
Abstract
Anemia represents a significant global public health issue, particularly during the early stages of childhood in developing countries, including Ethiopia. A cross-sectional study was conducted in a hospital with 209 children aged 6 to 59 months. Blood samples were collected from finger/heel pricks and analyzed using the HemoCue Hb 201 analyzer. SPSS was used for data analysis. The overall prevalence of anemia was 29.7%. The study revealed that children with anemic mothers’ history [AOR = 1.76, 95% CI = 1.20-2.60], children of lower monthly income families [AOR = 1.74, 95% CI = 1.19-2.53], children aged 12 to 23 months were identified as the most at risk group [AOR = 3.26, 95% CI = 1.22-8.68] the odds of anemia decreased as the child’s age increased. Providing supplements and enhancing family income for children of anemic mothers and those aged 12 to 23 months should be prioritized to manage anemia in children under 5 in the study area.
Introduction
Anemia is defined as a decrease in the number of red blood cells (RBC), the hemoglobin concentration, and/or the hemoglobin level below the normal range. The severity of anemia can vary according to factors such as age, sex, pregnancy, and altitude, which affect specific physiological needs.1,2
Childhood anemia is a complex issue influenced by various factors such as socioeconomic status, demographic characteristics, feeding practices, access to health services, and maternal anemia during pregnancy. These factors can act independently or in combination, making the condition multifaceted. 3 The risk factors for anemia vary by environment and include nutritional deficiencies (iron, folate, and vitamin B12), genetic hemoglobin disorders, intestinal parasitic infections (IPI), and acute and chronic infections. Iron is a crucial nutrient for human growth at all life stages, especially for children, due to its significant impact on their development. 4 In children under five, anemia is primarily caused by iron deficiency, but deficiencies in other micronutrients like folate, vitamin A, and vitamin B12 also contribute. 5
According to the WHO report, the global prevalence of anemia was 39.8% (95% UI 36.0%, 43.8%) among children aged 6 to 59 months, that is, 269 million children were affected by anemia in 2019. The highest prevalence of anemia in children under 5 years of age was observed in the African region, at 60.2% (95% UI 56.6%, 63.7%). 6 The prevalence of anemia in this region is estimated to be high, translating to approximately 83.5 million children in sub-Saharan countries.7 -9 Even in Ethiopia, a developing country in Africa, anemia remains a moderate to severe problem. A recent study reported that the combined prevalence of anemia among children aged 6 to 23 months was 57.76%, which is within the range of the World Health Organization for a serious public health problem. 10
Anemia in children can lead to a lower developmental index, poor motor development, lack of interest in their surroundings, shorter attention span, reduced cognitive abilities, and behavioral problems. All these factors hurt school achievement and overall behavioral development. Childhood anemia is a common disease that causes significant morbidity and mortality. 11
In numerous pastoral communities, awareness of this issue is limited due to a scarcity of studies. Research into this problem has greatly helped policymakers formulate plans and policies to address these challenges. To reduce the prevalence and severity of anemia, it is important to identify and target the underlying risk factors in pastoral communities. This study aimed to analyze the prevalence and determinants of anemia among children aged 6 to 59 months in the pastoral community of Borena, Borana zone, southern Ethiopia in 2023, at Yabelo General Hospital.
Methods
Study Setting, Design, and Study Population
The cross-sectional study was conducted at Yabelo General Hospital in the Borana zone of Oromia Regional State in Ethiopia, from February to June 2023, in a predominantly pastoralist community. Borena is located 567 km south of Addis Ababa, with Yabelo Town as its capital. The city has 1 general government hospital and 1 health center. Yabelo General Hospital, located in Yabelo City, offers a variety of health services such as laboratory work, delivery, outpatient treatment, care for children under 5 years of age, and prenatal care, serving the 926 690 residents of Borena Zone. 12
Sample Size and Sampling Procedures
The sample size was calculated using the single-population proportion formula, considering the prevalence of anemia among children under 5 years of age from a previous study carried out at Bule Hora General Hospital, 13 a 5% error margin, and an additional 10% for non-responses, result in a total sample size of 209. The study participants were enrolled using convenience sampling techniques. The study included children aged 6 to 59 months who visited Yabelo General Hospital during the study period, with their guardians or parents volunteering to participate and providing informed consent. However, children with a history of blood transfusion or surgery within the last 2 months were excluded.
Data Collection Method
To gather information about the family and child, we conducted interviews with the child’s mother and other caregivers using structured and pre-tested questionnaires. Data were collected on socioeconomic and demographic information, eating habits, and other risk factors. We assessed the mid-upper arm circumference (MUAC), height, and weight of the children according to the 2008 World Health Organization (WHO) standard. Each child was weighed using a portable weight scale while wearing only light clothing and standing barefoot in the center of a platform for a portable digital weight measuring scale. We used a known-weight object to calibrate the scale. Height was measured using a stadiometer in the Frankfurt position to the closest 0.1 cm. Each measurement was performed twice and the average results were used to analyze the anthropometry data.
Sample Collection, Processing, and Data Quality Assurance
Capillary blood samples were collected from each child to determine hemoglobin concentration using a hemoglobin analyzer or hemoCue. A drop of capillary blood was carefully collected from a finger prick (or a heel prick in children aged 6-11 months) after the first drop of blood was wiped with cotton wool. The filled microcuvette was loaded into the cuvette holder of the calibrated HemoCue Hb 201 analyzer and after a few seconds, hemoglobin measurement was performed. The results were recorded using a questionnaire. To ensure the reliability and validity of the study, the pre-analysis, analytical, and post-analysis steps were strictly applied immediately before, during, and after laboratory tests. The HemoCue was calibrated following manufacturer instructions before beginning of blood sample test. Quality control was carried out to ensure instrument performance.
Data Analysis
The data were coded, cleaned, and entered into EpiData version 3.1 for analysis. Analysis was carried out using SPSS version 25 (IBM® SPSS®, IBM Corp., Armonk, NY, USA). Descriptive analysis was performed and the results were presented as numbers and percentages or mean ± SD. The binary logistic regression model was used to identify determinants of anemia among children under 5 years old children. Statistical significance was considered at P < .05. The assessment of multicollinearity was checked using the variance inflation factor (VIF), and the result was 2.4. The fitness of the multivariable binary logistic regression model was tested using the Hosmer-Lemeshow test result was P = .62, and the model was considered to have a reasonable fit if P > .05.
Result
Sociodemographic Characteristics of Study Participants
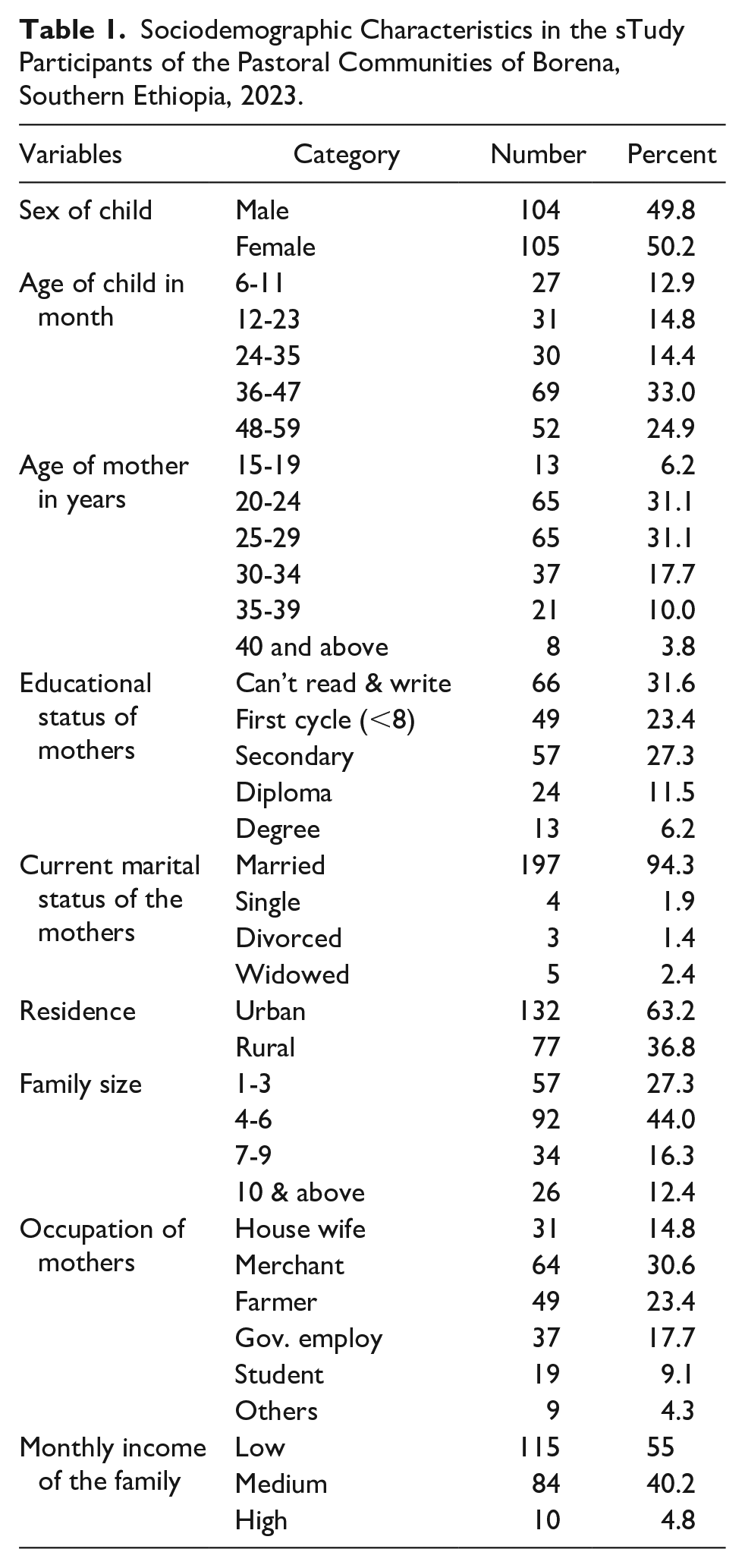
In the study, a total of 209 children aged 6 to 59 months were included. Children were categorized by age as follows: 6 to 11 months (12.9%), 12 to 23 months (14.8%), 24 to 35 months (14.4%), 36 to 47 months (33%), and 48 to 59 months (24.9%). The mothers’ age range was 15 to 49 years old. Regarding marital status, 197 (94.3%) mothers were married, 4 (1.9%) were single, 3 (1.4%) were divorced, and 5 (2.4%) were widowed. In terms of educational status, 66 (31.6%) mothers were unable to read and write, 49 (23.4%) attended elementary classes, 57 (27.3%) attended secondary school and 37 (17.7%) attended diplomas and higher. Approximately 92 (44%) families had 4 to 6 children, 57 (27.3%) had 1 to 3 children, and 26 (12.4%) had more than 10 children in their household (Table 1).
Sociodemographic Characteristics in the sTudy Participants of the Pastoral Communities of Borena, Southern Ethiopia, 2023.
Birth Order & Complementary Food-Related Results
Regarding the order of birth of the majority of children, approximately 67 (32.1%) were fourth or later born, and approximately 15.8% were first born in their household (Table 2).
Conditions of the Children of the Pastoral Community of Borena, Borana Zone, Southern Ethiopia, 2023.

Prevalence of Anemia Among 6 to 59 Children
During the study, 209 children aged 6 to 59 months were included, and 62 of them were found to be anemic, resulting in an overall prevalence of 29.7% [95% CI = 23.5-35.9]. This means that of the 209 children surveyed at Yabelo General Hospital, almost one-third were anemic (Figure 1).

The prevalence of anemia in number showed over all prevalence (number of children being anemic).
Prevalence of Anemia Among Children
The child’s hemoglobin level was used to determine the severity of their anemia. The range of hemoglobin levels was from 6.5 to 14.5 mg/dl, with an average of approximately 11.48 (±1.53) mg/dl. Children with severe malnutrition had higher levels of anemia compared to children with regular nutrition. As a result, 62 (29.7%) of the children were found to be anemic, out of which only 6 (2.9%) were determined to be severely anemic, 24 (11.5%) moderately anemic, and 32 (15.3%) slightly anemic (Figure 2).

Prevalence of anemia level in children aged 6 to 59 months attending the EPI and under 5 clinics of Yabelo General Hospital, 2023.
Determinants of Anemia Among Under-5 Years Old Children Attended at Yabelo General Hospital
The multivariable logistic regression analysis indicated that maternal anemia history, children’s age group, and household monthly income were significant determinants of anemia among children under 5 years old at Yabelo General Hospital. Children aged 12 to 23 months were the most at-risk group, with a 3 times higher risk of anemia compared to children aged 48 to 59 months [AOR = 3.26, 95% CI = 1.22-8.68], P-value = .018]. Children with mothers with a history of anemia were nearly 2 times more likely to be anemic compared to those with nonanemic mothers [AOR = 1.76, 95% CI = 1.20-2.60]. Similarly, children from households with lower monthly incomes were nearly 2 times more likely to be anemic compared to those from higher-income households [AOR = 1.74, 95% CI = 1.19-2.53] (Table 3).
Determinants of Anemia Among Under-5 Years Old Children Attended at Yabelo General Hospital.

Low income ≤ 5000 ETB, Medium = 5001 to 15 000 ETB, High ≥ 15 001 ETB.
Abbreviation: ETB, Ethiopian birr; COR, crude odds ratio; AOR, adjusted OR; CI, confidence interval.
Statistical significance at P < .05.
Discussions
This study evaluated the prevalence of anemia and its determinants among children aged 6 to 59 months. The overall prevalence of anemia among under-five children was 29.7% (95% CI = 23.5–35.9). This finding is consistent with the study done in Gondar, which reported 28.6%, 14 and the systematic review and meta-analysis study in Ethiopia, which reported 34.4%. 15 The prevalence reported in the current study exceeds 13.2% in the West Guji Zone in southern Ethiopia, 16 10.2% from daycare centers in Brazil, 17 and 9.7% from Ebonyi, Nigeria, in Sub-Saharan Africa. 18 This disparity could stem from socioeconomic challenges, insufficient government interventions, suboptimal child-feeding practices, and limited maternal education within the pastoralist community of the Borena area.
The finding of the current study was lower than several other studies: 48.9% at Shanan Gibe Hospital in Oromia, 19 41.1% at Guguftu Health Centre in Wollo, Amhara, 20 36.7% at Assela Referral Hospital in Oromia, 21 52.2% in Kombolcha town, northeast Ethiopia, 22 and 57.6% in a further analysis of the Ethiopian demographic health survey in 2016. 23 The discrepancy in anemia rates could be due to variations in sample size, dietary conditions, socioeconomic status, location, measurement sensitivity, and study area. Given the high prevalence of anemia in this region, it is important to implement new prevention and control measures.
The recent study revealed that a history of maternal anemia, the age group of the children, and the household’s monthly income are significant factors influencing anemia in children under 5 years old at Yabelo General Hospital. The children from households with lower monthly incomes were almost twice as likely to suffer from anemia compared to those from wealthier families. This finding is consistent with the research conducted in sub-Saharan Africa, which found an association between lower household wealth status and anemia in children under five, 24 as well as the Ethiopian Demographic Health Survey of 2016. 23 This is attributed to the fact that households with higher incomes tend to provide their children with nutritious foods and drinks that can safeguard their health and prevent anemia. This is why children in the poorest families are less likely to have a balanced diet, as they cannot afford and use diversified foods, making them susceptible to poor health conditions that lead to anemia, such as parasitic infections. 23
The study found that children under 24 months old were more likely to have anemia compared to older children and that anemia decreased as children got older. This report aligns with the findings of numerous studies carried out in Ethiopia and other countries such as the analysis of Ethiopian Demographic Health Survey 2016 data. 23 This may be because younger children experience rapid growth and have higher nutrient demands, including iron. Furthermore, the low iron concentration in breast milk may not meet the iron needs of breastfeeding children. 25
In the current study, maternal anemia history is strongly related to childhood anemia. Children born to mothers with a history of anemia were more likely to be anemic compared to those whose mothers did not have such a history. This report is consistent with research conducted in Sub-Saharan countries 24 and the Ethiopian Demographic Health Survey of 2016. 23 This could be attributed to the fact that mothers and their children share the same living environment, as well as similar socioeconomic and dietary conditions, which in turn can contribute to the prevalence of anemia as a reflection of the overall nutritional status of the household. 3
In the current study, the children classified as severely anemic were 2.9%. This report is supported by the study conducted in sub-Saharan countries that reported 3%. 24 However, the current study report is less than the findings from West Guji Zone Bule Hora General Hospital in the West Guji Zone. 26 The observed difference may be attributed to our study, which enrolled asymptomatic children who were attending the hospital.
Limitations of the Study
The study has certain limitations: it employed non-probability sampling methods with a limited sample size, making the findings not generalizable to the entire community. Additionally, the cross-sectional design of the study does not allow for the determination of cause-and-effect relationships. The study did not assess factors such as severe dental caries, which could be related to anemia. Furthermore, the study only included children under 5 who visited one health facility.
Conclusions and Recommendations
The study revealed that anemia is a significant public health issue in the study area. Factors such as the age of the children (in months), the history of maternal anemia, and household wealth/income were found to be the determinants of childhood anemia. The study revealed that children under 24 months of age were more likely to have anemia compared to older children. To manage anemia in children under 5 in pastoralist regions, specific supplements are essential, particularly for children of anemic mothers and those aged 12 to 23 months. These efforts should be combined with initiatives to enhance family income.
Supplemental Material
sj-docx-1-gph-10.1177_2333794X241310547 – Supplemental material for Burden and Determinants of Anemia Among 6 to 59-Month-old Children in the Pastoral Communities of Borana, Borana Zone, Southern Ethiopia
Supplemental material, sj-docx-1-gph-10.1177_2333794X241310547 for Burden and Determinants of Anemia Among 6 to 59-Month-old Children in the Pastoral Communities of Borana, Borana Zone, Southern Ethiopia by Girma Ashenafi, Alqeer Aliyo and Bontu Tesfa in Global Pediatric Health
Footnotes
Acknowledgements
We would like to thank the study participants and the Yabelo General Hospital staff, especially the data collectors and laboratory staff, for their valuable contributions.
Author Contributions
All authors involved in conceptualization, proposal development, design, project management, research and monitoring, data analysis, supervise, data collection process, performed, document preparation, interpretation, wrote and manuscript preparation. All authors read and approved the final manuscript.
Availability of Data and Materials
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Consent of Publication
Not applicable.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval and Consent to Participate
An official letter was obtained from the Institutional Review Board of Bule Hora University with reference number BHUIRB 0063/2023. Additionally, a permission letter was obtained from the Borana Zone Health Bureau and was submitted to the hospital administration. The protocol, importance and risks were explained to the parents or guardians of the participants, and written informed consent was obtained under the principles of the Declaration of Helsinki. Participation in the study was voluntary and refusal was possible. Data confidentiality was maintained using a specific coding number.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.