
Abstract
Introduction. Nephrotic syndrome (NS) is a kidney disease characterized by albuminuria, hyperlipidemia, edema, and hypoalbuminemia. Above 20 % of nephrotic children do not show response to steroid treatment. Molecular markers controlling apoptosis have not been studied as a predictors of steroid resistant NS (SRNS) and steroid sensitive NS (SSNS) in children. Aim of the Study. To identify clinical and molecular markers which define and predict the steroid-resistance phenomenon in children with NS. Methods. Fifty-six clinical cases of children hospitalized in Pediatric Hospital No. 7 (Kyiv, Ukraine) with NS (26 SSNS and 30 SRNS) studied. Stepwise logistic regression models used to analyze data. Data processed using GraphPad Prism 9.0 Software for Windows (USA, San Diego, CA). Results. Arterial hypertension, WBC and RBC count, serum creatinine, serum urea, serum cholesterol found to be factors defining and predicting SRNS. Apoptosis regulating BcL-xL, Bax but not caspase-8 found to be those defining SRNS. Among transcriptional factors HIF-1alfa selected as a factor predicting steroid resistance phenomenon. For SSNS group significant negative correlation observed between BcL-xL and Bax, BcL-xL and caspase-3, significant positive correlation observed between marker of cellular hypoxia HIF-1alfa and proapoptotic factor caspase-3. For SRNS group significant negative correlation observed between BcL-xL and Bax, BcL-xL and caspase-3 level, significant positive correlation observed between HIF-1alfa and proapoptotic factor caspase-3. Conclusions. Arterial hypertension, serum creatinine level, serum urea level, serum cholesterol level, WBC and RBC count, BcL-xL, Bax, caspase-3, and HIF-1alfa identified as candidate biomarkers to predict and define SRNS in pediatric NS.
Introduction
Nephrotic syndrome (NS) is the most common glomerular disease in childhood. Nephrotic syndrome is a syndrome characterized by increased glomerular filtration barrier permeability. It classically presents with heavy proteinuria (Urine protein excretion >50 mg/kg/day or a spot urine sample with albumin/creatinine ratio (UACR) greater than 3 g/g creatinine), hypoalbuminemia (serum albumin <3 g/dL), edema, and hyperlipidemia. 1
The prevalence is 12 to 16 per 100 000 children aged under 16 years. The reported incidence in children varies between 1.2 and 3.5 per 100 000 per year in Western Europe, 4.7 per 100 000 per year worldwide. 2 Although more than 85% of children with nephrotic syndrome respond to corticosteroids, approximately 10% to 15% remain unresponsive or later become steroid-resistant. Steroid-resistant nephrotic syndrome (SRNS) has been associated with negative renal prognosis. Approximately 36% to 50% of patients progressing to end-stage kidney disease within 10 years. 3
Steroid-resistant nephrotic syndrome is not a single entity. 4 Different factors discussed in term of steroid-resistance formation, that is, pathomorphological type of disease (the most dominant lesion is focal segmental glomerulosclerosis (FSGS),3,4 genetic markers, 5 metabolic factors. 6
This study aimed to investigate basic clinical (age, gender, blood pressure), basic clinical (serum creatinine, serum urea, serum cholesterol, complete blood count data, GFR, proteinuria), markers of apoptosis (BcL-xL, Bax, caspase-3, caspase-8), transcriptional factors (HIF-1alfa, NF-kappa B, Mn-SOD) as possible predictors of steroid resistance in children with NS.
Material and Methods
Patients
This case control study was carried out in the duration from June 2018 to August 2020. The study was conducted on 56 selected patients with NS collected from the nephrology department, Padiatric Clinical Hospital No. 7 (Kyiv, Ukraine) which is a clinical base of the Bogomolets National Medical University. An informed written consent was obtained from the parents of all participants. The study was approved by the local ethical committee of Bogomolets National Medical University and the research is complied with Helsinki Declaration.
Patients were also subjected to physical examination to document fever, edema, ascites, nutritional status, volume status, and hypertension. The laboratory data including; complete blood count, serum creatinine (Scr), serum urea, serum cholesterol, eGFR using Schwartz formula, 24 hours urine protein, urine analysis.
Patients Characteristics
NS was diagnosed by the triad of heavy proteinuria (>3 g/day), hypoalbuminemia, and edema. The steroid-sensitive nephrotic syndrome (SSNS) group included 26 patients who responded to steroid treatment within 8 weeks. Steroid-resistant nephrotic syndrome was defined as a failure to respond to standard steroid treatment (2 mg/kg/day) for at least 6 weeks. All patients received the same dose of corticosteroid for 4 weeks (prednisolone 2 mg/kg/day), ACE inhibitors were only given to patients with hypertension. The patients were selected upon the outcome of 6 weeks of corticosteroid treatment. Patients with history of infection, high ASOT, hematuria, fever, protein energy malnutrition, and autoimmune diseases were excluded.
Immunoblotting for Detection of BcL-xL, Bax, NF-ĸB, Caspase-3, Caspase-8, NF-ĸB, HIF-1alfa, Mn-SOD
Tissue samples used to measure markers of apoptosis, intracellular hypoxia, anti-oxidative response. Proteins solubilized in Laemmli sample buffer were resolved in polyacrylamide gels by SDS-PAGE and transferred to a polyvinylidene difluoride membrane. Membranes were then blocked in 5% non-fat milk in TBS-T (136 mM NaCl, 10 mM Tris, 0.05% Tween 20) and immunoblotted using the Bcl-xL, Bax, NF-ĸB and HIF-1α Ab (Cell Signaling Technology, Danvers, MA USA) the caspase-3 and caspase-8 Ab (Cell Signaling Technology, Danvers, MA USA), MnSOD Ab (Abcam, Cambridge, Cambs, United Kingdom) for 1 hour at room temperature. The actin mouse mAb was used as a loading control. After 3 washes with TBS-T, the membranes were incubated with secondary anti-rabbit or anti-mouse antibodies labeled with horseradish peroxidase for 1 hour at room temperature. Membranes were washed 3 times with TBS-T. The protein bands were visualized by chemiluminescent substrate ECL. Quantification of the protein content was done by densitometric analysis.
Statistics
The data expressed as means ± SEM and as frequencies and percentages when appropriate. ANOVA followed by the post hoc test and nonparametric test (Mann-Whitney U test) were used to test significance of differences. Receiver operator characteristic (ROC) curves were constructed to assess sensitivity, specificity, and respective area under the curve. The optimum cutoff value was investigated by maximizing both sensitivity and specificity and minimizing the distance from the left upper corner of the ROC curves. Pearson correlation was run to study the correlation between factors regulating apoptosis. Regression analysis was performed to assess the studied parameter as potential predictors of steroid resistance. Data processed using GraphPad Prism 9.0 Software for Windows (USA, San Diego, CA). P values <.05 considered statistically significant.
Results
Patients
The study was carried out during the period over 24 months. 56 patients with NS were included in to the study. Twenty-six children had SSNS and 30 had SRNS. In the SSNS group the mean of patients ages was 11.2 ± 0.6, 53.3% of them were males, all of them had generalized edema, and 12 of them (46.2%) of them were hypertensive.
In the SRNS group the mean of patients’ ages was 11.0 ± 0.6, 66.6% of them were males, all of them had generalized edema, and 70% of them were hypertensive.
Clinical Characteristics of Patients with SSNS ans SRNS included into the study.

P < .05, **P < .01. Data presented as means ± SEM and percentages. Statistical analysis done using chi-square test.
The comparison of SSNS and SRNS patients’ clinical findings showed a statistically significant difference regarding the incidence of hypertension, which was evidently higher in the SRNS group (P value <.01). Major part of participants in SSNS and SRNS were boys (P < .05 and P < .05, respectively) (Table 1).
Basic Laboratory Biomarkers
Also, comparison of the laboratory findings showed statistically significant differences between SSNS and SRNS regarding WBC count—6.87 ± 0.47·109/L and 9.14 ± 0.47·109/L, respectively (P < .001). No difference in level of platelets count found in SSNS and SRNS—258.5 ± 11.5·109/L and 289.0 ± 11.5·109/L, respectively (P > .05) (Figure 1).

Complete blood count analysis in children with SSNS and SRNS. ***P < .001, ns: not significantly different. Histograms represent means ± SEM. Statistical analysis was performed using the Mann-Whitney U test.
Biochemical markers, that is blood urea, serum creatinine, serum cholesterol measured in all children. Serum creatinine and serum cholesterol found to be significantly different between the SSNS and SRNS groups. Serum creatinine concentrations documented at level 68.38 ± 3.46 µmol/L in children with SSNS and 80.23 ± 2.72 µmol/L in children with SRNS (P < .01). Serum cholesterol levels were higher in SRSN 11.97 ± 0.38 mmol/L children as compared to 9.89 ± 0.38 µmol/L in children with SRNS (P < .001). Blood urea levels were 9.99 ± 0.63 mmol/L and 11.08 ± 0.5 mmol/L (P > .05) (Figure 2).

Biochemical markers in children with SSNS and SRNS. **P < .01, ***P < .001, ns: not significantly different. Histograms represent means ± SEM. Statistical analysis was performed using the Mann-Whitney U test.
Glomerular filtration rate (GFR) and 24-h urine protein excretion were selected as markers of kidney function impairment. GFR found to be significantly lower in SRNS children as compared to children with SSNS—68.38 ± 2.72 mL/min/1.73 m2 and 82.84 ± 4.3 mL/min/1.73 m2 (P < .01). No difference found in proteinuria level when comparing SSNS group and SRNS group— 9.1 ± 0.71 g/24 h and 8.73 ± 0.59 g/24 h (P > .05) (Figure 3).

GFR and proteinuria levels in children with SSNS and SRNS. **P < .01, ns: not significantly different. Histograms represent means ± SEM. Statistical analysis was performed using the Mann-Whitney U test.
Apoptotic Markers in Children With Nephrotic Syndrome
The expression of proapoptotic and antiapoptotic factors were studied using immunoblotting. Bax, caspase-3 and caspase-8 were chosen as apoptotic markers, Bacl-xL as antiapoptotic.
Increased level of Bax expression in SRNS in comparison to SSNS documented—90.15 ± 2.0 mmol/L and 104.5 ± 3.o a.u., respectively (P < .01). Bax can initiate a cascade of events that eventually involves cleavage of caspase-3. Caspase-3 which is a final effector in mitochondrial level of apoptosis measured at level 131.1 ± 1.45 a.u. in children with SSNS and 141.4 ± 1.59 a.u. in children with SRNS (P < .001).
Caspase-8 selected as a proapoptotic marker and effector of the extrinsic apoptotic pathway. No difference in caspase-8 level found between SSNS and SRNS—37.3 ± 1.5 a.u. 139.6 ± 1.88 a.u., respectively (P > .05).
Significantly lower value of antiapoptotic factor BcL-xL found in children with SRNS in comparison to SSNS—SSNS and SRNS— 110.5 ± 1.84 a.u. 92.88 ± 2.74 a.u., respectively (P < .001). (Figure 4).
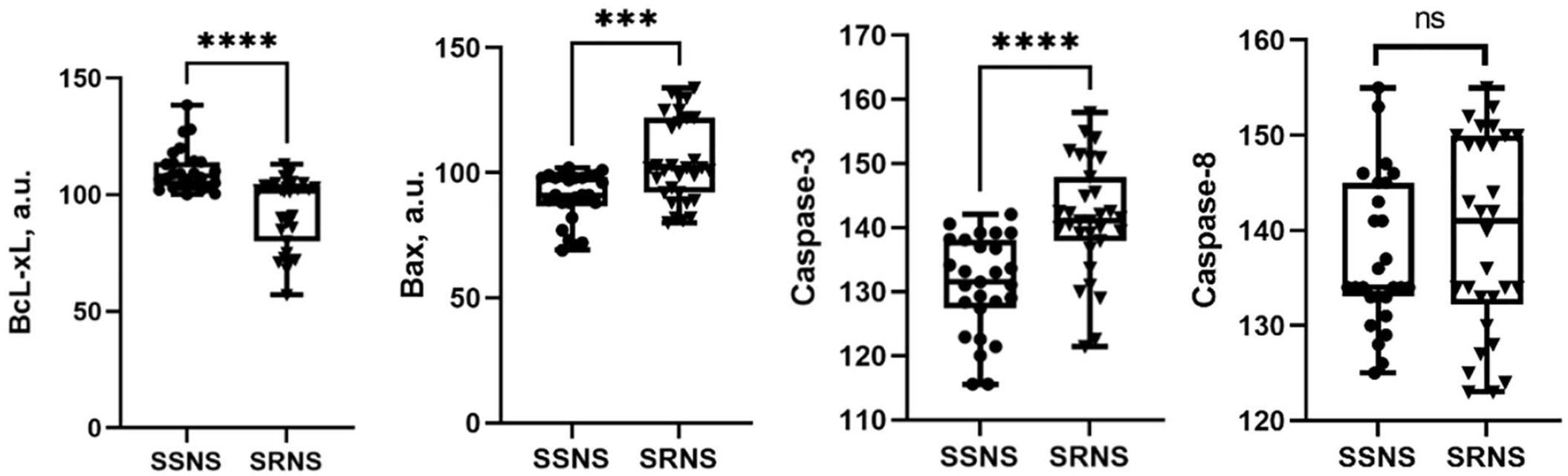
Levels of proapoptotic and antiapoptotic markers in children with SSNS and SRNS.
Beside apoptotic markers, studying of the NF-kB, HIF-1alfa, Mn-SOD done. NF-kB NF-κB is expressed in nearly all mammalian cells. Under physiologic (resting) conditions, NF-κB exists as an inactive form composed of a dimeric form of the transcription factor and its binding partner, IκB, which maintains NF-κB in an inactive form. NF-κB is activated in response to a various types of stress, including chronic inflamation. 7 We found that SRNS children have lower NF-kB level (107.3 ± 1.98 a.u) as compared to SSNS children (97.42 ± 3.34 a.u) (P < .05).
In mammalian cells, manganese superoxide dismutase (MnSOD) is the essential mitochondrial antioxidant enzyme that detoxifies the free radical superoxide, the major by-product of mitochondrial respiration. 8 Mitocholdrial respiration changes have place under inflammatory conditions. Level of Mn-SOD was significantly lower in children with SRNS and compared to SSNS—109.9 ± 3.0 and 95.16 ± 4.33, respectively (P < .05).
Finally, levels of HIF-1alfa as a marker of intracellular hypoxia studied in nephrotic children. 9 Significantly higher HIF-1alfa in children with SRNS in comparison to group with SSNS found—202.8 ± 4.44 a.u and 212.9 ± 2.14 a.u, respectively (P < .01) (Figure 5).

Levels of NF-kB, Mn-SOD and HIF-1alfa in children with SSNS and SRNS. *P < .05, **P < .01, ns: not significantly different. Histograms represent means ± SEM. Statistical analysis was performed using the Mann-Whitney U test.
Identification of Clinical and Metabolic Factors Defining and Predicting Steroid Resistance in Nephrotic Children
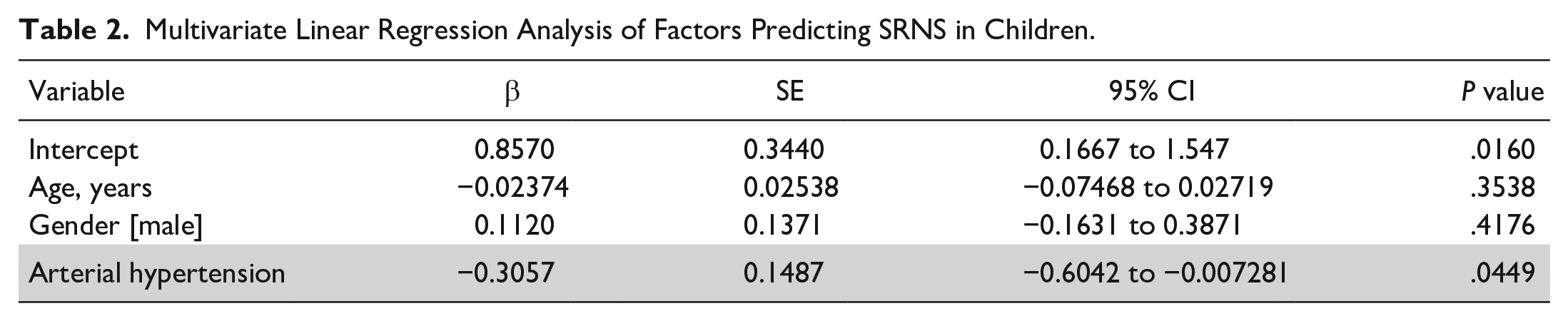
Multivariate linear regression analysis used to determine the clinical predictors of steroid resistance in nephrotic children among categorical factors. Demographic parameter, that is, age, gender and presence of arterial hypertension were included into analysis. Factor predicting SRNS these were identified arterial hypertension presence (β—0.31, SE 0.15, 95% CI −0.6 to −0.007, P < .05). None of other studied factors found as a predictors of SRNS—age (β—0.02, SE 0.03, 95% CI −0.07 to 0.03, P > .05), gender—(β 0.11, SE 0.13, 95% CI −0.16 to 0.39, P > .05) (Table 2).
Multivariate Linear Regression Analysis of Factors Predicting SRNS in Children.
Logistic regression models for the odds of steroid resistance among numerical factors in nephrotic children made using a step-wise selection procedure. Candidate predictors entering the model at P < .05. Three models created: (I) basic laboratory factors—RBC, WBC, PLT; (II) biochemical and factors: Serum creatinine, Serum urea, Serum cholesterol; Functional factors: GFR, proteinuria; (III) apoptosis controlling factors: Bax, BcL-xL, caspase-3, caspase-8; (IV)—transcriptional factors: NF-kB, HIF-1alfa, Mn-SOD. Receiver operating characteristics curve and area under the curve (AUC) analyses used to assess each model’s ability to define clinical steroid resistance.
Logistic regression analysis (Table 3) of basic laboratory factors selected WBC level (OR: 1.4; OR 95% CI: 1.12-1.85) and RBC level (OR: 1.14; OR 95% CI: 0.38-3.48) but not PLT count (OR: 1.0; OR 95% CI: 1.0-1.02) as a markers able to define the steroid resistance in nephrotic children (AUC: 0.75; SE: 0.06; 95% CI: 0.63-0.88; P < .001) (Figure 6A).
Logistic Regression Analysis of Factors Defining and Predicting SRNS in Children.

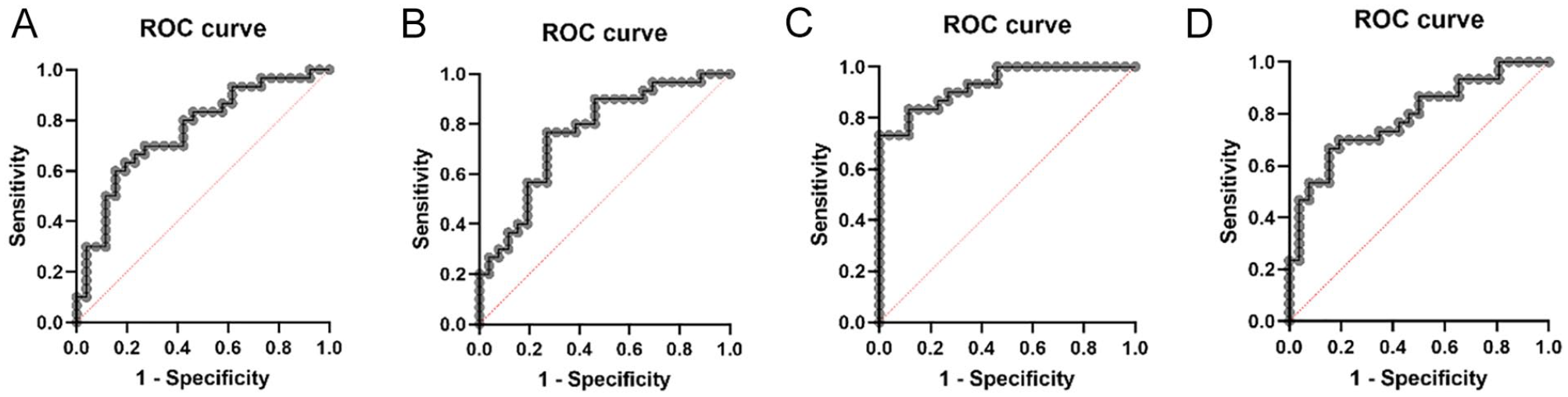
Receiver operating characteristics curve defining clinical steroid resistance. (A) basic laboratory factors—RBC, WBC, PTC; (B) biochemical and factors: Serum creatinine, Serum urea, Serum cholesterol; Functional factors: GFR, proteinuria; (C) apoptosis controlling factors: Bax, BcL-xL, caspase-3, caspase-8; (D)—transcriptional factors: NF-kB, HIF-1alfa, Mn-SOD.
Among biochemical factors and parameters showing kidney function impairment (Table 3) serum creatinine (OR: 1.04; OR 95% CI: 0.92-1.14), serum urea (OR: 1.14; OR 95% CI: 0.89-1.49), serum cholesterol (OR: 1.97; OR 95% CI: 1.37-3.18) were found to be a factors defining SRNS. GFR level (OR: 0.95; OR 95% CI: 0.87-1.04) and proteinuria level (OR: 0.85; OR 95% CI: 0.67-06) did not fit the model (AUC: 0.88; SE: 0.05; 95% CI: 0.78-0.97; P < .001) (Figure 6B).
Apoptosis regulating factors Bax, BcL-xL, caspase-3, caspase-8 (Table 3) were analyzed in terms of factors predicting SRNS. BcL-xL (OR: 1.4; OR 95% CI: 1.17-1.91), Bax (OR: 1.15; OR 95% CI: 1.04-1.37), caspase-3 (OR: 1.66; OR 95% CI: 1.27-2.68) but not caspase-8 (OR: 0.95; OR 95% CI: 0.84-1.05) (AUC: 0.93; SE: 0.03; 95% CI: 0.87-0.99; P < .001) fit the model (Figure 6C).
Finally, group of transcriptional factors NF-kB, HIF-1alfa, Mn-SOD included into the logistic analysis (Table 3). We found that HIF-1alfa, which is a marker of intracellular hypoxia selected as a factor defining steroid resistance phenomenon (OR: 1.02; OR 95% CI: 0.98-1.07). Nuclear transcriptional factor NF-kappaB (OR: 0.95; OR 95% CI: 0.9-1.01) and antioxidative factor Mn-SOD did not fit the model (OR: 0.95; OR 95% CI: 0.92-0.98)—(AUC: 0.78; SE: 0.06; 95% CI: 0.67-0.91; P < .001) (Figure 6D).
Pearson correlation was run to correlate principal factors found to be those defining steroid resistance in nephrotic children—Bax, BcL-xL, caspase-3, HIF-1alfa in both SSNS group (Figure 7A) and SRNS group (Figure 7B).
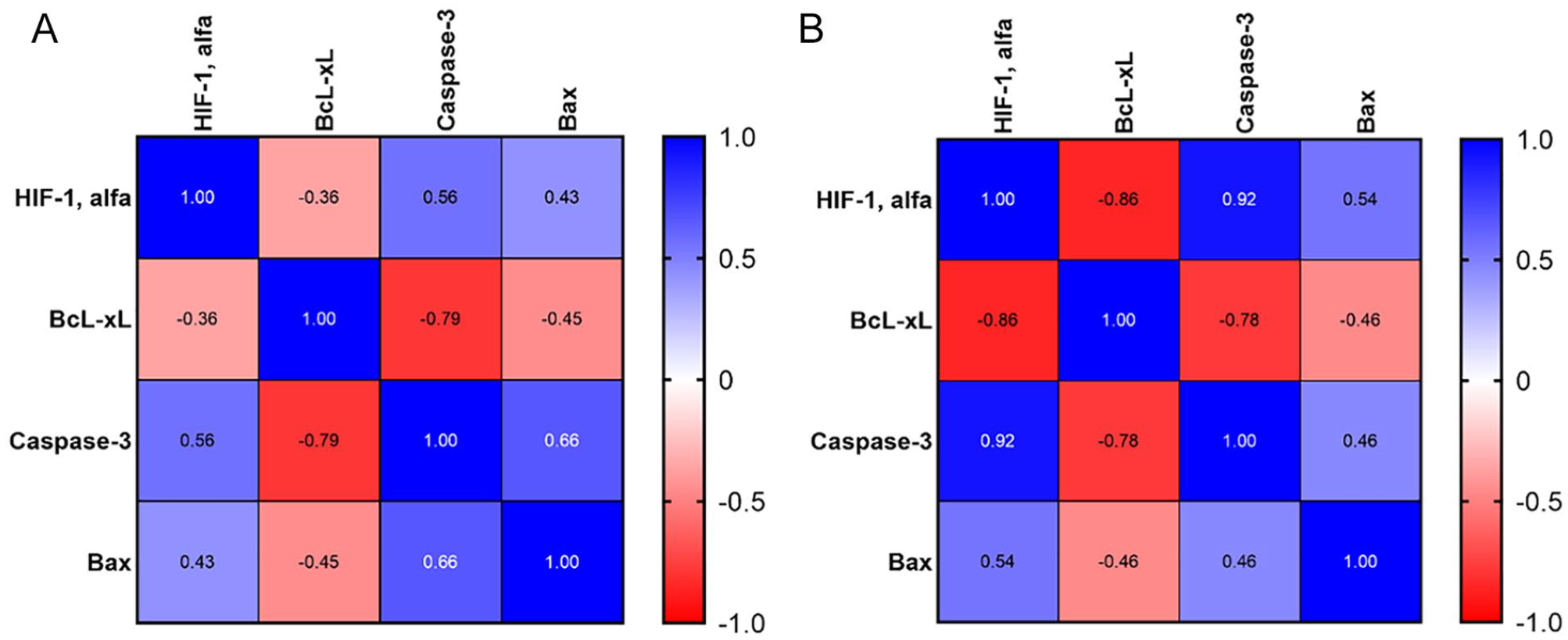
Heat map correlation between factors regulating apoptosis. (A)SSNS group and (B)SRNS group.
For SSNS group significant negative correlation was observed between antiapoptotic factor BcL-xL and proapoptotic factor Bax (r = −0.45, P < .05), significant negative correlation was observed between antiapoptotic factor BcL-xL and proapoptotic factor caspase-3 (r = −.79, P < .05), significant positive correlation was observed between marker of cellular hypoxia HIF-1alfa and proapoptotic factor caspase-3 (r = .56, P < .01) and proapoptotic factor Bax (r = .43, P < .05).
For SRNS group significant negative correlation was observed between antiapoptotic factor BcL-xL and proapoptotic factor Bax l (r = −.46, P < .05), significant negative correlation was observed between antiapoptotic factor BcL-xL and proapoptotic factor caspase-3 (r = −.78, P < .01), significant positive correlation was observed between marker of cellular hypoxia HIF-1alfa and proapoptotic factor caspase-3 (r = .92, P < .05) and proapoptotic factor Bax (r = .53, P < .05).
Discussion
Patients with SRNS have a more progressive disease course and poor outcomes when compared with SSNS patients. Different factors predicting and defining steroid resistance in nephrotic children discussed. Predictors of initial steroid resistance in study done by Kim et al 10 were age at onset, hypertension, and decreased kidney function.
Other research group identified creatinine concentration, malonate and glutamine concentration as 2 candidate biomarkers predictive of SRNS. In addition, paired-sample analyses done this study identified several candidate biomarkers with the potential to identify mechanistic molecular pathways/targets that regulate clinical steroid resistance, including lipoproteins, adipate, pyruvate, creatine, glucose, tyrosine, valine, glutamine, and sn-glycero-3-phosphcholine.
In study done by Bennett et al Vitamin D–binding protein (VDBP), alpha-1 acid glycoprotein 1 (AGP1), alpha-1 acid glycoprotein 2 (AGP2), alpha-1-B glycoprotein (A1BG), fetuin-A, prealbumin, thyroxine-binding globulin and hemopexin, and alpha-2 macroglobulin were measured and combined with urine neutrophil gelatinase–associated lipocalin (NGAL), which had been previously shown to distinguish patients with SRNS. A subset of 5 markers (including VDBP, NGAL, fetuin-A, prealbumin, and AGP2) showed significant associations with SRNS. 11
In our study we focused on general clinical parameters, markers of apoptosis, cellular hypoxia and antioxidant effector. Previously it was shown that apoptosis is a hallmark of proteinuria kidney diseases. Albuminuria, a well-documented predictor of progressive loss of kidney function, is considered a cause of kidney damage and loss of function.12-15
And the BCl-2 family has long been identified for its role in apoptosis regulation. The members of the Bcl-2 family are designated as such due to their BCL-2 homology (BH) domains and involvement in apoptosis regulation. The BH domains facilitate the family members’ interactions with each other and can indicate pro- or anti-apoptotic function. 16
Wada et al 17 shown that puromycine-induced podocyte apoptosis is p53 dependent and associated with changes in Bcl-2-related proteins and AIF translocation. The protective effects of dexamethasone on PA-induced apoptosis were associated with decreasing p53, increasing Bcl-xL, and inhibition of AIF translocation.
We analyzed levels of apoptotic family proteins in kidney material of children with NS. Our results show that level apoptotic factor Bax, apoptotic factor caspase-3 higher in children with SRNS and antiapoptotic factor BcL-xL level is lower in SRNS as compared to SSNS. No difference found in capse-8 level. Logistic regression model shows that BcL-xL, Bax and caspase-3 selected as factors predicting and defining SRNS.
Nuclear transcriptional factor NF-kB was downregulated in SRNS children as compared to SSNS group. NF-kB regulated Bax translocation to mitochondrial membrane and subsequently regulates apoptosis. Children with SRNS have lower NF-kB level as compared to SSNS.
We analyzed level of HIF-1alfa which is an important transcriptional factor regulating many cellular functions. 18 HIF-1 is a heterodimer composed of the rate limiting factor HIF1α and the constitutively expressed HIF-1β. 19
Nephrotic syndrome associates with chronic inflammation under the persistent influence of proteinuria. 20 Hypoxia can induce apoptosis by causing hyperpermeability of the inner mitochondrial membrane, which leads to the release of cytochrome C. The most direct induction of hypoxia induced apoptosis is the inhibition of the electron transport chain at the inner membrane of the mitochondria. The lack of oxygen inhibits the transport of protons and thereby causes a decrease in the membrane potential. The reduction of mitochondrial derived ATP causes activation of Bax, leading to caspase-3 activation. 21
Our results show that HIF-1alfa level was higher in SRNS children as compared to SSNS. At the same time children with SRNS have significantly lower level of Mn-SOD as compared to SSNS. Mn-SOD is an important player in apoptosis regulation via suppression of cytochrome c release. 22 We found that HIF-1alfa bur not NF-kB and Mn-SOD is a factor defining steroid resistance phenomenon in nephrotic children.
Correlation analysis shown significant negative correlation between antiapoptotic factor BcL-xL and proapoptotic factor Bax level, significant negative correlation between antiapoptotic factor BcL-xL and proapoptotic factor caspase-3, significant positive correlation was between marker of cellular hypoxia HIF-1alfa and proapoptotic factor caspase-3 and proapoptotic factor Bax. This relationship between principal factors regulating apoptosis observed in both SSNS and SRNS.
Finally, we hypothesize that apoptosis triggered by proteinuria in children with nephrotic syndrome depends on intrinsic mitochondrial pathway activation (Figure 8).

Signaling apoptotic pathway induced by proteinuria in nephrotic children.
The intrinsic apoptotic pathway is controlled by the family of Bcl-2 proteins. The mitochondrial apoptotic pathway is initiated by activation of Bax, a prominent pro-apoptotic member of the Bcl-2 family, to the outer mitochondrial membrane, where it oligomerizes and penetrates the inner mitochondrial membrane. This results in release of cytochrome C and caspase activation, the apoptotic executors. Bcl-xL, a prominent anti-apoptotic member of the Bcl-2 family, counteracts Bax accumulation on the mitochondria and Bax-induced permeabilization of the mitochondrial membranes.
Individual analysis of factors controlling apoptosis, that is, Bax, BcL-xL, caspase-3. HIF-1alfa, may have clinical significance in predicting and defining steroid resistance in nephrotic syndrome. Further investigations of other proapoptotic and antiapoptotic factors in children with NS is important in terms of finding new approaches of adequate treatment.
This study has certain limitations that must be presented. Our pilot study was cross-sectional, at a single center with somewhat limitation in patients. The strength is that enrolled patients were age-matched with no difference between SRNS patients and SSNS patients in disease duration. The strength of our panel to distinguish SRNS from SSNS (AUC 0.75-0.95; P < .0001) is high enough.
Footnotes
Author Contributions
IB: substantially contributed to conception or design; contributed to acquisition, analysis, or interpretation of data; drafted the manuscript; critically revised the manuscript for important intellectual content; gave final approval; Agree to be accountable for all aspects of the work in ensuring that questions relating to the accuracy or integrity of any part of the work are appropriately investigated and resolved. IM: substantially contributed to conception or design; contributed to acquisition, analysis, or interpretation of data; drafted the manuscript; critically revised the manuscript for important intellectual content; gave final approval; Agree to be accountable for all aspects of the work in ensuring that questions relating to the accuracy or integrity of any part of the work are appropriately investigated and resolved. IB: substantially contributed to conception or design; contributed to acquisition, analysis, or interpretation of data; drafted the manuscript; critically revised the manuscript for important intellectual content; gave final approval; Agree to be accountable for all aspects of the work in ensuring that questions relating to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work done with support from laboratories of Pediatric Clinical Hospital 6 and Pediatric Clinical Hospital 7, Bogomolets National Medical University.
Ethical Approval
The study conducted according to the guidelines of the Declaration of Helsinki. An informed written consent obtained from the parents of all participants. The study approved by the local ethical committee of Bogomolets National Medical University.
Data Availability Statement
The datasets generated during and/or analyzed during the current study are available from the corresponding author on reasonable request.