
Abstract
Background:
Uterine artery doppler velocimetry has proven to be efficient in the prediction of preeclampsia and intrauterine growth restriction. We aimed to determine its value among high-risk Bahamian women and the most predictive parameter.
Methods:
We prospectively observed 128 women to detect the frequency of preeclampsia and intrauterine growth restriction development in relation to uterine artery doppler velocimetry. The main outcome measures were resistance index, pulsatility index and notching.
Results:
The mean difference of 0.082 (±0.011; 95% CI: −0.096, −0.069) in the resistance index and 0.122 (±0.011; 95% CI: −0.144, −0.100) in the pulsatility index between those without preeclampsia and those with, was statistically significant (p < 0.001). The mean RI had a better prognostic value than the mean pulsatility index (OR: 2.623E+51 (95% CI: 2.577E+25, 2.671E+77); p < 0.001. Notching showed a statistically significant with the development of intrauterine growth restriction.
Conclusion:
The best predictor of preeclampsia was the Resistance Index indices, while end diastolic notching was the best predictor for intrauterine growth restriction.
Keywords
Introduction
Preeclampsia is a hypertensive disorder of pregnancy, defined by elevated blood pressure and proteinuria that typically develop after 20 weeks of gestation. While its exact cause remains undefined, it is widely accepted that a failure of placental trophoblasts to properly invade the myometrium leads to inadequate remodeling of the maternal spiral arteries. This results in an increase in placental vascular resistance, a pathology also observed in intrauterine growth restriction (IUGR). 1
Uterine artery doppler velocimetry (UADV) is a noninvasive tool used to measure this vascular resistance, and an abnormal doppler flow is linked to an increased risk for both preeclampsia and IUGR. In normal pregnancies, the diagnostic diastolic notch seen in the first trimester typically disappears by 24 weeks. Its persistence, however, is a strong predictor for future complications. 2
A debate exists, however, about which UADV parameter is the most effective predictor. While notching has a high negative predictive value, its low positive predictive value and concerns about reproducibility have led many researchers to focus on more objective measures of vascular impedance, such as the pulsatility index (PI) and resistance index (RI). 3
This pilot study aimed to determine the value of UADV as a screening tool for preeclampsia and IUGR in a high-risk Bahamian population. We sought to identify the most predictive UADV parameter to assist in developing a departmental screening protocol. By providing population-specific insights into doppler profiles and outcomes in this understudied group, our work contributes to reducing health inequities, enhancing the global understanding of UADV, and improving maternal and fetal outcomes in the Caribbean region and beyond.
Methodology
Setting
The study was conducted in the Commonwealth of the Bahamas at The Princess Margaret Hospital (PMH) in the country’s capital city of New Providence.
Study design
This study design was a cluster sampling. The five major local clinics on the island were identified as the naturally occurring clusters. To ensure a comprehensive and representative sample, all five clinics were selected for participation. The selection order was randomized using Microsoft Excel to document the systematic inclusion of each clinic. Data collection involved spending 1 week at each clinic, where we administered questionnaires to a census of available and consenting patients attending their routine antenatal care appointments. This study commenced in January 2022 and was completed by December 2022.
Study population
Antenatal women with high-risk factors for preeclampsia and intrauterine growth restriction development were included in this study. Participants were between 18 and 24 weeks gestation and of singleton pregnancy with at least one of the following high-risk criteria. They were all enrolled in the Department of Obstetrics and Gynecology at The Princess Margaret Hospital. There was no missing data or loss to follow-up for any participants in this study.
Sampling issues
Selection criteria
Inclusion high-risk criteria
Primigravida, grand multipara
Age > 41
Chronic or gestational hypertension
Pre-gestational or gestational diabetes mellitus
History of preeclampsia
History of partial or complete placental abruption
Antiphospholipid syndrome
Autoimmune diseases
BMI > 25
Exclusion criteria:
Congenital anomalies
Multiple pregnancies
Premature rupture of membranes (PROM)
Preterm labor
Intrauterine fetal demise
Sample size
During the study, it was anticipated that a minimum of 70% of the participants studied using ultrasound doppler of the uterine artery would have had abnormal findings (p = 0.70). The intention was to have a 5% margin of error accompanying this estimate (d: ±0.05). Also the amount of Type 1 error (alpha=) assumed in this estimation process was 5% (i.e., =0.05; hence, z = 1.96 SD). The above information was included in the Chocrane’s Formula for determining the minimum sample size needed when estimating a proportion. 4
A preliminary assessment of the possible number of obstetric patients who would fit the criteria for being successfully selected in this study was likely 409 that would make up this study population number. Hence, further adjusting the minimum sample size corrected for having to be taken from such a finite population revealed that only a minimum of 126 persons was needed for this study.
A questionnaire collecting demographic information and risk factors for adverse pregnancy outcomes was administered to all participants. The questionnaire was pilot-tested on 12 participants, representing 10% of the total study population to ensure clarity and internal consistency.
UADV studies were performed on participants between 18 and 24 weeks’ gestation as part of their routine antenatal care. Gestational ages were confirmed by an early ultrasound scan. All doppler studies were conducted at Princess Margaret Hospital by the same researcher, trained by a consultant radiologist.
Technique
Ultrasound studies were performed using a GE “Voluson P8” machine with a 3.5 MHz curvilinear abdominal transducer. We used real-time pulsed wave color flow to assess the uterine arteries.
For each uterine artery, we obtained three consecutive waveforms to ensure consistency and minimize intraobserver variability. The mean PI and Resistive Index (RI) were calculated from these waveforms, and the presence of end-diastolic notching was noted. We used established cut-offs, a PI above the 95th percentile (>1.58), an RI > 0.58, and the presence of diastolic notching, as a screening tool, similar to methodologies used by Pongrojpaw et al. 5 and Thakur et al. 6
Following the scans, participants underwent routine antenatal check-ups and were followed until delivery. Maternal and neonatal outcomes were collected from their patient files in the labor ward. 3
Prime/outcome variables
The participants were examined for factors which included:
(a) Independent variables (UADVs)
(b) Dependent factors (mean birth weight, mean gestational age, and perinatal parameters and IUGR)
(c) Demographic factors 7
Data analysis
Both descriptive and inferential statistics were used to analyze the collected data with IBM Statistical Package for the Social Sciences (SPSS) (IBM Corp., Armonk, NY, USA).
Descriptive statistics
Appropriate measures of central tendency (percentages, modes, medians, and means) and their accompanying measures of dispersion (full ranges, interquartile ranges, and standard deviations) were calculated for the study’s variables.
Inferential statistics
Inferential statistics were used to analyze the results for statistical significance (p-value criterion: <0.05). Normality was assessed for all continuous variables. As the normality assumption was largely violated, the strengths of association were assessed using Spearman’s rho correlation coefficient (rSp). This nonparametric measure was chosen because it’s more robust and doesn’t require assumptions of normality or linearity, making it appropriate for our data.
Results
Predictors of impaired uteroplacental blood flow
For preeclampsia prediction, the area under the curve (AUC) was 0.934 for PI and 0.932 for RI. Similarly, for IUGR prediction, the AUC was 0.926 for PI and 0.942 for RI. This is shown above in Figures 4 and 5, respectively. These consistently high AUC values, all exceeding 0.92, demonstrate that uterine artery PI and RI possess discriminatory powers in identifying pregnancies at risk for both preeclampsia and IUGR within our high-risk Bahamian cohort. This provides evidence supporting the association between use of these doppler parameters as screening tools in this specific population.
End diastolic notching as a determinant of IUGR and preeclampsia
A statistically significant relationship was found between diastolic notching and both IUGR (Cramer’s V = 0.447, p < 0.001) and preeclampsia (Cramer’s V = 0.814, p < 0.001). Among participants without IUGR (n = 111), 93.7% had normal findings, while among those with IUGR (n = 15), 53.3% had normal findings, 6.7% had unilateral notching, and 40.0% had bilateral notching. Similarly, for patients without preeclampsia (n = 106), no notching was observed. However, among those with preeclampsia (n = 20), 30.0% had normal findings, 20.0% had unilateral notching, and 50.0% had bilateral notching. This is further detailed above in Figure 6.
A multiple logistic regression analysis, using both the RI and PI as predictors, produced a statistically significant model for predicting preeclampsia status (p < 0.05). The model’s predicted probabilities for being preeclamptic ranged from <<0.001 to 0.996, with a median of 0.008 (IQR: <0.001, 0.142). This is shown above in Table 2.
As shown in Table 4 above, the model using combined predictors found the median probability of having an infant with IUGR to be 0.714 (IQR: 0.714, 0.714), with a minimum probability of 0.600 and a maximum of 0.714. The probability of IUGR was consistently tied to the presence of diastolic notching:
No diastolic notching (n = 112): 0.0714
Unilateral notching (n = 4): 0.250
Bilateral notching (n = 10): 0.600
The histogram of this probability distribution was markedly right-skewed and leptokurtic.
Discussion
This prospective observational study was carried out to detect the frequency of the development of pre-eclampsia and IUGR among high-risk pregnant women in the Bahamas, in relation to Uterine Artery doppler velocimetry. In this study, the 126 pregnant participants were followed to delivery using the process that was outlined in Figure 1, and the doppler analysis consisted of demonstrating the presence of RI values, PI values, end-diastolic notching, and MAP. RI reflected blood flow impedance distal to the site of measurement in the microvascular bed. PI reflected the total distal resistance in the vessel and offered data about the cross-section of placental vessels and their placental volume. While end-diastolic notching was typical of vessels with a high resistance and reflected the elasticity of the vessels. Each of these parameters reflects the decidualization of spiral arterioles. 8

Flow chart of sampling process.
To provide a more comprehensive understanding of our cohort’s characteristics and the distribution of key predictive markers, and as recommended by the reviewer, we have included histograms illustrating the distribution of participants’ RI and PI. These visual representations are crucial for assessing data normality, identifying potential outliers, and offering insights into the spread of values within our study population.
Figure 2, depicting the distribution of RI, shows that 82 (65.1%) participants had an RI value of <0.58, while 44 (34.9%) exceeded this established cutoff point for abnormality. This observed proportion of elevated RI values in our high-risk Bahamian cohort is notably higher than what might be expected in a general obstetric population, where the prevalence of abnormal uterine artery doppler findings is typically lower. For instance, studies in broader populations often report a smaller percentage of women exceeding the 95th centile for RI, highlighting the specific characteristics of our high-risk group. 9

Histogram showing the probability distribution of RI among study participants.
Similarly, Figure 3 presents the distribution of PI values. The mean PI of participants was 0.81 (±0.8), with values ranging from a minimum of 0.61 to a maximum of 1.17. Given that the maximum value of 1.17 was notably distant from the majority of the data, the median PI of 0.80 (IQR: 0.75, 0.86) provides a more robust measure of central tendency and the typical spread of PI values among participants. When compared to a previous study involving a large cohort of 7851 pregnancies, where the mean PI was 0.99 and the 95th centile was 1.63, our mean PI appears lower. 10 However, it is important to consider that our pilot study focuses on only a small group of a high-risk population, this may have resulted in a significant proportion of participants with RI values exceeding the 0.58 cutoff, despite a relatively lower mean PI. These distributions visually reinforce the variability in doppler parameters among high-risk pregnancies and underscore the importance of individualized assessment and the development of population-specific reference ranges.
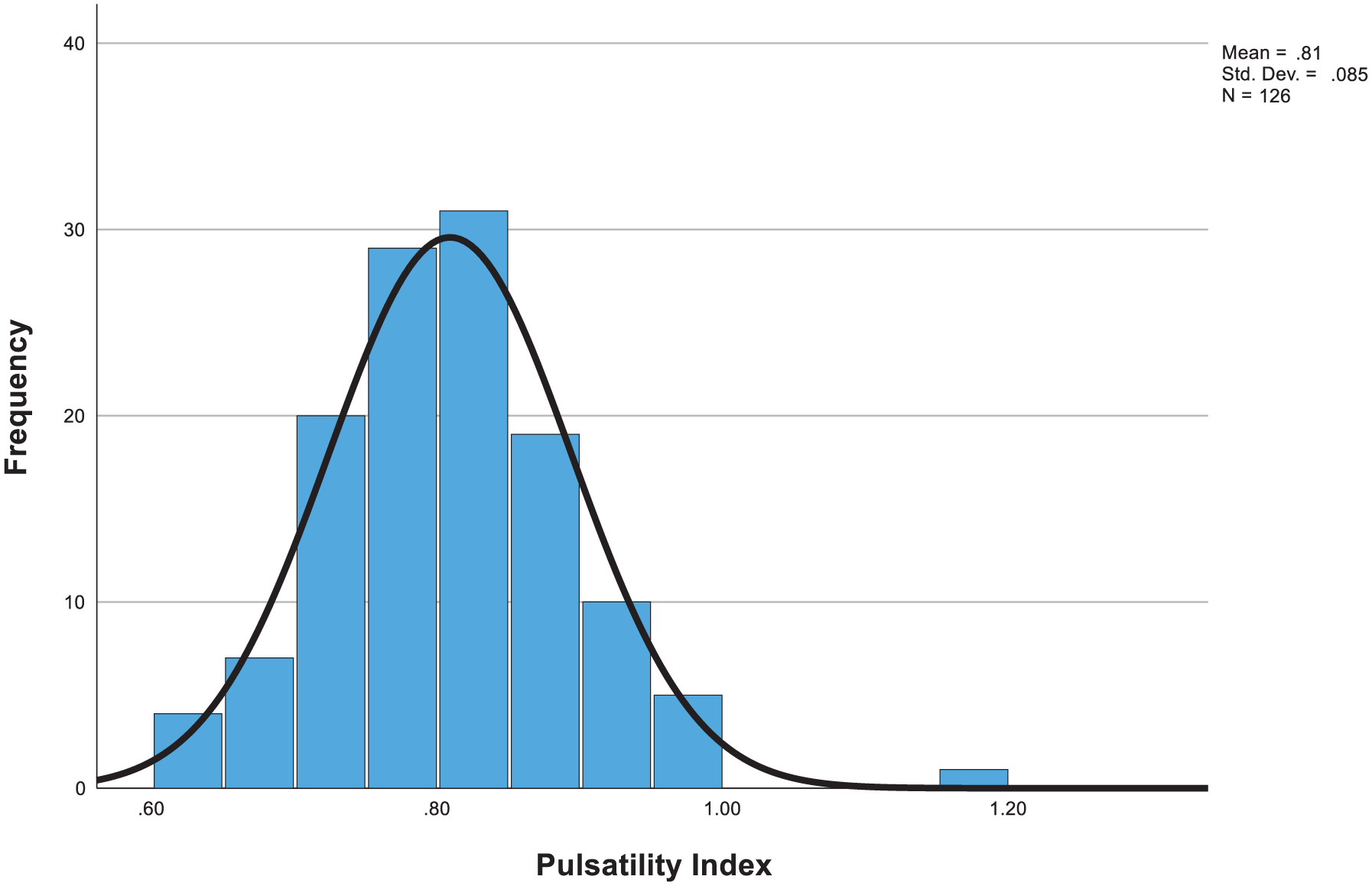
Histogram showing the probability distribution of PI among study participants.
Doppler parameters
Our analysis of predictive performance revealed a strong discriminatory power for both PI and RI in predicting adverse outcomes. The AUC values from the receiver operating characteristic (ROC) curve analysis confirmed the predictive ability of these parameters.
For preeclampsia prediction, the AUC was 0.934 for PI and 0.932 for RI, as shown in Figure 4.
For IUGR prediction, the AUC was 0.926 for PI and 0.942 for RI, as shown in Figure 5.
These consistently high AUC values, all exceeding 0.92, provide evidence suggesting that uterine artery PI and RI may be used as screening tools for identifying pregnancies at risk for both preeclampsia and IUGR within high-risk Bahamian women. 11 This finding coincides with the strong associations we observed in this pilot study and highlights the clinical utility of UADV in this context.
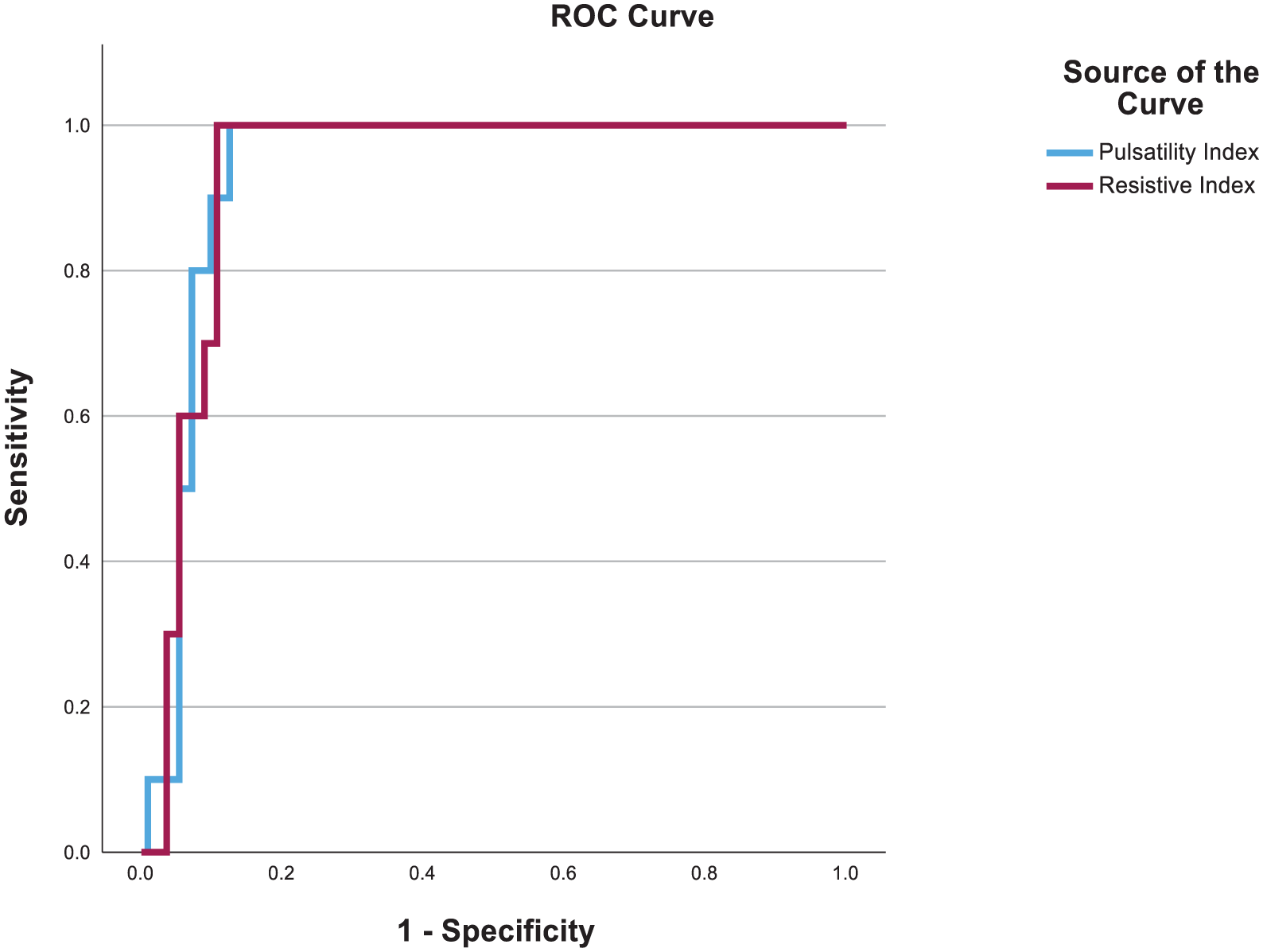
ROC curve analysis to more rigorously evaluate the predictive performance of PI and RI for preeclampsia.

ROC curve analysis to more rigorously evaluate the predictive performance of PI and RI for IUGR.
Predictors of preeclampsia
In our study, an elevation in the RI, PI, and the presence of end-diastolic notching were all strongly associated with the development of preeclampsia. We defined an abnormal UADV as an RI ⩾ 0.58, a PI > 1.58, or the presence of notching (unilateral or bilateral), consistent with established literature.
Resistive Index
The mean difference in RI between participants with and without preeclampsia was 0.082 (±0.011; 95% CI: −0.096, −0.069), which was statistically significant (p < 0.001), as shown in Table 1. This aligns with several studies. Thakur et al. and Mariana et al. both found a strong association between an elevated uterine artery RI and the development of preeclampsia.1,6 Similarly, Yusuf et al. reported that an elevated RI was highly predictive of preeclampsia in high-risk pregnancies. 12 Roberts et al. also found a significant association between uterine artery RI and preeclampsia. 13
Mean resistive index and pulsatility index of participants with preeclampsia verses the participants without preeclampsia, the difference between their means and its statistical significance.

The mean difference of 0.082 (± 0.011; 95% CI: −0.096, −0.069) in the resistive index of the 106 participants with no preeclampsia verses the 20 with preeclampsia was statistically significant (p < 0.001). The mean resistive index for patients without preeclampsia was 0.549 (±0.004), while for those with preeclampsia, it was 0.632 (± 0.005).
The mean difference of 0.122 (± 0.011; 95% CI: −0.144, −0.100) in the pulsatility index of the 106 participants with no preeclampsia verses the 20 with preeclampsia was statistically significant (p < 0.001). The mean pulsatility index for patients without preeclampsia was 0.789 (± 0.008), while for those with preeclampsia, it was 0.911 (± 0.008).
Pulsatility Index
The mean difference in PI between those with and without preeclampsia was 0.122 (±0.011; 95% CI: −0.144, −0.100), which was also statistically significant (p < 0.001), also shown in Table 1. These results align with a number of studies, including those by Khong et al., 2 Reddy et al., 14 and Mallikarjunappa et al., 15 which similarly found an elevated PI to be a good predictor of preeclampsia. The predictive value of PI is further supported by the work of Dal et al., 16 who reported a 66.6% positive predictive value and 61.9% sensitivity for preeclampsia screening. Additionally, in their high-risk Nigerian cohort, Roberts et al. 13 observed that PI significantly and correctly predicted 86% of preeclampsia cases.
End-diastolic notching
End-diastolic notching showed a moderately positive relationship with the development of preeclampsia (Cramer’s V = 0.814, p < 0.001). While none of the participants without preeclampsia (n = 106) showed notching, among the 20 with preeclampsia, 30.0% showed no notching, 20.0% had unilateral notching, and 50.0% had bilateral notching, as shown in Figure 6. This strong association is supported by multiple studies. Mariana et al. 1 reported a high rate of preeclampsia (100.0%) in patients with bilateral notching. Yusuf et al., 12 Coleman et al., 3 and Oancea et al. 8 also found a significantly higher prevalence of notching in participants who developed preeclampsia.

Bar chart depicting the effect of unilateral and bilateral end-diastolic notching on IUGR and preeclampsia.
Prognostic value of predictors
In our multiple logistic regression analysis, mean RI was found to have a stronger prognostic value for preeclampsia than mean PI (OR: 2.623E+51 (95% CI: 2.577E+25, 2.671E+77); p < 0.001), as shown in Table 2. This finding is consistent with research by Thakur et al., 6 Kurdi et al., 17 and Albaiges et al., 18 who also reported that mean RI performed better than other doppler indices in the prediction of preeclampsia.
Multiple logistic regression analysis regarding significant predictors (RI and PI) of participants preeclampsia status in this study.

Predictors of IUGR
In our study, we found a strong association between elevated second-trimester UADV and the development of IUGR. The mean difference in RI was 0.034 (±0.014; 95% CI: −0.062, −0.006) between those with and without IUGR, which was statistically significant (p = 0.018). While the mean difference in PI was 0.047 (±0.023; 95% CI: −0.001, −0.0.093), this was also a statistically significant difference (p = 0.045), as shown in Table 3. These findings are consistent with existing literature, as studies by Razavi et al., 19 Papageorghiou et al., 20 and Asafi et al. 21 have all shown a connection between abnormal doppler indices (RI and PI) and IUGR.
Mean resistive index and pulsatility index of participants with IUGR verses the participants without IUGR, the difference between their means and its statistical significance.

Mean Resistive Index: The mean difference of 0.034 (± 0.014; 95% CI: −0.062, −0.006) in the resistive index of the 111 participants with no IUGR verses the 15 with IUGR was statistically significant (p = 0.018). The mean resistive index for patients without IUGR was 0.558 (±0.005), while for those with IUGR it was 0.593 (±0.011).
Mean Pulsatility Index: The mean difference of 0.047 (±0.023; 95% CI: −0.001, −0.093) in the pulsatility index of the 111 participants with no IUGR verses the 15 with IUGR was statistically significant (p = 0.045). The mean pulsatility index for patients without IUGR was 0.803 (±0.008), while for those with IUGR, it was 0.850 (±0.017).
RI: resistance index; PI: pulsatility index; IUGR: intrauterine growth restriction.
We also found a statistically significant relationship between end-diastolic notching and the development of IUGR (Cramer’s V = 0.447, p < 0.001). The prevalence of notching was notably higher in the IUGR group. Of the 111 participants without IUGR, 93% had normal findings, while 2.7% and 3.6% showed unilateral and bilateral notching, respectively. In contrast, among the 15 participants with IUGR, only 8% had normal findings, with 6% showing unilateral notching and 40% showing bilateral notching. This is comparable to the findings of Mariana et al., who reported that 40% of patients with bilateral notching developed IUGR. 1
In our multivariable logistic regression analysis, end-diastolic notching was a better predictor of IUGR than either mean RI or mean PI, as shown in Table 4. Specifically, bilateral notching was the most predictive parameter (OR: 19.500; 95% CI: 4.550, 83.568; p < 0.001). Furthermore, the mean gestational weight of infants differed statistically significantly by 1.60 (±0.28) lbs. between those with normal versus bilateral notching (p < 0.001). These results align with a study by Khong et al., which also found that bilateral notching was a better prognostic indicator of IUGR than other doppler parameters. 2
Multiple logistic regression analysis regarding significant predictors (End-Diastolic Notching), of participants’ infants’ IUGR status in this study.

RI: resistance index; PI: pulsatility index; IUGR: intrauterine growth restriction.
Limitations
This study has several limitations, primarily stemming from its small sample size and pilot nature. The sample, consisting exclusively of women from a single center in the Bahamas, limits the direct generalizability of our findings. This single-center design, combined with population-specific factors like a unique genetic background, environmental influences, and healthcare system structure, restricts the applicability of our results to other, more diverse populations.
A second limitation is the inherent subjectivity of notching assessment and the lack of a universally accepted definition. While we followed a standardized protocol, this definitional variability in the literature can impact the generalizability of our notching-related findings. Additionally, our use of a >95th percentile cutoff for the RI and PI, although based on clinically established thresholds, may have reduced statistical power. A continuous modeling approach would provide a more granular and statistically powerful assessment, and we acknowledge that this as a limitation of the pilot phase.
Third, the high AUC values we observed (e.g., 0.934 for PI and 0.932 for RI) are notably higher than those reported in some meta-analyses. 22 This is likely a statistical artifact of our small sample size rather than an indication of superior predictive accuracy in the Bahamian context. The same is true for the extremely large odds ratio for RI predicting preeclampsia, which resulted in an unstable model and a confidence interval spanning 52 orders of magnitude. This phenomenon is a known statistical artifact in logistic regression with small sample sizes and limited events.
Finally, standard guidance for robust logistic regression recommends at least 10 events per variable. 23 Our study’s event count falls below this threshold, which may have led to less stable and potentially biased coefficient estimates.
Strengths
Despite its limitations, our study has several key strengths. First, we focused on a high-risk population already predisposed to preeclampsia, making our findings particularly relevant to this group. This is a unique approach compared to many studies that include low-risk women.
Additionally, this study addresses a crucial gap in the literature by focusing on a previously unstudied Bahamian cohort. This population-specific research is essential for providing foundational data on UADV within this demographic. The findings can be used as a basis for further, larger-scale research and have potential applicability to neighboring Caribbean nations facing similar maternal health challenges.
Third, a strength is the demonstration of the feasibility and methodology of our research design. Our work proves that the protocol for UADV screening and data collection is practical and can be successfully implemented in a clinical setting with limited resources. This provides preliminary data and a proof of concept that can be used to justify and design a larger, more definitive study.
Furthermore, all doppler scans were performed by a single investigator using the same machine and standardized settings. The investigator was trained and approved by a consultant radiologist, which ensures the accuracy and internal validity of our results by minimizing intraobserver variability.
Conclusion
Our study assessed the frequency of preeclampsia and IUGR in relation to UADV findings in high-risk Bahamian women between 18 and 24 weeks’ gestation. Our findings on the predictive value of uterine artery PI and RI align with recent longitudinal studies, like that of Cavoretto et al., 24 which established contemporary reference ranges for these parameters. This confirms the relevance of our findings within a broader global context of doppler research. We found that a combination of RI and PI provides the best prediction for preeclampsia, supporting the use of these objective measures over the more subjective assessment of notching.
Recognizing the limitations of our small pilot sample, we can plan subsequent, larger-scale investigations. These studies will feature a significantly larger sample size, enabling more stable statistical modeling and providing more biologically plausible odds ratios and narrower confidence intervals.
Clinical implications
The ability to predict preeclampsia and IUGR is critical for providing targeted care. Uterine artery doppler velocimetry can be clinically used to stratify high-risk pregnant women, allowing for the prophylactic administration of low-dose aspirin and more focused surveillance for those at increased risk. This tool could be particularly valuable in resource-limited settings like the Bahamas.
Supplemental Material
sj-docx-1-smo-10.1177_20503121251378109 – Supplemental material for Role of second trimester uterine artery doppler in early prediction of preeclampsia and intrauterine growth restriction among high-risk Bahamian residents
Supplemental material, sj-docx-1-smo-10.1177_20503121251378109 for Role of second trimester uterine artery doppler in early prediction of preeclampsia and intrauterine growth restriction among high-risk Bahamian residents by Azaria Clare and Vrunda Sakharkar in SAGE Open Medicine
Footnotes
Acknowledgements
We would like to thank Dr. Morton A. Frankson (The University of The West Indies School of Clinical Medicine and Research, Nassau, The Bahamas) for his epidemiological support in this research.
Ethical considerations
The study was approved by The Public Hospital Authority/University of The West Indies Research Ethics Committee Ethics Committee via the Research Application Identifier Number MROS/539311/QQC/APPROVED dated 28 January 2022.
Consent to participate
Informed consent to participate was written and voluntary.
Author contributions
VS conceived the study. AC developed protocol, gained ethical approval, recruited patients, collected and analyzed data, and wrote the first draft of the manuscript. All authors researched literature, reviewed and edited the manuscript. VS approved the final version.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
10.6084/m9.figshare.28046063
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.