
Abstract
We aimed to identify clinical predictors of fatal outcome in children under 5 years of age having diarrhea and severe sepsis and treated in the Intensive Care Unit of the Dhaka Hospital of icddr,b from October 2010 through September 2011. Among 191 enrolled children, 70 (37%) died and were considered to be cases, while the remaining 121 (63%) who survived constituted the controls. The cases more often had shortness of breath (SOB), septic shock, dehydrating diarrhea compared with the controls (for all, P < .05). After adjusting for potential confounders using logistic regression analysis, the likelihood of death was higher in children who had septic shock and SOB and lower in children having dehydrating diarrhea (for all, P < .05). Thus, SOB can trigger an early alarm for sepsis recognition; otherwise, these children can end up with fatality from septic shock. In resource-poor settings, early identification of these predictors can alleviate death.
Introduction
Pediatric sepsis is the leading cause of hospital deaths, 1 and percentages are presumed to be higher in diarrheal children especially in resource-poor settings.2,3 Sepsis with its ability to produce severe sepsis, septic shock, multi-organ failure, and death 2 is a major health care problem. Though the number of under-5 deaths decreased from 16.4 million in 1970 to 5.0 million in 2016, 4 in southern Asia and sub-Saharan Africa, more than 50% of all under-5 deaths are caused by infectious diseases, having features of sepsis or septic shock. 2 Low- and middle-income countries like Bangladesh face an enormous economic burden due to the increasing number of severe sepsis. 5
Sepsis results from a complex interplay between host, pathogen, and health system response factors where the body’s unregulated inflammatory response to an infection injures its own tissues and organs.2,6 Early recognition of sepsis is crucial to administer antibiotics, fluid, and inotrop to prevent the development of septic shock and its fatal consequences.2,7,8 However, results in studies comparing early versus usual sepsis care 9 did not find any difference. A study conducted by Maitland et al found early fluid resuscitation was associated with high mortality in children, 10 whereas other studies demonstrated aggressive fluid resuscitation improves the outcome of severe sepsis and septic shock.7,11,12
Despite advances in prevention and treatment, children with severe sepsis continue to represent significant treatment challenges. 13 Children with diarrhea often present with overlapping clinical signs, with shock resulting either from severe dehydration or severe sepsis or both. However, children with diarrhea having hypovolemic shock used to respond with fluid resuscitation, whereas lack of response to fluid resuscitation is almost invariable in children with septic shock. 14
The intensive care unit (ICU) of the Dhaka Hospital of the International Centre for Diarrhoeal Diseases Research, Bangladesh (icddr,b) provides care for a number of children with diarrhea having severe sepsis and/or septic shock. Despite the implementation of the survival sepsis guideline, we often encounter a high number of deaths in these children. 8 Severe sepsis and septic shock result in mortality of 14% and 67%, respectively, 3 and 33% mortality was observed when there are signs of systemic inflammatory response syndrome and bacteremia. 15 However, data on the risk factors for severe sepsis are limited, especially in children with diarrhea. We hypothesized that there are clinical, demographic, and laboratory parameters that independently predict severe sepsis progression to a fatal outcome. Therefore, the aim of this study was to evaluate the clinical characteristics of children having diarrhea and severe sepsis and compare the survivors with the nonsurvivors to identify the independent predictors of death.
Methods
Ethical Statement
In this retrospective chart analysis, patients or caregivers were not asked for an interview. Data were de-identified before analysis. This study was approved by the Research Review Committee and Ethical Review Committee of icddr,b.
Study Design
We conducted a retrospective analysis of all diarrheal children of either sex, aged 0 to 59 months, treated for severe sepsis in the ICU from October 2010 through September 2011. Sepsis was defined as tachycardia plus hypothermia (≤35.0°C) or hyperthermia (≥38.5°C), or abnormal white blood cell count plus the presumed presence of infection. Severe sepsis was defined as the presence of sepsis plus poor peripheral perfusion (age-specific hypotension and/or absent peripheral pulses and/or delayed capillary refilling time in the absence of dehydration or after correction of dehydration, if any). Objective parameters for detection of severe sepsis were the following: a mean arterial pressure of <50 mm Hg and/or urine output <1 mL/kg/h and capillary refill time of >3 seconds. Patients were categorized as septic shock if they were unresponsive to fluid (normal saline/cholera saline) boluses (20 mL/kg with a maximum of 40 mL/kg for severely malnourished children over 2 hours and 60 mL/kg over 10-15 minutes for the children without severe malnutrition) and required the support of inotropes.3,16 The comparison was made between survivors and nonsurvivors.
Study Site
This study was conducted at the Dhaka Hospital of icddr,b, which often caters to around 150 000 patients annually. The ICU of this hospital manages around 1000 children under 5 years of age each year. The detailed description of the study site has been provided elsewhere. 16
Patient Management
All children (both cases and controls) admitted to the ICU received standard management following the hospital guidelines. At the ICU, peripheral capillary oxygen saturation is measured using a portable pulse oximeter (OxiMaxN-600; Nellcor, Boulder, CO), and blood glucose is estimated using a Gluco-check machine (STADA, Bad Vilbel, Germany). Children with hypoxemia receive oxygen supplementation through nasal prongs (2 L/min) or a mask (5 L/min). Dehydration is corrected following the World Health Organization (WHO) guidelines using oral fluids (oral rehydration salt solution) for those with some dehydration or intravenous fluids (mostly cholera saline) for those with severe dehydration or unable to drink for any reason. 17 Appropriate feeding, with micronutrients, vitamins, and minerals, is provided.
Regarding antibiotics, Dhaka Hospital follows its own evidence-based protocol depending on local pathogen epidemiology and sensitivity pattern. As a part of sepsis management, well-nourished children get injection ampicillin and injection gentamycin and malnourished children get third-generation cephalosporin (usually injection ceftriaxone) and injection gentamicin.12,16 Injection levofloxacin is added instead of injection gentamicin if there is concomitant pneumonia. 16 Antibiotics are also changed if there is rapid deterioration within 24 hours or no improvement after 48 hours. 18 After 72 hours of the availability of blood culture reports, antibiotics are adjusted accordingly.12,18
After correcting any dehydration, as defined by the Dhaka method, which is almost similar to the WHO method and approved by the WHO, 19 patients were assessed for features of severe sepsis, and intravenous fluid is administered to patients with severe sepsis following the surviving sepsis guidelines. 8 Patients with septic shock (unresponsive to fluid resuscitation) having severe acute malnutrition received blood transfusions as suggested by the WHO. 17 In resource-poor settings like Bangladesh, it is difficult to arrange safe blood promptly. So, inotropes are started in children who developed septic shock, without waiting for a blood transfusion. However, a transfusion is given as soon as the blood becomes available. Our treatment goal is to achieve good peripheral perfusion, with a mean arterial pressure of >50 mm Hg and/or urine output >1 mL/kg/h and capillary refill time of <3 seconds. Mechanical ventilation is used to manage children admitted to the ICU with respiratory failure.
Measurements
Case report forms were developed, pretested, and finalized for the acquisition of relevant data. Data collection of these children included age, gender, socioeconomic status, presence of vomiting, abdominal distension, poor intake, shortness of breath (SOB), exclusive breast feeding, vaccination according to expanded program on immunization schedule, prior antibiotic usage, presence of severe acute malnutrition, mental status (abnormally sleepy), convulsion, dehydrating diarrhea, respiratory rate, hypoxemia (peripheral capillary oxygen saturation <90% in room air), adventitious breath sound, pneumonia, septic shock, required change of antibiotics, bacteremia, pathogen in stool, raised serum creatinine (1.5 times the upper limit of normal [ie, >53 µmol/L for infants and >93 µmol/L for children aged >1 year]), hypokalemia (serum potassium <3.5 mmol/L) or hyperkalemia (serum potassium >5.3 mmol/L), hyponatremia (serum sodium <135 mmol/L), hypernatremia (serum sodium >150 mmol/L), hypocalcemia (serum calcium <2.12 mmol/L), hypomagnesemia (serum magnesium <0.65 mmol/L), hypermagnesemia (serum magnesium >1.05 mmol/L), metabolic acidosis (serum TCO2 <18 mmol/L), blood transfusion, and mechanical ventilation. The socioeconomic condition was considered poor if caregivers live in a slum and/or in a tin-shaded house as monthly income was not recorded on the questionnaire.
Statistical Analysis
All data were entered into a personal computer and edited before analysis using SPSS for Windows (version 20.0, IBM Corp, Armonk, NY) and Epi Info (version 7.0, Epi Info Software; Center for Disease Control and Prevention, Atlanta, GA). Differences in proportions were compared by the χ2 test or Fisher’s exact test as and when applicable and differences of means were compared by the Student’s t test, and the Mann-Whitney U test was used for comparing data that were not normally distributed. P < .05 was considered statistically significant. The strength of association was determined by calculating the odds ratio and their 95% confidence intervals. To identify clinical predictors associated with death, variables were initially analyzed in a bivariate model, and then, after adjusting with potential confounders, a multiple logistic regression model was used to identify the independent predictors.
Results
During the study period, 191 diarrheal children under 5 years of age were found to be treated for severe sepsis, and among them, 70 (37%) died.
In bivariate analysis, children among the nonsurvivors often presented with SOB, abnormal sleepiness, septic shock, less often had dehydrating diarrhea, more often progressed to septic shock and received inotropes, and required more mechanical ventilation compared with the survivors (Table 1). Other variables including systolic and diastolic blood pressure and total leukocyte count were comparable between the groups (Tables 1 and 2). Among the cases, 75% had no dehydration and 25% had some or severe dehydration, whereas among the controls, 51% had no dehydration and 49% had some or severe dehydration.
Characteristics of Children Under 5 Years of Age With Diarrhea and Severe Sepsis Having Fatal Outcome Compared With Survivors.
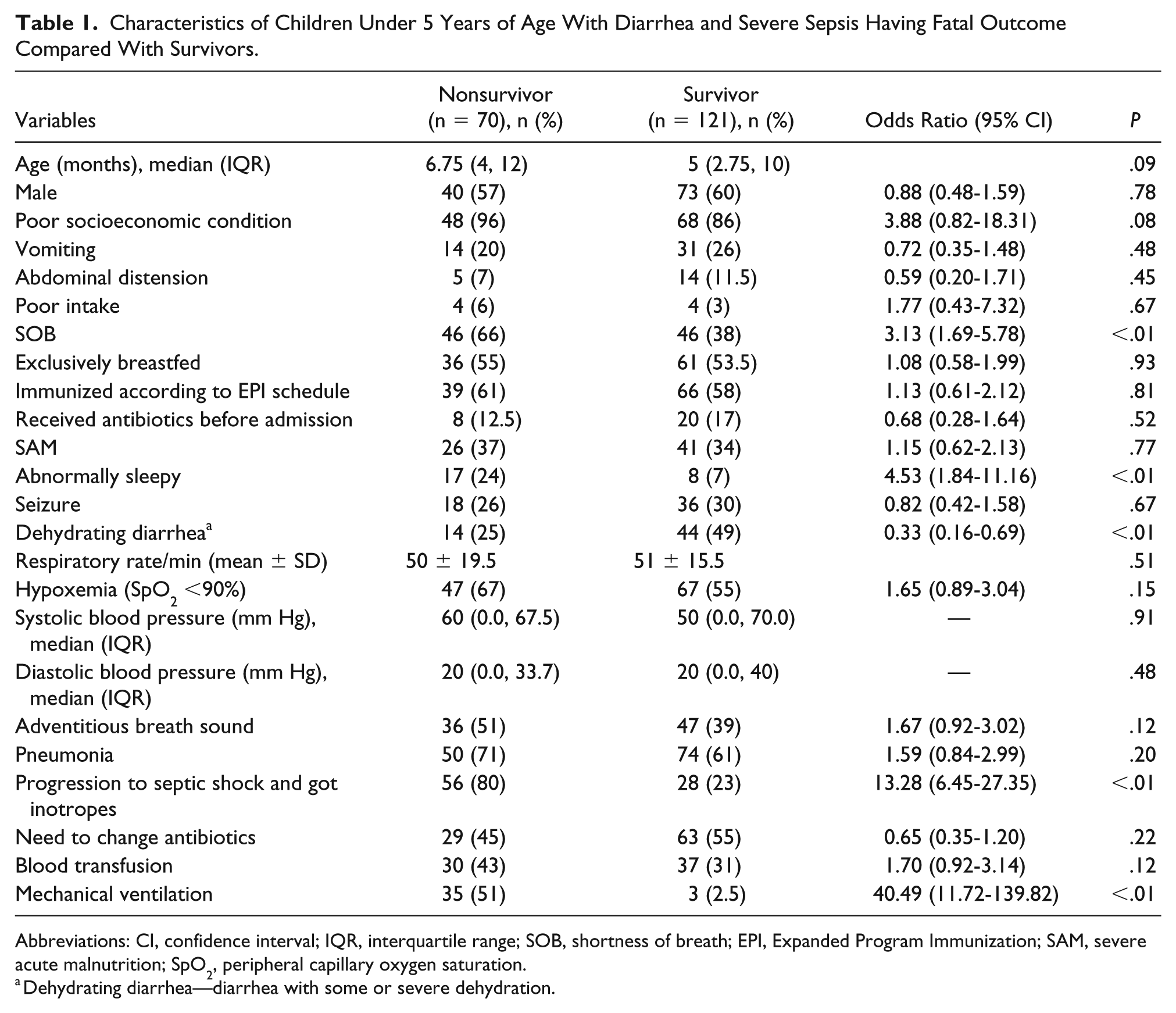
Abbreviations: CI, confidence interval; IQR, interquartile range; SOB, shortness of breath; EPI, Expanded Program Immunization; SAM, severe acute malnutrition; SpO2, peripheral capillary oxygen saturation.
Dehydrating diarrhea—diarrhea with some or severe dehydration.
Laboratory Characteristics of the Study Children.

Abbreviations: CI, confidence interval; IQR, interquartile range.
In logistic regression analysis, after adjusting for potential confounders, such as abnormal sleepiness, the independent predictors of death in diarrheal children under 5 years of age having severe sepsis, either at admission or during hospitalization were SOB and septic shock, and independent predictor of survival was dehydrating diarrhea (Table 3).
Logistic Regression Analysis to Explore the Clinical Predictors of Death.

Blood culture isolates among the survivors and the nonsurvivors are shown in Table 4. Gram negatives (14/17 [82%] vs 25/29 [86%]) were predominant in both groups.
Bacterial Isolates From Blood of the Study Patients.

Discussion
In diarrheal children having severe sepsis, SOB and septic shock were the independent predictors of death, whereas dehydrating diarrhea was less frequently associated with deaths. These are the main observation of this study.
SOB is a clinical sign of sepsis that can rapidly cause tissue damage, organ failure, and death. 20 In sepsis, there is a circulatory compromise that in turn causes global tissue hypoxemia leading to SOB by producing a mismatch between systemic oxygen delivery and oxygen supply. 21 In our study population, we observed significantly higher death among cases where severe sepsis progressed to septic shock. Septic shock leading to death in diarrheal children was also observed in other studies. 15 In severe sepsis, amplified cytokines or other inflammatory stimuli causes microcirculatory and endothelial damages with vasodilatation and capillary leakage 22 as a result of disrupted tissue oxygenation, anaerobic cellular respiration with increased lactate production, and development of metabolic acidosis. 19 The cellular injury, accompanied by the release of pro-inflammatory and anti-inflammatory mediators, often progresses to organ dysfunction, commonly involving the circulation, lung, gastrointestinal tract, kidney, and nervous system. 23 Multi-organ failure is one of the main cause of death in patients with severe sepsis. 24 All these children with severe sepsis had received fluid resuscitation following protocolized management guidelines in the hospital.3,12,16 Though controversy exists, there is also evidence that early, aggressive fluid resuscitation improves the outcome of severe sepsis and septic shock. 7
In our study, we found that the nonsurvivors had fewer numbers of dehydrating diarrhea than the survivors. We do not have any ready explanation for that. One possible explanation is that the Dhaka Hospital of icddr,b is the specialized diarrheal hospital and all the clinicians are highly expert in assessing dehydration and their prompt management. Thus, the patients with dehydration (some or severe) were assessed correctly immediately after admission and had received immediate treatment including fluids resuscitation as the signs of dehydrating diarrhea are more visible compared with the signs of severe sepsis. These patients also received frequent follow-ups. This might help eliminate the dehydration-related SOB25,26 in our study population. Still, the probability of coexistence of dehydration and severe sepsis could not be ruled out, and in that scenario, patients received early fluid resuscitation.
Regarding outcome, nonsurvivors required more mechanical ventilation and it is understandable. Chisti et al also found similar findings in under 5 diarrheal children. 27 In our study, no survival benefit was observed among children who got a blood transfusion (Table 1). In critically ill septic patients, red blood cell transfusion is associated with a dose-dependent increase in morbidity and mortality. Bachou et al also observed blood transfusion was associated with increased risk of hospital deaths among severely malnourished children in Africa. 28 The WHO advocates blood transfusions for reducing mortality in severely malnourished children with septic shock. 7 And there are studies where survival benefits were observed when the early transfusion was arranged as a part of early goal-directed therapy. 7 One explanation might be due to resource constraint, as blood and blood products are not readily available in our country. On the other hand, when the deleterious cascade of sepsis is on, already there is a diffuse cellular injury with organ dysfunction, which cannot be reversed only with blood to increase oxygen transport to tissue. 23
Moreover, identification of the offending organism is crucial as inappropriate antibiotics increase the probability of septic shock progression from gram-negative bacteremia. 29 Both the groups had evenly distributed bacteremia (82% vs 86%), and those were predominantly gram negatives. Gram-negative bacteremia in diarrheal children admitted to the critical care units has previously been reported. 15 The translocation of gram-negative bacteria through the diseased and inflamed gut of diarrheal children is a possibility for this sepsis. 30 In our study, isolation of any offending organism was possible in 25% (46/186) of cases. For patients presenting with sepsis, our findings also support the recommendation of surviving sepsis campaign to obtain blood cultures before administration of antibiotics within 1 hour. 8
We acknowledge several limitations of our study. First, as our data were gathered from a single academic hospital, located in the capital of Bangladesh, it is not clear how generalizable our findings are to other settings. Second, we retrieved retrospective data, so due to lack of adequate information, we were unable to formulate severity illness score. Third, due to the small sample, we found wider confidence intervals. Fourth, we only evaluated bacterial pathogens for sepsis and severe sepsis but had limited scope for viral or fungal isolation.
Conclusion
Our data suggest that children with diarrhea having severe sepsis often had a fatal outcome and they frequently presented with SOB and septic shock. Data also suggest that children with diarrhea and severe sepsis who had a fatal outcome were less likely to have dehydrating diarrhea. Therefore, identification of these simple clinical features such as SOB and septic shock in predicting deaths in children under 5 years of age with diarrhea who were treated in ICU for severe sepsis may help design future intervention studies that may further help reduce mortality in such children, especially in resource-poor settings.
Footnotes
Author Contributions
MS, FA, S, TA, NJS, TA, and MJC conceived and designed the study; MS collected, merged, and cleaned the data; MS, FA, S, TA, NJS, TA, and MJC analyzed and interpreted the data; MS, and MJC gave technical support and conceptual advice; MS wrote the first draft of the manuscript and all the authors reviewed the manuscript; MJC finally approved the manuscript. All authors read and approved the final manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by icddr,b and its donors, which provide unrestricted support to the institution for its operations and research. Current donors providing unrestricted support include the Government of the People’s Republic of Bangladesh; Global Affairs Canada (GAC); Swedish International Development Cooperation Agency (SIDA); and the Department for International Development, UK (UKaid).