
Abstract
Purpose. To investigate factors associated with immunization incompletion of children under 5 years in Ebonyi state, Southeastern part of Nigeria. Method. A cross-sectional and a cluster sampling design were implemented; 400 women of childbearing age in families with children between 0 to 59 months of age were interviewed in Ebonyi state. Demographic characteristics of the child and mother, the child’s immunization history, and reasons for partial immunization were obtained with the use of a self-administered questionnaire. Data were analyzed using descriptive statistics of mean, standard deviation, t-test and ANOVA with SPSS version 23 and hypothesis tested at P < .05. Results. Findings revealed that 180 (48.1%) females, and 194 (51.9%) males’ children were immunized; Less than half 155 (41.9%) of the children had 1 missed dose, considered as partial immunization cases indicating low coverage. Of the reasons given for incomplete immunization mothers, mothers agreed that immunization centers are far from home (x̄ = 2.55 ± 0.92). This reason significantly affects mothers who were young (≤20 years) (x = 2.86 ± 0.94; P = .018), single (x = 2.84 ± 1.05; 0.037), had secondary education (x = 2.65 ± 1.08;0.000), students (2.89 ± 1.08; P = .000), poor (x = 2.63 ± 1.05; P = .009), and primiparous (x = 2.50 ± 1.08; P = .036) are more affected and they agreed (grand mean >2.50). Conclusion. Immunization coverage was low, and far location from health facility was indicted thus policy implementers should locate health facilities close to homes. also health education on the importance of immunization should be given to mothers especially those who are young and has low socio-economic status.
Keywords
What do we already know about this topic?
There is low immunization in Nigeria.
How does your research contribute to the field?
This article investigated the routine immunization of children under 5 years in Ebonyi state, Southeast Nigeria using a cross-sectional study, and findings agreed with the report of the National Demographic Health Survey. Reasons given for incomplete immunization were long waiting time, far distance, attitudes of health workers, inconvenient schedules of immunization, and beliefs.
What are your research’s implications toward theory, practice, or policy?
Efforts to increase accessibility, reduction in waiting time, sensitization on the need for antenatal and hospital delivery, girl-child education, and family planning should be enhanced by policy makers and relevant agencies.
Introduction
More than 2.7 million children die annually, even when existing immunization would have prevented 2 to 3 million deaths. 1 The under-5 mortality is caused by malaria, pneumonia, diarrhea, and other vaccine-preventable diseases like pertussis, measles, and meningitis,2,3 and one of the utmost public health challenges today is suboptimal vaccine uptake rates. Moreover, the reduction of under-5 mortality rate in Nigeria is important because among the lower-middle-income country (LMC) in West Africa she has the highest under-5 child mortality rate (U5MR) with 714 000 deaths occurring every year, and that accounts for 13% U5MR globally. 2 Immunization is the first line of action against vaccine-preventable diseases and one of the most effective health benefits available to children for reducing under-5 mortalities.4,5 In Nigeria, vaccine-preventable diseases (VPD) are known to account for 22% of childhood death amounting to over 200 000 children per annum.6-8 About 87% of post-neonatal mortality can be tackled by addressing malaria, pneumonia, and diarrhea and improving immunization. The incidence of disabilities, including mental retardation, hearing loss or deafness, meningitis, intellectual disability as well as mobility impairment, has been greatly reduced by immunization against polio as well as rubella, meningitis, measles, diarrhea and pneumonia. 2 To guarantee children full protection against vaccine-preventable diseases, caregivers (mothers) need to be mandated to taking the provided vaccines at the right time. According to CDC children before the age of 2 years should be fully immunized against 14 potentially deadly diseases which include polio, rubella, hepatitis, measles, yellow fever, tuberculosis, pertussis tetanus, and rotavirus among others. 9 Also, WHO planned a 9-month vaccine plan for infants at their priming age of life such as Bacilli Calmette Guerin (BCG), Oral Polio Vaccine (OPV), Hepatitis B vaccine (HBV), Hemophilus Influenza B vaccine, Diphtheria, Pertussis and Tetanus (DPT), inactivated polio vaccine (IPV) Measles vaccine and Yellow fever vaccine.10,11 The underlying goal of the immunization schedule is to achieve effective, lasting immunity against vaccine-preventable diseases. 12
Currently, it is recommended that all children when born should be vaccinated with the appropriate vaccine. At birth they should be given Bacille Calmette–Guerin (BCG, OPV0, and Hep B0, at 6th weeks-Pentavalent 1 (DPT1, Hep B, and Hib), PCV1, OPV1 and Rota1, at 10 weeks-Pentavalent 2 (DPT, Hep B, and Hib), PCV2, OPV2 and Rota 2. At 14 weeks- Pentavalent 3 (DPT, Hep B and Hib), PCV3, OPV3, and IPV. At 6 months the children should receive Vitamin A 1st dose. In the 9th month, each surviving child should be given 1st dose measles, yellow fever, and meningitis vaccines. At age 15 to 23 months a child should be vaccinated with measles second dose.13,14 Therefore, a fully immunized child must have had the above.4,15
The estimated global vaccination coverage in 2018 according to the World Health Organization, were: Bacilli Calmette Guerin (BCG)-47%, 3 doses of Oral Polio Vaccine (OPV)-85%, Hepatitis B vaccine (HBV)-84%, 3 doses of Hemophilus Influenza B (Hib) vaccine-22%, 3 doses of Diphtheria, Pertussis, and Tetanus (DTP3) vaccine-86%, 1 dose of Measles vaccine-86%, 2 doses of measles vaccine-69%, Rotavirus vaccine-35%, and Yellow fever vaccine-49%.16-18 Immunization programs have become more difficult over the past years’ due principles and factors of consideration in introduction, and availability of new vaccines, 19 and setting up of desired worldwide target for disease control such as polio eradication and measles elimination. 10 Polio which is targeted for worldwide eradication has stopped in all nations except for Pakistan, Afghanistan, and Nigeria. All the countries, especially those experiencing conflict and instability remain at risk until polio is fully eradicated. 17 However, Since August 2016 Nigeria has not recorded any case of wild polio and is on the point of polio eradication; this success rests on highly granular monitoring and evaluation (M&E), the deployment of digital technology, and reaching the most isolated communities. 2
Though the country has recently made some progress in immunization rates with current coverage at 50.1% which is low. 2 To address this crisis, numerous approaches were deployed to boost immunization in Nigeria but these interventions still encounter challenges. 20 The Federal Government of Nigeria (FGoN) has committed itself to improve its human capital to reduce under-5 mortality by half by 2030. The proposed Multiphase Programmatic Approach (MPA) includes Improving utilization and quality of immunization which is the Intermediate Program Outcome (Phase I) among others. 2 Despite the awareness and struggle in immunization program the immunization coverage of children still lags. Children who are not immunized most time are likely to come from families of low socioeconomic status.21,22 To prioritize immunization, parents are supposed to perceive immunization as one of the safest and most effective interventions to prevent morbidity and early child mortality. Contrary to this, due to much engagement, customs, and tradition, they missed many opportunities which in turn lead to childhood mortality. In the country for instance, vaccines are made available to the public freely, yet over 20% of Nigerian children are not fully immunized each year. 16
This study, therefore, investigated the factors affecting the routine immunization utilization of children under 5 in Ebonyi state, Nigeria.
Materials and Methods
Study Design
This study adopted a population-based cross-sectional survey. According to Abonyi et al, 23 a descriptive survey consists of study in which data are collected collected from a small sample of a large population that enables the researcher to describe systematically and interpret the characteristic features and facts about things that exist.
Study Setting
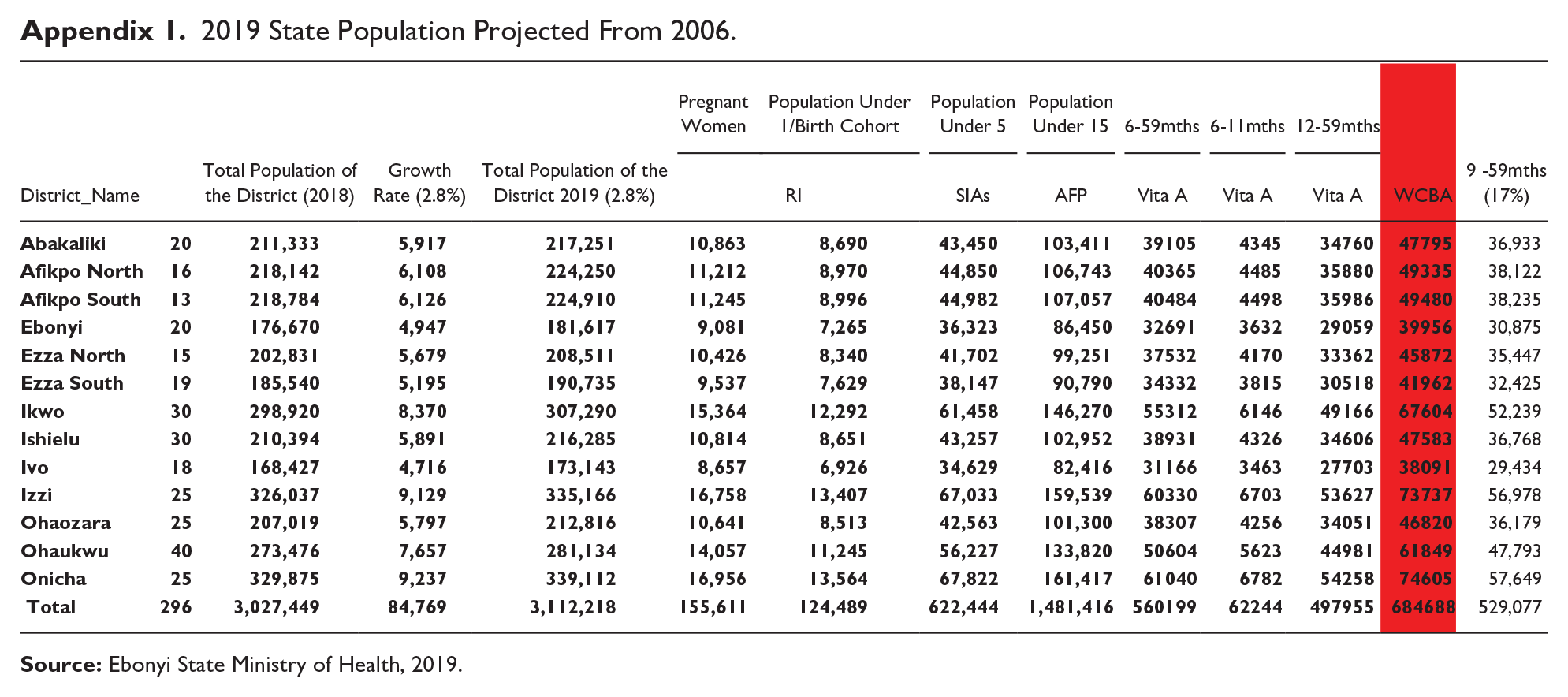
The study was conducted in 6 LGAs in Ebonyi state which has 13 Local Government Areas and 156 autonomous communities. Ebonyi state occupies a land area of 5,954 square kilometers and situated between longitude 70 and 80 301 E and latitude 50 401 and 60 541 north of the equator. The state is part of the southeast geopolitical zone and bounded in the north by Benue state, in the west by Enugu state, in the east by Cross River State and in the south by Abia state. The population of Ebonyi state for 2019 is 3 027 449 (projected from 2006 census of 2 173 501 with a projected growth rate of 2.8%). The population of children under 5 years was 622 444 (20.56%), pregnant women 155 611 (5.14%) and women of childbearing age 684 688 (22.62%). 24 see Appendix 1
Study Population
For this study, the population comprised of 684688 women of childbearing age in Ebonyi state projected from the 2006 census of 2,173,501 with a projected growth rate of 2.8% for the year 2019. 24
Sample and Sampling Technique
The sample size of the study consisted of 400 women of childbearing age which was determined using Taro Yamen formula used by Uzoagulu.
25
Ebonyi state was divided into 3 senatorial zones namely: Ebonyi north, central, and south zones. 6 out 13 LGAs were purposively selected, 3 rural and 3 Urban. The respondents were recruited purposively from the households that have women of childbearing age with under 5 children ensuring that there was proportional representation in the villages (there were
Data Collection Instrument
The instrument for data collection was self- administered questionnaire consisted of 3sections; section A on child’s demography (Age, Sex, Birth order, place of birth and immunization Status); B on mother demography (Age, parity, marital status, occupation, no of antenatal visit, level of Education, location and number of children living in the household); C, 7 items on factors using a 4-point Likert scale of strongly agreed (SA), agreed (A), disagree (D), strongly disagree (SD). Three experts’ facilitators from the Department of Public Health established the face validity of the instrument. This ensured clarity of instructions; proper wording of items, appropriateness, and adequacy of the items in addressing the objectives of the study. The reliability of the instrument was established using data collected from 20 Women of Child-Bearing Age not included in the study sample. The process yielded an overall reliability of the coefficient of 0.934 which is reliable for use in this study. Five research assistants interpreted the questions in the local language to the non-literate’s mothers.
Data Analysis
In this study, fully immunized children are children who were immunized based on WHO classification. Childs’ immunization cards were used to ascertain their immunization status. Of 400 copies distributed 374 representing 94% return rate were used for data analysis. Thereafter, data were analyzed using mean (x) score, standard deviation, t-test and Analysis of Variance (ANOVA). Mean score was used to answer all the research questions. The criterion mean (x) of 2.50 was set for the study. A criterion mean was derived by adding up the scale values and dividing the sum by the number of scale options thus: 4 + 3 + 2 + 1 = 10/4 + 2.50. Uzoagulu 25 criterion mean adopted from Likert’s scaling was applied to categorize the different constructs being studied for description. A criterion means of 2.50 and above was “agreed” and below 2.50 was considered “disagreed.” On the other hand, t-test and ANOVA were used to test hypotheses at 0.05 level of significance.
Results
Result revealed that majority of children whose mothers participated in the study were 2 years 98(26.1%) and ≤1year 82(21.9%), females 180(40.1%), in Birth order [1-2] 273(73.0%), fully immunized 219(58.6%), born in the home of TBAs 105(28.1%) and their mothers had antenatal visits of 4 and above 181(48.4%). Also out of 374 mothers’ respondents, the majority were 21-30 years of age 232(62.0%), married 291(77.8%), rural dwellers 353(94.4%), had secondary education 155(41.4%), self-employed 221(59.1%), wealth of middle class 229(61.2%), multi-parous 224(59.9%) and had 3-4 number of children living in their household 159(42.5%) Table 1.
Socio-Demographic Characteristics of Respondents (Mothers) and Children (n = 374).

Factors investigated were: health workers’ behavior, experience with past immunization, location, beliefs, schedules, time and vaccine unavailability. In result of Table 2, A majority of the mothers 205(54.8%) disagreed to health worker’s negative behavior (x̄ = 2.11 ± 0.86); 169(45.2%) agreed that immunization was effective (x̄ = 2.11 ± 0.86); 123(32.9%) agreed that immunization centers were far from home (x̄ = 2.44 ± 1.02); 184(49.2%) disagreed to no belief in immunization; 246(65.8%) disagreed that there was inconvenient immunization schedule (x̄ = 2.00 ± 0.68); 174(46.5%) disagreed to long time spent during immunization (x̄ = 2.35 ± 0.99); and 180(48.1%) disagreed to unavailability of respondents (x̄ = 1.82 ± 0.81). It was reported that a mean score of ≥2.50 was agreed and <2.50 as disagreed. Thus, mothers have a positive attitude toward immunization and agreed that immunization was effective (Table 2).
Frequency and Percentage of Mothers Responses to Each Likert Scale on the Factors Affecting Routine Immunization Utilization.

Abbreviations: SA, Strongly Agree; A, Agree; D, Disagree; SD, Strongly Disagree.
Fifty-eight point 6% (58.6%) of children of the sampled mothers were fully immunized while 41.4% were partially immunized. Mothers of children who were fully immunized only agreed that past immunization were effective (x̄ = 2.82 ± 0.93). While they strongly disagreed to other factors which were: negative health workers’ behavior (x̄ = 1.94 ± 0.73), vaccination centers far from home (x̄ = 2.36 ± 1.08), no belief in immunization (x̄ = 1.59 ± 0.61), inconvenient immunization schedule (x̄ = 1.94 ± 0.63), long time spent during immunization (x̄ = 2.26 ± 1.02), and unavailability of vaccine (x̄ = 1.69 ± 0.69). Also, mothers whose children were partially immunized agreed that immunization was effective (x̄ = 2.78 ± 1.02) immunization center was far from home (x̄ = 2.55 ± 0.93) and time spent during immunization was long (x̄ = 2.55 ± 0.92). Also they strongly disagree to unavailability of vaccine (x̄ = 1.75 ± 0.79) and slightly disagreed that health workers’ behavior were negative (x̄ = 2.34 ± 0.97), no belief in immunization (x̄ = 2.14 ± 0.95) and inconvenient immunization schedule (x̄=2.08 ± 0.75). Thus factors that mostly contributed to mothers’ negative attitude to routine immunization were: immunization center being far from home. Table 3.
Mean and Standard Deviation Scores on Mothers Responses Based on the Immunization Status of the Child.

Abbreviations: Dec, Decision; Std dev, standard deviation.
The independent variables are the socio-demographics while mother’s responses (attitudes in mean score) is dependent. Overall, mothers disagreed to negative health workers’ behavior (grand mean = 2.11 ± 0.86). This disagreement was more among older mothers >40 years (2.00 ± 0.00), those who delivered at private hospital (1.85 ± 0.79) (P = .002), those who had up to 4 antenatal visit (1.96 ± 0.77), birth order [1-2] (2.04 ± 0.083), (P = .014) widowed (2.00 ± 1.02), urban residents (2.10 ± 1.04), those with secondary education (1.94 ± 0.70), civil servants (1.92 ± 0.56), the rich (2.03 ± 0.93), primiparous (1.88 ± 0.76) (P = .002*), and those with less number of children (1.99 ± 0.75). however, only place of delivery, birth order, and parity were significant (P < .05). [Table 4].
Summary of Analysis of Variance and Independent Sample t Test on Mother’s Responses on Health Workers’ Behavior Based on the Socio Demographic Characteristics.

Abbreviations: Dec, Decision; S, Significant; NS, Not Significant.
Overall, mothers agreed that past immunization was effective (grand mean = 2.82 ± 0.98). this agreement was more among mothers of older age (3.00 ± 1.41), those who delivered at public hospital (2.98 ± 1.03), had up to 4 antenatal visits (2.86 ± 1.01), child’s birth order [3-4] (2.88 ± 1.09), singles (2.91 ± 0.59), rural residents (2.84 ± 0.97), those with secondary education (2.90 ± 0.82) (P = .020*) civil servants (3.08 ± 1.29), the middle class (2.87 ± 1.02), multiparous (2.90 ± 0.93), and those with the least number of children [1-2] (2.90 ± 0.85). However, only level of education was significant (P < .05) with this response (Table 5).
Summary of Analysis of Variance and Independent Sample t Test on Mothers Responses on Experience with Past Immunization Based on the Socio Demographic Characteristics.

Abbreviations: Dec, Decision; S, Significant; NS, Not Significant.
Table 6 showed that on geographic factors, mothers generally disagreed that vaccination centers were far from home (grand mean = 2.44 ± 1.02). This response was more among mothers who were middle age (2.31 ± 0.90), (P = .018*), those that delivered at a public hospital (2.29 ± 1.03), those with no antenatal visit (2.33 ± 2.00), the widowed (2.08 ± 1.09), (P = .037*), urban residents (2.24 ± 1.03), those with tertiary education (1.85 ± 0.92), (P = .000), civil servants (2.08 ± 0.93, (P = .000*), the rich (2.03 ± 1.00), (P = .009*), grand multiparous (2.15 ± 0.93 (P = .036*), and those with more than 6 number of children (2.07 ± 1.00). Age, marital status, level of education, occupation, wealth index, and parity were significant (P < .05) (Table 6).
Summary of Analysis of Variance and Independent Sample t Test on Mothers Responses on Location [Vaccination Centers Being Far From Home] Based on the Socio Demographic Characteristics.

Abbreviations: Dec, Decision; S, Significant; NS, Not Significant.
Table 7 showed that on beliefs, overall, majority of the mothers strongly disagreed to no belief in immunization (grand mean = 1.82 ± 0.81). Their responses with regard to the socio demographic characteristics of the respondents showed that those who had the highest disagreement were the middle age mothers (1.80 ± 0.89), delivered in a public hospital (1.58 ± 0.65) (P = .000*) mothers who had 1 to 3 antenatal visits. (1.61 ± 0.65) P = .000*), birth order 3 to 4 (1.79 ± 0.93), widowed (1.73 ± 0.78), urban dwellers (1.81 ± 0.98), had tertiary education (0.46 ± 0.81) P = .002*, civil servants (x = 1.46 ± 0.81), P = .002*, the rich (x = 1.37 ± .66), P = .003*, primiparous (x = 1.77 ± 0.73), and those who had 3-4 number of children in the household (x = 1.77 ± 0.79). place of birth, level of education, occupation, and wealth index were significant with this response.
Summary of Analysis of Variance and Independent Sample t Test on Mothers Responses on Beliefs, Based on the Socio Demographic Characteristics.

Abbreviations: Dec, Decision; S, Significant; NS, Not Significant.
Table 8 revealed that on geographic factors, majority mothers disagreed to inconvenient immunization schedules no belief in immunization (grand mean = 2.00 ± 0.68). Their responses with regard to the socio demographic characteristics of the respondents showed that those who had the highest disagreement were middle age mothers who were 31 to 40 years (1.91 ± 0.56), delivered in public hospital (1.85 ± 0.73) (P = .007*), mothers who had ≥4 antenatal visits, (1.90 ± 0.62) (P = .004*), child’s birth order >6 (1.60 ± 0.89), widowed (1.88 ± 0.59), rural dwellers (2.00 ± 0.67), those that have tertiary education (1.61 ± 0.65) (P = .000*), civil servants (x = 1.85 ± 0.78), the rich (2.00 ± 0.80), (P = .040), grand multi-parous (1.90 ± 0.63), and those who had 5 to 6 number of children in the household (1.88 ± 0.61), (P = .044*).
Summary of Analysis of Variance and Independent Sample t Test on Mothers Responses on Schedules Arrangement, Based on the Socio Demographic Characteristics.

Abbreviations: Dec, Decision; S, Significant; NS, Not Significant.
Table 9 showed that, on time spent during immunization, the majority of mothers disagreed on a long time spent during immunization (x = 2.34 ± 0.99). this response was significant with older mothers >40 years (1.75 ± 0.50) (P = .000), the divorced (2.04 ± 0.84), (P = .001*), those with tertiary education, (1.76 ± 0.67), civil servants (1.73 ± 0.53), (0.010*) and the rich (1.91 ± 1.00), (P = .000)
Summary of Analysis of Variance and Independent Sample t Test on Mothers Responses on Long Time Spent During Immunization, Based on the Socio Demographic Characteristics.

Abbreviations: Dec, Decision; S, Significant; NS, Not Significant.
In Table 10, it was shown that majority mothers disagreed strongly to unavailability of vaccine (x = 1.72 ± 0.73). This disagreement is significant with birth order [1-2] (1.71 ± 0.016), those with tertiary education, (1.52 ± 0.72), (0.049) civil servants (1.42 ± 0.70) (P = .000*), middle class (1.61 ± 0.71) (0.000*), and those with up to 5 number of children (1.53 ± 0.66), (P = .035*).
Summary of Analysis of Variance and Independent Sample t Test on Mothers Responses on Vaccine Unavailability, Based on the Socio Demographic Characteristics.

Abbreviations: Dec, Decision; S, Significant; NS, Not Significant.
Discussion
Immunization Status of the Children
The result of the study showed that 219(58.6%) of children were fully immunized showing low coverage which is in line with the findings of Etana and Deressa,
13
Noh et al,
21
Al-lela et al,
26
Akwataghibe et al,
27
Factors Affecting the Routine Immunization Utilization
Factors investigated were: behavior, experience with past immunization, location, Beliefs, schedules, time and vaccine unavailability
Health workers’ behavior
In this study respondents disagree that health workers’ behavior were negative (grand mean = 2.11 ± 0.86), though those whose children were partially immunized were more likely to agree (x = 2.34 ± 0.97) than the fully immunized (x = 1.94 ± 0.73), hence negative health workers are more likely to affect those whose children had partial immunization. With respect to the socio-demographic characteristics, mothers of children of birth order 5 to -6, (x = 2.62 ± 0.97), delivered at Home of TBA (x = 2.32 ± 0.89), having no antenatal visit (x = 2.31 ± 1.01), having no formal education (2.31 ± 0.99), Grand multiparous (x = 2.37 ± 0.99) and having ≥6 number of children living in the household (x = 2.67 ± 1.14) were significantly associated with complain of negative health workers’ behavior (P = .014, .002, .003, .002, .002, .000) respectively. This finding aligns with the other findings of Akwataghbe et al 27 whose respondents reported health workers’ behavior as “helpful” or “very helpful” while Al-lela et al 26 and Rahji and Ndikom 31 who found that health workers’ attitude, is a factor hindering compliance with immunization schedules.
Experience with Past Immunization
The majority of the mothers agreed that past immunization of their children was effective (grand mean = (x = 2.82 ± 0.98). Both the mothers of fully and partially immunized children strongly agreed that past immunization was effective (x = 2.80 ± 0.93; 2.78 ± 1.02). This showed that experience with past immunization had no negative influence on routine immunization utilization of children. This report is significantly associated with the level of education among those who have secondary education (x = 2.90 ± 0.82, P = .020). Contrastingly, Akwataghibe et al 27 reported that AEFI promoted fear among young mothers and, thereby discouraging initial use of immunization.
Location of Health Facility
The respondents whose children were partially immunized agreed that vaccination centers were far from home (x = 2.55 ± 0.93) while those who had their children fully immunized reported otherwise (x = 2.36 ± 1.08). This finding revealed that the location of vaccination centers can influence the routine immunization of children. It will have a negative influence when it is far from mothers and not easily assessable but will influence it positively when situated close to their homes. However, mothers who were young (≤20 years) (x = 2.86 ± 0.94), single (x = 2.84 ± 1.05), had secondary education (x = 2.65 ± 1.08), students (2.89 ± 1.08), poor (x = 2.63 ± 1.05), and primiparous (x = 2.50 ± 1.08) are more affected and they agreed (grand mean >2.50) hence significant (P = .018, .037, .000, .000, .009, and .036) respectively. Similarly, Abdulraheem and Onajole, 32 and Rahman and Obaida-Nasrin, 33 reported that long walking distances, is associated with incomplete immunization. Contrastingly, respondents in the study of Akwataghibe et al 27 reported health facilities as being generally within walking distance to their households.
Beliefs
The respondents generally disagreed that they have no belief in immunization (x = 1.82 ± 0.81). This showed that mothers believed that immunization is beneficial to them having also agreed to its effectiveness in disease prevention. However, those whose children were partially immunized were more likely to disbelief in immunization (x = 2.14 ± 0.95). Socio-demographic characteristics significantly associated with beliefs as recorded in this study were place of birth (P = .000), number of antenatal visits (P = .000), level of education (P = .000), occupation (P = .002) and wealth index (P = .003). In addition, those who gave birth at home of TBAs (x = 2.12 ± 0.10), had no antenatal visits (x = 2.31 ± 1.06), no formal education (x = 2.27 ± 1.05), no job (x = 2.10 ± 0.93), and poor (x = 2.03 ± 0.77) were more likely not to belief in immunization. At variance with this report Akwataghibe et al 27 reported superstitious belief among respondents hindering immunization completion among children.
Schedule
The mothers generally disagreed with inconvenient immunization schedules (x = 2.00 ± 0.68). However, those whose children were partially immunized disagreed less (x = 2.08 ± 0.75) than those who had their children fully immunized (x = 1.94 ± 0.63) thus inconvenient schedules slightly affect completion of immunization. Socio-demographic characteristics that are significantly associated with this response were, place of delivery (P = .007), no of antenatal visits (P = .004), level of education (P = .000), and number of children living in the household (P = .044). Therefore, those gave birth at home of TBA (x = 2.12 ± 0.66), had no antenatal visit (x = 2.16 ± 0.72), no formal education (x = 1.78 ± 0.69), and up to 6 or more number of children living in the household (x = 2.07 ± 0.73) were more likely to complain of inconvenient immunization schedule.
Time
Respondents slightly disagreed that time spent during immunization was long, however, those whose children were partially immunized agreed (x = 2.50 ± 0.92) to this long duration. Hence log waiting time at immunization negatively affects the immunization utilization of children. Mothers’ age, marital status occupation, and wealth index were significantly associated with this response (P = .000, .0001, .010, and .000) respectively. So mothers who were young (x = 2.69 ± 0.94), single (x = 2.94 ± 1.08), self-employed (x = 2.42 ± 1.04) and poor (x = 2.63 ± 1.07) agreed to long time spent during immunization. Similarly, Abdulraheem and Onajole, 32 Rahji and Ndikom (2013), reported that long waiting time at the facility, is associated with poor completion of RI schedules.
Vaccine Unavailability
The mothers generally disagreed with vaccine unavailability (x = 1.72 ± 0.73). However, those whose children were partially immunized disagreed less (x = 1.75 ± 0.79) than those who had their children fully immunized (x = 1.69 ± 0.69) thus vaccine unavailability slightly affect completion of immunization. Socio-demographic characteristics that is significantly associated with this response were, birth order (P = .016), occupation (P = .003), wealth index (P = .000) and number of children living in the household (P = .035). Therefore, those whose children are older (4 years) (x = 1.94 ± 0.93), birth order >6 (x = 2.40 ± 0.89), had no job (x = 1.79 ± 0.72), poor (x = 1.96 ± 0.70) and having less number of children (1-2) living in the household (x = 1.85 ± 0.77) were more likely to complain of vaccine unavailability. Contrastingly, Unavailability of vaccines at the scheduled times was the most frequent complaint by respondents in other studies. 27
Socio-Demographic Determinants
Birth order, place of delivery, and number of antenatal visits were not significant with factors affecting immunization in this study (P = 0 > .05). The findings of this study are in line with the findings of Noh et al, 21 Al-lela et al, 26 Abdullahi, 34 De Oliveira et al. 35 However, the findings from this study are in complete contrast to other findings from a study in rural Bangladesh which found that sex discrimination plays an important role in immunization coverage, with male children more likely to be fully immunized than their females’ counterparts and mothers having received TT injection were also found to be one of the significant predictors of full immunization coverage for children.33,34,36 Odiit and Amuge, 37 Tagbo et al, 38 Yunusa et al 39 reported that delivery in a health facility is a determinant of parental compliance with routine childhood immunization.
Mothers age, marital status, location, parity, and number of children in the household were not significant (P > .05) with factors affecting immunization. This is in line with the findings of Al-lela et al 26 who found no significant associations between the immunization completeness group and mother’s age. At variance Basheer et al, 5 Rahman and Obaida-Nasrin, 33 Awasthi et al, 40 Adefolalu et al 41 found age to be significant. Also, Yunusa et al 39 opined that there was a significant association between the number of children and the completion of immunization. Also other studies found that parity is a very important determinant of immunization schedule completion.33,40 While Munthali 36 reported that location was significant
Furthermore, in this study mothers’ level of education, occupation, and wealth index were significant (P < .005). This is in line with the findings of Basheer et al, 5 Adefolalu et al, 41 Konwea et al, 30 Antai, 42 Noh et al, 21 Al-lela et al, 26 Yunusa et al, 39 Bbaale, 43 Gidado et al, 44 Tagbo et al, 38 Canavan et al, 45 Feiring et al, 46 Maina et al. 47 Contrastingly, the study of Bbaale, 43 did not indicate any association between the higher income of parents/caregivers and the completion of immunization schedules while Ramavhoya et al 48 and Etana and Deressa, 13 reported not significant in level of education. The difficult terrain of our study area made the work to take extra days. It also took some women time to find their child’s immunization cards which limited the study.
Conclusion
In conclusion, there was a low immunization coverage among children under 5; and among other factorsinvestigated, mothers generally agreed that immunization centers were far from their homes. Reasons for non-completion of immunization was common among mothers whose children were partially immunized. The health facility location factor was significant with mothers who were young (≤20 years), single, had secondary education, students, poor, and primiparous (P < .05) Therefore, we recommend that government and donor agencies involved in policy making should locate health facilities close to homes. Also health education on the importance of immunization should be given to mothers especially those who are young and has low socio-economic status.
Footnotes
Appendix
2019 State Population Projected From 2006.
| Pregnant Women | Population Under 1/Birth Cohort | Population Under 5 | Population Under 15 | 6-59mths | 6-11mths | 12-59mths | |||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| District_Name | Total Population of the District (2018) | Growth Rate (2.8%) | Total Population of the District 2019 (2.8%) | RI | SIAs | AFP | Vita A | Vita A | Vita A | WCBA | 9 -59mths (17%) | ||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
36,933 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
38,122 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
38,235 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
30,875 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
35,447 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
32,425 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
52,239 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
36,768 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
29,434 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
56,978 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
36,179 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
47,793 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
57,649 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
529,077 |
Acknowledgements
We acknowledge all the community heads who directed and gave consent for the research to be carried out in their regions.
Author Contributions
All the authors participated fully in overall development of the paper.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was self-sponsored.
Ethical Approval
Ethical approval was obtained from the Ethics Committee of Ebonyi State Ministry of Health Abakaliki (Reference number: EBS/MOH/ERC/V.53/039).
Informed Consent
Written informed consent was obtained from all subjects before the study.