
Abstract
The research aimed at studying the mother’s social-hygienic and medical biological risk factors and determining their predictive value. The retrospective case-control study was conducted with 142 pregnant women participating in it. In the case group there were involved 92 mothers whose pregnancy was completed by the birth of a newborn baby suffering from the intrauterine growth restriction. The control group was made of 50 pregnant women, whose pregnancy was completed by the birth of a healthy neonate. The research resulted in specifying the risk factors of high priority: the low standards of living (OR 3.61), chronic stress (OR-3.06), sleeping disorder (OR-3.33) and poor nutrition (OR-3.81). As regards the coexisting pathology the following was revealed: endocrine pathology (OR-3.27), ischemic heart disease (OR-4.35), arterial hypertension (OR-6.47), iron deficiency anemia (OR-4.11), pathology of respiratory system (OR-3.42), chronic genital inflammatory and infectious processes. The preeclampsia (92%) and low amniotic fluid (89%) were detected to have the high predictive value. The awareness of risk factors allows us to employ the timely measures for the reduction of negative impact on the fetus and neonate.
The investigation of causes of forming the syndrome of fetal developmental delay is a topical issue of perinatology. The above mentioned is conditioned by increasing tendency towards the spread of disease, frequency of complications and negative impact on further health conditions of children. Fetal developmental delay was acknowledged as “the most common and complex problem of modern obstetrics”1,2 by Board of American Obstetrician- Gynecologists in 2013.
According to popular studies conducted in recent years the spread of fetal developmental delay equals to 10 to 44% on average. Based on the data of a number of authors, the disease is registered in every 10th pregnancy and 3 to 8% of newborn babies suffer from it. 3 Fetal developmental delay is related to high risk of perinatal illnesses: chronic hypoxia, hyperbilirubinemia (elevated bilirubin), hypoglycemia, respiratory and neurological disorders (12%). 4 Fetal developmental delay is the most considerable cause of neonates’ stillbirth, that accounts for fourfold increase of its coefficient.3,5 Decrease in cognitive function and the development of metabolic syndromes in children are considered to be long-term complications of the disease. 4
Nowadays, there exist a fair amount of information about etiology and pathogenesis of fetal developmental delay. Hypotrophy of fetus is a poly -etiologic process, in formation of which maternal (age, social-economic status, ethnic affiliation, somatic pathology, folate deficiency, pernicious habits etc.), placental (infarction, developmental anomaly, anomalous implantation, infectious placentitis), or fetal (constitutional peculiarities, gender, location, malformation, chromosomal aberrations, congenital anomalies, current infections following the pregnancy) factors perform the vital role. In 20% of cases the major cause of fetal developmental delay represents a genetic or infectious pathology.2,6,7
It is also worth noting, that risk factors have not been entirely systemized, the frequency and share of each factor in formation of syndrome is unknown. 8 The specific attention should be focused on mother’s risk factor, whose negative impact accounts for the disorder of placental angiogenesis, feto—placental insufficiency (dysfunction of placenta), metabolic disorders in fetus and newborn babies.9,10 The identification of maternal risk factors is a cornerstone of successful solution to this problem.
The research aims at studying the mother’s social- hygienic and medical-biological risk-factors determining their share and predictive value in forming fetal developmental delay.
Design of research
The hospital retrospective case-control study was conducted in a traditional design. The cohort of 92 mothers, whose pregnancy was completed by the birth of neonates suffering from intrauterine growth restriction, were involved in the case (main) group through applying the selection method.
The verification of syndrome of fetal developmental delay was based on the inconsistency of fetometrical data with the gestational age of fetus (less than 10th percentile after 18 weeks of pregnancy).
The control group consisted of 50 pregnant women, whose pregnancy was developing physiologically and was completed by the birth of a healthy neonate, whose anthropometric indicators corresponded to their gestational age.
Risk factors were studied through investigating pregnant women by cross-sectional study (medical history) and standard questionnaire. There were studied a mother’s demographic and social-economic indicators, obstetric anamnesis, extra genital and genital diseases, complications of pregnancy. The length of completing the questionnaire was 45 minutes on average.
The statistical analysis was conducted through using Microsoft Excel 2010 and SPSS/v15 software packages. In order to evaluate risk factors, odds ratio (OR) was studied on the basis of 95% confident interval (CI).
Findings
The cohort of 142 pregnant women of reproductive age were studied, 83 of them were Georgian (58,5%) and 59—of different nationalities (41,5%). The average age of participants was 27.1 ± 6.3 in the main and 27.2±5.8 in control group. The majority of participants represented civil servants (main group—54.4%, and control group—58%). Low level of education (21.7%), financial income (23.9%) and low standards of living (23.7%) were more frequently encountered in the main group. Table 1 shows quantitative indicators of maternal demographic and social-economic risk factors and their relative risk.
Demographic and Social-Economic Risk Factors Revealed in Studied Women (n = 142).

Based on findings, more than 2 indicators of odds ratio were revealed among single (OR-2.18) and Tabaco consuming mothers. According to P-data, low standards of living (OR-3.61, 95% CI 1.08-13.31, P-.034), chronic stress (OR-3.06, 95% CI 1.41-6.69, P-.004), sleeping disorder (OR-3.33, 95% CI 1.51-7.34, P-.002), and poor nutrition (OR-3.81, 95% CI 1.73-8.49, P-.001) proved to be statistically reliable.
It is worth noting, that regarding the coexisting extra genital diseases, obesity (50.0) and gastroenterologic diseases (55.4%) prevailed among the patients of main group, which 1.5 times exceeded the data of control group (32% and 46% respectively). See Table 2.
Extra Genital Pathology Revealed in Studied Women t (n = 142).

The high indicators of odds ratio were detected in case of existing endocrine pathology (OR-3.27, 95% CI −1.23-9.02, P-.014), ischemic heart disease (OR-4.35, 95% CI −1.45-13.92, P-.006), arterial hypertension (OR-6.47, 95% CI −2.63-16.29, P-.000), iron deficiency anemia (OR-4.11, 95% CI −1.80-9.42, P-. 001) and chronic pathology of respiratory system (OR-3.42, 95% CI −1.57-7.52, P-.002). Anemia was represented by extremely high share (80.4%), which denoted the sharp decline in the process of erythropoiesis. Anemia and iron deficiency in maternal and fetal organism cause the decline in ferment activation of respiratory system and even more strengthen placental insufficiency.1,11
In terms of coexisting genital pathology special attention was focused on chronic inflammatory and parasitic diseases. The frequency of inflammatory processes of genital system was higher in case of fetal developmental delay (main group 52.2%, control group 40%). See Table 3.
Genital Pathology Revealed in Studied Women.
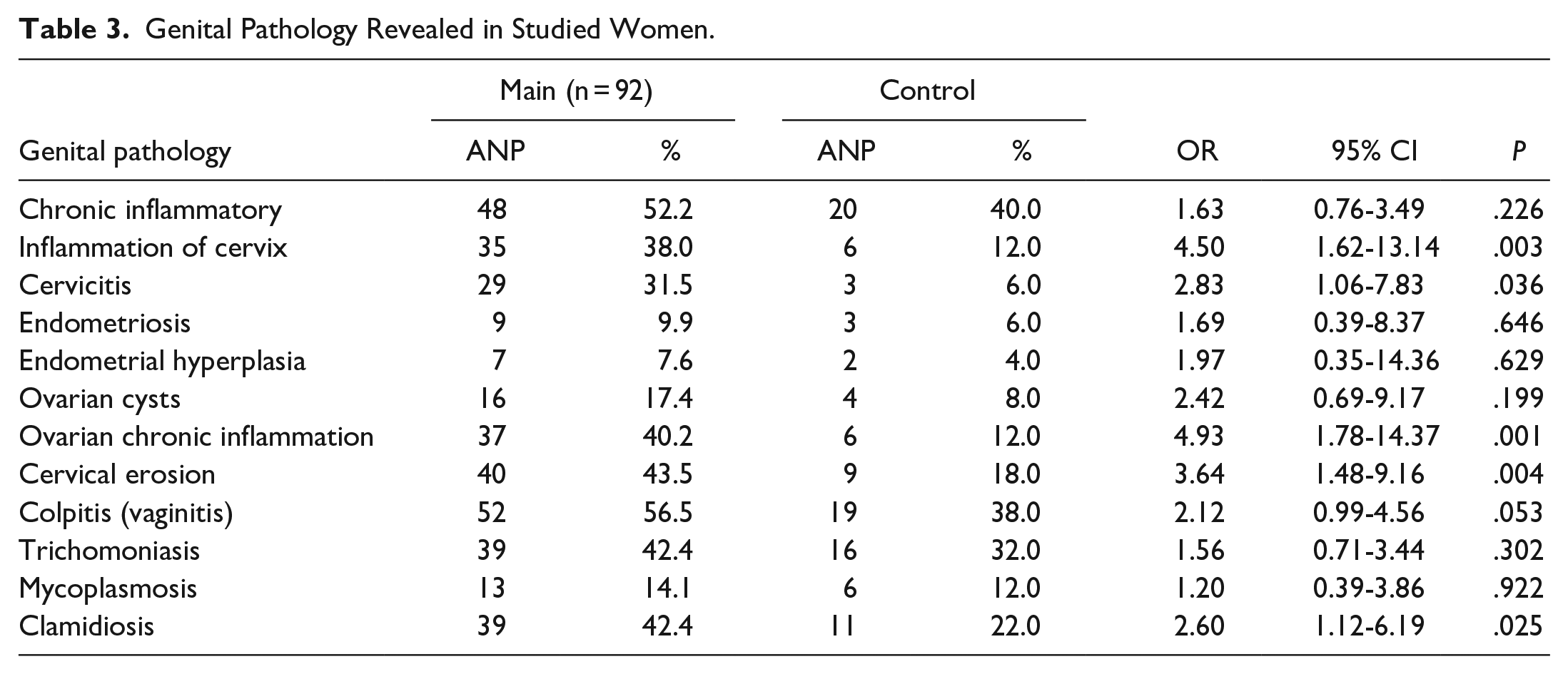
The inflammation of cervix was detected 3 times more in the main group (38%) (OR-4.50, 95% CI −1.62-13.14, P-.003). Cervicitis (31.5%) (OR-2.83, 95% CI −1.06-7.83, P-.036), ovarian chronic inflammation (40.2%) (OR-4.93, 95% CI −1.78-14.37, P-.001) and cervical erosion (43.5%) (OR-3.64, 95% CI −1.48-9.16, P-.004) were represented by high share. According to researches, chronic genital inflammatory processes disturb a pregnant woman’s ability of adaptation, cause metabolic disorders and prolong feto-placental insufficiency. 6
Among parasitic and infectious diseases the attention was focused on high frequency of trichomoniasis (42.4%) and clamidiosis (42.4%). In case of clamidiosis odds ratio was high as well (OR-2.60, 95% CI −1.12-6.19, P-.025). Depending on the literary data, during pregnancy the activation of parasitic and infectious processes is linked to homeostatic changes of the organism and effects fetal organs as well as the systems of vital importance extremely negatively. 12
In case of fetal developmental delay the study of obstetric anamnesis of pregnant women showed that the average indicator of recurrent pregnancy was 2.15 ± 1.75, and the parity 1.49 ± 0.81: in the control group 2.6 ± 1.52 and 1.82 ± 1.11 respectively. Twenty-eight and three tenths percent of the main and 28.0% of control group took hormonal contraceptives. Dysmenorrhea was detected in 46.7% of the main group, whereas this indicator made 16% in the control group.
A number of cases of current complications following the pregnancy (27.2%) and labor (29.4%) were also detected in the anamnesis of pregnant women with fetal developmental delay (in the control group 20% and 16%). As regards the current complications following the pregnancy: in the main group there were surely encountered vomiting during pregnancy (88.0%) (OR-7.97, 95% CI −3.20-20.24, P-.000), risks to miscarriage (loss of fetus) (86.9%) (OR-10.8, 95% CI −4.39-1.84, P-.000), low amniotic fluid (69.6%) (OR-15.7, 95% CI −6.0-42.74, P-.000) and preeclampsia (951.1%) (OR-12.01, 95% CI −3.72-42.92, P-.000). Preeclampsia is the most frequent and greatest cause of forming the placental blood circulation disorder and insufficiency that perform the significant role in formation of fetal developmental delay. As regards low amniotic fluid, according to the data of recent years, oligohydramnios is considered to be one of the earlier diagnostic criterion of fetal developmental delay.13,14
Predictive value was determined for statistically-valid risk identified in the process of research. See Table 4.
The Predictive Value of Maternal Risk Factors.

The risk factors of high predictive value revealed in the process of research were as follows: low standards of living (84%), endocrine pathology (82%), ischemic heart disease (85%), inflammation of cervix (85%), cervicitis 981%), ovarian chronic inflammation (86%), and risks to miscarriage (80%). Preeclampsia (92%) and low amniotic fluid (89%) proved to be of particularly high value.
In conclusion, the complex study of mother’s social-hygienic and medical-biological indicators was conducted in the process of research. There were detected statistically-valid risk factors having a high priority and predictive value, which can be identified in the pre-gravid phase. The considerable importance is attached to timely identification of these factors and introduction of individual measures of managing them so as to minimize their incidence and reduce negative impact on pregnant women and fetus.
Footnotes
Author Contributions
The research is done by Author and it was conducted in Georgian perinatal multiprofile centers.
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.