
Abstract
Pediatric hemorrhagic stroke (HS) has become a problem, determining both a high frequency of fatal outcomes and early disability. The priority objective determining the effectiveness of diagnosis, treatment, and prevention of hemorrhagic stroke is to identify the etiology of the disease. We report a case of hemorrhagic stroke in a 2-month old child with cytomegalovirus infection, which led to a negative outcome of the disease. In the context of the current presentation, a set of neuroimaging, somatic, and laboratory changes in the child with HS is shown. Our case demonstrates a high probability of hemorrhagic stroke in cytomegalovirus infection, which requires an appropriate vigilance and interdisciplinary approach in identifying the cause of hemorrhagic stroke in children.
Introduction
Hemorrhagic stroke in childhood is defined as a cerebrovascular event that occurs between 30 days and 18 years of age. There are 2.9 cases of HS per 100 000 children each year. 1 The etiology of HS in children includes cerebrovascular, cardiovascular diseases, hemostasis, metabolic disorders, and genetic polymorphisms. However, data on HS associated with cytomegalovirus infection is limited. 2 In this report we highlight the case of HS in a 2-month-old child with cytomegalovirus infection.
Case Report
A 2-month-old girl was admitted to the emergency clinic with complaints of restlessness, lethargy, refusal of breastfeeding, pallor, repeated vomiting, and hyperthermia up to 38.2°. These complaints appeared 7 hours before the hospitalization to the clinic.
He baby from the first reported pregnancy and childbirth. The mother was diagnosed with an exacerbation of maxillary sinusitis at 4 months of pregnancy. Anhydrous period of 5 hours, weakness of labor forces and stimulation of labor activity were observed during the birth. Body weight at birth was 2700 g, 8 to 9 points by Apgar scale.
At the admission department of the clinic the child was examined by a neurosurgeon, anesthesiologist, intensive care specialist, pediatrician. The condition was considered as extremely serious. Consciousness by Glasgow Coma Scale (SCG)—5 points. A tense and bulging anterior fontanelle. Meningeal signs were noted—nuchal rigidity, seizure tendency, moderate anisocoria by left-sided pupil dilation, sluggish pupillary, right side ptosis. The skin was jaundiced, mucous pale, cyanosis, acrocyanosis. Petechial rashes were found in the hard palate, bleeding from injection sites.
It was decided to perform a computerized tomography (CT) of the brain. A CT scan of the brain revealed an intracerebral hematoma of the left parietal and temporal lobes. Massive subarachnoid hemorrhage in the left parietal and temporal region. Displacement of medial brain structures to the right by 6 mm. Swelling of the brain (Figure 1).
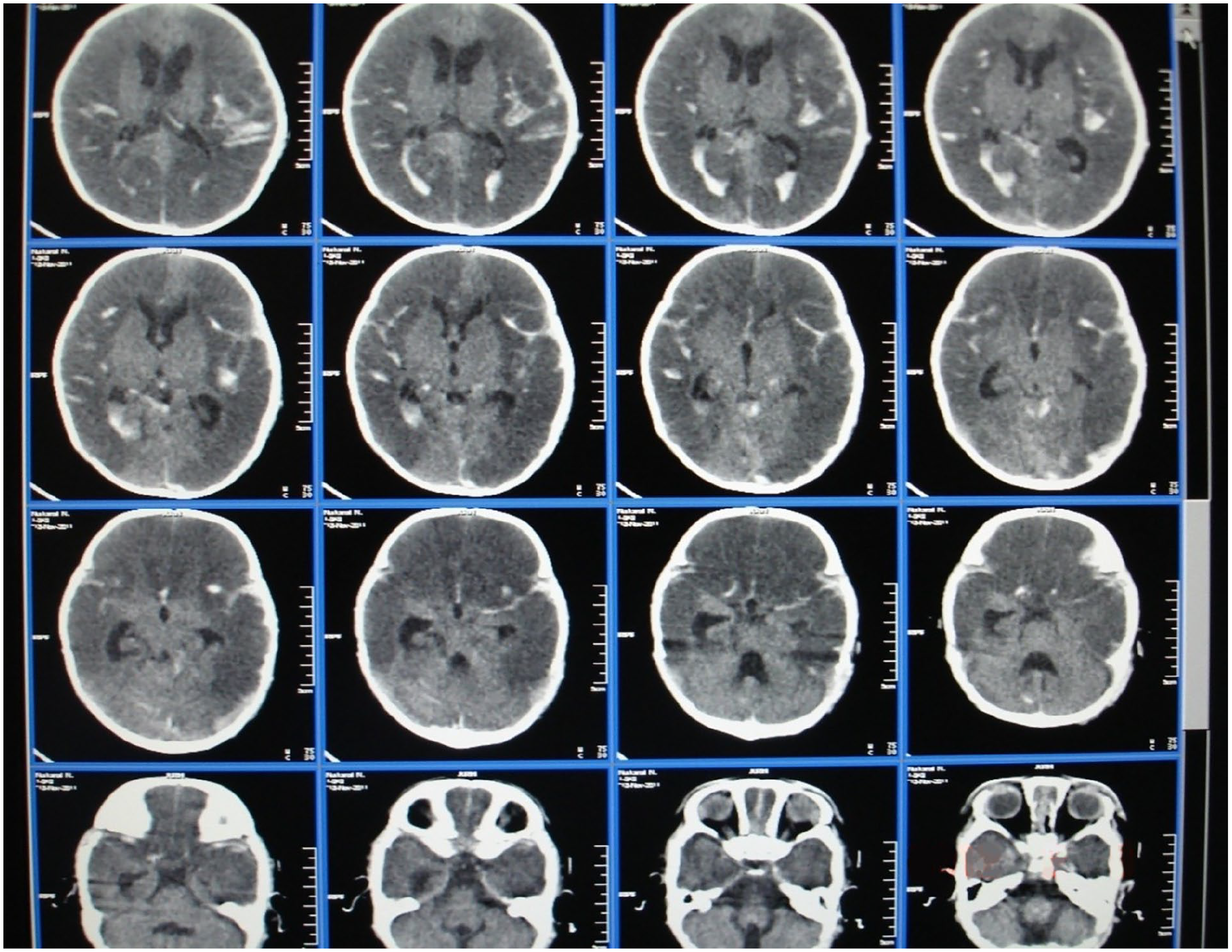
CT—intracerebral hematoma of the left parietal and temporal lobes. Massive subarachnoid hemorrhage in the left parietal and temporal region. Swelling of the brain.
Later, the child had tonic-clonic seizure, bradypnea grew worse—breathing rate was 18 respiratory movements per minute. By auscultation: rough respiration, low and medium bubbling rales.
Muffled heart tones, bradycardia, heart rate was 104 beats/minute. Hepatomegaly (+4 cm).
Endotracheal intubation has been performed due to dyspnea, the child has been transferred to artificial lung ventilation.
Violation of vital functions, acute neurological symptomatology, CT results determined the decision to hospitalize the child to the intensive care unit.
The X-ray imaging made in the intensive care unit revealed 2-sided pneumonia with confluent foci. Abdominal ultrasound imaging showed diffuse changes in hepatic parenchyma, left renal pelvis dilatation. The electrocardiographic examination showed sinus bradycardia 107 per minute, incomplete right bundle branch block.
Given the child’s high body temperature, we performed a polymerase chain reaction of the blood to detect infectious agents. Analysis of polymerase chain reaction revealed class M antibodies to Cytomegalovirus, which indicated the active phase of cytomegalovirus infection.
General and biochemical blood tests were performed, as well as analysis of changes in the hemostasis and fibrinolysis system. Initial abnormalities in the general and biochemical blood tests showed a decrease in the number of erythrocytes to 2.1 × 1012/l, hemoglobin 63 g/l, hematocrit 19. There were also leukocytosis—15.1 × 109/l, accelerated sedimentation rate—33 mm/hour, increase of total bilirubin up to 81 μmol/l, direct fraction—26 μmol/l.
Coagulogram data showed a decrease of platelet count—23 × 109/μl. The aggregation properties of thrombocytes decreased. The platelet aggregation rate was 16%. Plasma procoagulation activity decreased—6.8% per minute, which was accompanied by an increase in thromboplastin inactivation index—4.1% per minute.
The initial phase of blood coagulation (prothrombin activation) was characterized by reduced ability to coagulate blood. The recalcification time of citrate plasma lengthened to 148 seconds. Thrombin generation (II phase of blood coagulation) was accompanied by deficiency of prothrombin complex factors, which was manifested by reduction of prothrombin index to 66%, fibrinogen consumption. Thereby in the III phase of blood coagulation the fibrinogen concentration was 1.9 g/l. Positive values of ethanol gelation test and fibrinogen have been revealed. Hemostasis anticoagulant link activation was indicated by antithrombin content decrease—0.69% and antithrombin III increase—98.1%. Fibrinolytic reactions activation was indicated by fibrinolytic activity growth—47.1 mm2, protein C concentration increase—104%, plasminogen activator activity—29 mm2, plasmin activity—17.1 mm2.
Lumbar puncture results: the liquor flowed under increased pressure. Laboratory analysis of the liquor showed the presence of fresh erythrocytes, incomplete transparency, cytosis of 3 cells, which confirmed subarachnoid hemorrhage.
In spite of the conservative therapy, the condition of the child was progressively worsening: for 3 days the condition according to Glasgow Coma Scale was 3 points, wide, unresponsive pupils, atony, areflexia were observed. Laboratory data without positive dynamics. It was decided to perform a repeat CT scan, as well as neurosonography, which revealed a breakthrough hemorrhage in the lateral ventricles of the brain with cerebral edema (Figure 2).

Neurosonography—there is displacement, dislocation of medial brain structures, increased echogenicity in brain parenchyma and periventricular area, enlargement of lateral ventricles and third ventricle due to hemorrhage in lateral ventricles, cerebral edema.
By the end of the third day the child’s vital function disorder progressed. Uncontrollable hypotension, cardiac arrest, coma, wide pupils, no photoreaction, atony, areflexia with subsequent lethal outcome were observed.
We made the final clinical diagnosis: intrauterine infection, cytomegaloviral infection, active phase.
Complications of the main disease: acute hemorrhagic cerebral circulation disorder. Acute intracerebral hematoma of the left parietal and temporal lobes. Massive subarachnoid hemorrhage in the left parietal and temporal area, intraventric hemorrhage. Swelling, cerebral dislocation. Third-degree coma. Two-sided focal confluent bronchopneumonia, type III respiratory failure, toxic hepatitis. disseminated intravascular coagulation syndrome. Heart failure: polyorgan failure.
Pathological and anatomical diagnosis: intrauterine cytomegalovirus infection, visceral form, cytomegalovirus metamorphosis of the alveol epithelium, 2-sided focal confluent, serous-desquamation, purulent pneumonia, focal gliosis, and focal glial scars in the brain, cytomegaloviral endothelial metamorphosis of the endothelial vessels of the soft membranes, with massive hemorrhages into the stroma of the soft membranes.
Complication: acute intracerebral hematoma of the left parietal and temporal lobes. Massive subarachnoid hemorrhage in left parietal and temporal area, intraventricular hemorrhage. Brain and soft cerebral edema. Related disease: intravenous serous hepatitis. DIC syndrome, polymicrotrombosis with multiple hemorrhages under the serous and mucous membranes, in the respiratory sections of the lungs, in the internal organs. Protein parenchymatous dystrophy of renal tubules, hepatocytes. Type 2 to 3 hymus accidental involution. Cause of death: polyorganic failure.
We believe that the coincidence of clinical and pathological—anatomical diagnosis is complete and indicates the ability of cytomegalovirus infection to lead to hemorrhagic stroke in children.
Discussion
In this clinical observation the development of hemorrhagic stroke (HS) in the child was detected by CT scan, laboratory analysis of the liquor. It showed the presence of fresh red blood cells, as well as data from pathological and anatomical studies.
The HS was associated with Cytomegalovirus infection, which was revealed by polymerase chain reaction on blood. The manifestation of infections in the perinatal period indicates an intrapartum or contact route of infection of children with hemorrhagic stroke. The burdened infectious, obstetric, and gynecological history of mothers, which we have identified, plays a role in the transmission of infectious agents from a mother to a child. Thus, the mother at 4 months of pregnancy was diagnosed with exacerbation of maxillary sinusitis, 5 hours without amniotic fluid, weakness of patrimonial activity, and its stimulation was observed in childbirth.
Harbert et al 3 indicate that a burdened perinatal history was found in 63% of children with cerebrovascular disease, where unfavorable pregnancy and childbirth in the mother is combined in equal proportions with difficulties of adaptation in the neonatal period. The probability of prenatal, perinatal, or postnatal mother-to-child transmission has been demonstrated. 4 Congenital immunodeficiency, the signs of which have been revealed by the results of pathological and anatomical studies with the type 2 to 3 accidental thymus involution, may also have been a factor contributing to the progression of infection. This indicates the pathogenic role of cytomegalovirus infection, capable of suppressing the immune response in the newborn, which is accompanied by activation of a chronic or latent infection. 5
The infection of Cytomegalovirus was accompanied by acute intracerebral hematoma of the left parietal and temporal lobes, massive subarachnoid hemorrhage to the left parieto-hysterical region, and intraventricular hemorrhage.
Hemorrhage determined the symptoms of HS: general cerebral symptomatology with conscious disturbance, repeated vomiting, tonic-clonic seizure. Rigidity of the occipital muscles reflected symptoms of irritation of the brain membranes. Primarily left-sided localization of the pathological process was confirmed by left-sided pupil dilation. The paresis of the optic nerve was manifested by reduced reaction of pupils to light, which was followed by the right side ptosis. The child developed lymphatic dystension syndrome due to progressive intracranial hypertension, cerebral edema, as evidenced by tension and swelling of the large fontanelle, as well as CT data. Jaundice, pale mucous membranes, cyanosis, acrocyanosis caused both by blood loss, posthemorrhagic anemia, and intrauterine infection and liver and lung damage were of diagnostic importance. A significant place of HS in the child was taken by life-threatening disorders of vital functions with bradycardia up to 104 beats/minute, as well as bradypnea with a breathing rate of 18 respiratory movements per minute and subsequent apnea. Bulbar dysfunction was manifested by disorder of sucking, swallowing. There was a disturbance of thermoregulation in the form of hyperthermia up to 38.2°, which was associated with the presence of concomitant pathology of inflammatory genesis in the lungs and liver.
The increase of inflammatory markers: leukocytes (15.1 × 109/l), accelerated SOE (33 mm/hour), and bilirubin level (up to 81 µmol/l), due to the direct fraction (26 µmol/l), as a consequence of the impact of viruses and bacteria on the liver. Posthemorrhagic anemia was accompanied by reduction of red blood cell count to 2.1 × 109/l, hemoglobin to 63 g/l, hematocrit 19%.
Infection with Cytomegalovirus was accompanied by the DIC with development of hypocoagulation and increase of anticoagulant and fibrinolytic potentials. 6 The development of thrombo-haemorrhagic disorders in particular in perinatal and early infancy reflects both the features of the clotting system, characterized by a deficiency of the most procoagulants, and the influence of pathological factors, in particular infective agents on the labile system of hemostasis, liver, vascular endothelium, fetal organs, and newborn. The development of DIC is also considered by literature to be a characteristic feature of cytomegaloviral infection in a child’s intrauterine infection. 7 Under these conditions, the mechanism for realization of cerebral hemorrhage is likely to be lesion of the vascular wall due to inflammation, endothelial dysfunction of cerebral vessels, and DIC syndrome in the hypocoagulation phase.
In conclusion, the risk of hemorrhagic stroke in infants should be recognized as a complication of infection with cytomegaloviral infection.
Footnotes
Author Contributions
All authors contributed to the development of the manuscript. All authors approved the final manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
For de-identified single case reports, institutional review board approval is not required. The patient’s mother has consented to publication of this de-identified case report.