66 for “disease information.” Under the detailed items, the scores from lowest to the highest were, 2.05 for “stress management for mothers of children experiencing precocious puberty,” 2.07 for “stress management for children experiencing precocious puberty” (Table 3).
Education Needs and Knowledge of Participants (n = 111).

Abbreviations: Pp, precocious puberty; Sub-total, Average by category.
Correlations Among the Guilt, Uncertainty, Education Needs, and Knowledge of the Participants
The guilt of mothers with children experiencing precocious puberty was found to have a significantly positive correlation with uncertainty (r = .54, P < .001), and education needs (r = .30, P = .002). The uncertainty of the mothers had a significantly positive correlation with education needs (r = .26, P = .005). On the other hand, the education needs of the mothers had significantly positive correlation with knowledge (r = −.39, P < .001). The higher the mother’s knowledge, the lower the education needs (Table 4).
Correlations Among Guilt, Uncertainty, Education Needs and Knowledge (n = 111).

Discussion
The average guilt of the mothers, stood at 2.23 points (out of 5), similar to the guilt score of 2.62 in a previous study 22 using the same measurement tool. The guilt of a mother with precocious puberty child is closely related to stress and anxiety, and the guilt is significantly reduced when applying social support. 13 Proper care of mother improves precocious puberty, 23 so psychosocial interventions should be provided to help mothers with precocious puberty to provide adequate care.
The uncertainty score was 2.11 (out of 4), which was lower than the uncertainty score of 2.37 of the mothers of hospitalized children, measured using the same tool. 20 The anxiety of the mothers of children experiencing precocious puberty was 3.68 points (normal: 0-3; mild: 4-6), the stress was 8.68 points (normal: 0-7; mild: 8-10) along with a report that corresponds to “mild.” 14 Evidently, the uncertainty, anxiety or stress of such mothers was not excessively high, although it was outside the “normal” range. This is because of the psychocentric problems arising out of the uncertainties around the long-term treatment for precocious puberty. However, while the treatment is ongoing, it is not perceived as an emergency treatment or a life-threatening situation.
The sub-domains of education needs are classified into 4 categories namely, “disease information,” “health care method,” “treatment information,” and “emotional support.” Among these, education needs were the highest for “emotional support,” but their knowledge was the least. Within “emotional support,” their education demand for the stress management of their children was the highest, while their knowledge regarding their own stress management was the lowest. Mothers who play an important role in childcare have heavy mental burdens and education needs, but lack the knowledge, revealing their difficult lives. Any future development of individualized programs for such mothers should also include the provision of information and emotional support.
An analysis of the differences in the general characteristics of the participants revealed that the guilt, uncertainty, and education needs were significantly higher when the mother experienced other therapies (oriental medicine, folk therapy) besides the main treatment, for her child’s precocious puberty. Over-emphasis on an illness or the inability to make an accurate judgment and predict results exacerbates guilt and uncertainty. 21 In this study, the mothers seemed to have tried various treatments to overcome their guilt and uncertainty. The lack of accurate knowledge and information needed to determine the objective treatment seems to have led them to unproven approaches. This suggests, that the mothers should be provided with accurate disease-related information and guidance, to help them adopt effective and scientifically proven management methods.
This study also analyzed the various correlations. The guilt, uncertainty, and education needs had significantly positive correlations. However, there was a significant negative correlation between education needs and knowledge. This is consistent with the results of a previous study 22 wherein the mothers of such children showed higher levels of concerns and anxiety. The lack of studies on the relationship among the education needs, knowledge, and psychological variables (guilt, uncertainty), limits our discussion. In this study, the mothers faced difficulties regarding the correct treatment for precocious puberty post diagnosis, which naturally increased their demand for education. Thus, higher educational needs signified lower knowledge. Further, higher demand for knowledge signified lesser knowledge. Future studies thus need to investigate why, despite a high demand for the knowledge, there is an overall deficiency of it.
As this study further indicates, the educational programs for children experiencing precocious puberty and their families should not only include disease-related information, but also information that could cater to their psychological stability. A limitation of the study is a lack of data regarding diagnosis (type of Pp, idiopathic, caused by brain lesions or other causes), it is necessary to consider the data on diagnosis and treatment later.
The results of this study cannot be generalized because it analyzed the data collected through convenience sampling. Another reason is that the participants were not selected keeping specific family-related categories like single parents, grandparents, and multicultural families, in mind. Nevertheless, it is significant that the mother’s psychological characteristics, education needs, and knowledge were analyzed. Particularly, in the preliminary survey, through an open-ended questionnaire, we directly collected the mothers’ desired contents of education and used this to create a questionnaire. This could be a useful resource for developing educational programs, as it reflects the needs of the participants. We aspire for the results of this study to be used as basic data for developing family-centered education programs for children experiencing precocious puberty.
Conclusion
The guilt and uncertainty of the mothers were found to be slightly high. While indicating high education needs, their knowledge was low. This study is significant in terms of factoring in the psychological aspects of the mothers and systematically grasping their needs. In particular, their education needs and knowledge about precocious puberty showed a significantly negative correlation, suggesting that the participants had a high level of education needs to know, but the knowledge they knew was insufficient. This suggested that specific education and psychological interventions are needed for the mothers. Future studies need to focus on developing education programs for mothers dealing with their child’s precocious puberty. Further, it is important to research interventions for children, to promote their healthy growth, post diagnosis.
Footnotes
Author Contribution
Conceptualization, H.Y.A and K.H.Y.; Methodology, M.R.S.; Software, K.H.Y.; Validation, H.Y.A. and M.R.S.; Formal analysis, H.Y.A.; Investigation, K.H.Y.; Resources, K.H.Y.; Data curation, H.Y.A. and K.H.Y.; Writing—original draft preparation, H.Y.A. and M.R.S.; Writing—review and editing, M.R.S.; Project administration, H.Y.A.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Institution Review Board statement
Data were collected only after an approval (IRB No.: EU17-09; Approval date: February 3, 2017) from the Bioethics Committee of the researcher’s institution.
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.