
Abstract
Mental health in adolescents represent a considerable public health issue in developing countries. These problems are considered a source of problem for adolescents’ quality of life. The study objective was to determine the association between mental health problems and sociodemographic variables among adolescents. A cross-sectional study was conducted from October to December 2016 using a school-based survey in 4 districts and 3 cities in West Java Province, Indonesia. Stratified multistage random sampling was used to select junior and senior high school students and self-administered questionnaires were used to collect study data which included: personal data, socioeconomic status scale, and self-reported version of Strengths and Difficulties Questionnaire (SDQ) which divided into 5 subscales. About 3452 adolescents of 32 schools were included in this study, 59% female, 56% junior high school, 56% district residence, most parents’ education were senior high school. The prevalence of mental health problems based on SDQ subscale as total difficulties, conduct problem, emotional symptoms, peer problems, hyperactivity-inattention, were abnormal 31.6, 38.9, 30, 29.3, 15.6, respectively. Mental health problems were more prevalent amongst adolescents in junior high school and residence in district area, with RR and 95% CI were 1.14 (1.04-1.26), and 1.18 (1.08-1.30). As conclusions mental health problems in adolescents were associated with education level and residence area
Introduction
Adolescence, the stage of life between the ages of 10 and 19 years, is a period of transition from childhood to adulthood in the process of developing physical and mental health. 1 Adolescents tend to be healthy, and many health problems in this population have a psychosocial rather than a biological basis. The many physical, psychological, and behavioral changes during adolescence can contribute to psychosocial and mental health problems that can have serious consequences for teens’ development, productivity, and quality of life.2,3 For instance, higher scores among adolescents on scales for mental health problems are associated with lower scores for their emotional well-being and their life satisfaction. 3 Mental health problems account for about 10% to 20% of the burden of illness in adolescence, 1 and the prevalence of mental health problems in adolescents across low- and middle-income countries is high. In a meta-analysis of 10 studies from sub-Saharan Africa of a sample of 9713 children and adolescents, 1 in 7 reported significant mental health difficulties, and in a survey of 51 Asian countries, prevalence’s ranged between 10% and 20%.4-6
There could be high returns on investments in addressing adolescents’ mental health issues.7,8 The failure to recognize and address mental health problems in this population is a serious public health issue with important consequences for the achievement of basic development goals in low- and middle-income countries. There are multidirectional linkages between mental health conditions and socio-demographic variables such as age, sex, education, household size and residency, employment, and income.
Indonesia is the fourth most populous country in the world and considered low to middle income, and about 6% of the population aged 15 and older reports symptoms of anxiety or depression. 9 West Java is the most populous and most densely populated among 34 provinces in Indonesia; it consists of 16 districts and 9 cities and has a population of 46.3 million. In Indonesia Health Research & Analysis 2018, the prevalence of mental or emotional problems was 12.1% (95% CI: 11.6-12.7) among the population in West Java aged 15 years or older. 9 To date, however, there have been no data on the prevalence of mental health problems among West Javanese adolescents aged below 19 years.
The aim of this study was to provide prevalence estimates of mental health problems in high school adolescents aged 12 to 17 years as measured using the Strengths and Difficulties Questionnaire (SDQ) Indonesian version10-12 and to analyze the associations between SDQ scores and socio-demographic variables in West Java Province, Indonesia.
Method
An analytic cross-sectional study was conducted from October to December 2016 that consisted of administering the SDQ in 4 districts and 3 cities in West Java. The sampling method was stratified multistage random sampling as shown in Figure 1 with stratification into 2 categories, semi-urban (district) or urban (city). In the first stage, in each region, students were randomly selected from public and private junior and senior high schools from a sampling frame of districts and city junior and senior high schools provided by the West Java Department of Education. In the second stage, classes were randomly selected from the schools that had been selected in the first stage, and all students in selected classes were administered the questionnaire. The participants were 12 to 17 years old.
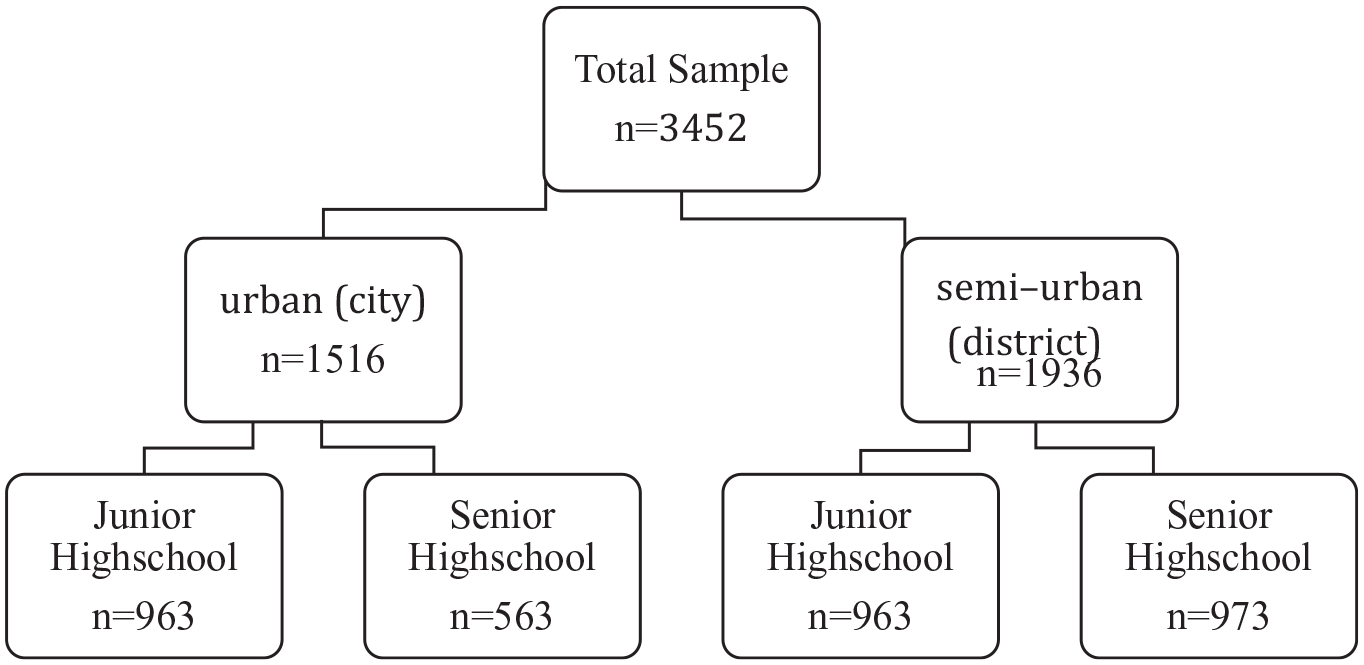
Sampling method.
The study was conducted after approval from the Research Ethics Committee, Universitas Padjadjaran. Written informed consent was obtained from school principals, and parents were given the choice of having their children participate. The ethics committee approved the consent and ascent procedure used in this study. Data were collected using the translated and validated Indonesian version of the SDQ; the scale was self-administered and completed in a single sitting supervised by trained enumerators. Students were assured of confidentiality and that participation was entirely voluntary. They were also provided with information on whom to contact with questions.
The SDQ is a brief screening questionnaire for mental health problems in children aged 3 to 16 years old. It consists of 5 subscales (conduct problems, hyperactivity, emotional symptoms, peer problems, and total difficulties) with 5 items each, and all items are rated on a scale of 0 to 2 where 0 = not true, 1 = somewhat true, and 2 = certainly true; excluding the items for total difficulties, the total SDQ score ranges between 0 and 40 divided into 1 of 3 categories: normal, borderline, or abnormal. The higher the total difficulties score, the more severe the mental or emotional problems.13-15 The SDQ has been translated into Indonesian and has been validated.11,12 In addition to completing the SDQ, the adolescent study participants each completed a structured face-to-face interview to give socio-demographic information (gender, level of education, residence location, parents’ education level). Descriptive analysis was performed on the characteristics and frequency of mental and emotional health status using chi-square, relative risk (RR), and 95% confidence intervals (CIs). Data were processed using SPSS software version 25, and statistical significance was set at P < .05.
Results
Table 1 presents the socio-demographic characteristics of the 3452 adolescent study participants from 32 schools in West Java. Specifically, the table summarizes the respondents’ gender, education level, and location as well as their parents’ education levels. By gender, 2008 participants, 58.6%, were girls, and 1926, 55.8%, were in junior high school. By parents’ education level, 36.2% of the students’ mothers and 37.4% of their fathers had graduated high school.
Socio-Demographic Characteristics of Adolescents in West Java, 2016 (n = 3452).

Figure 2 presents the distributions of the students’ SDQ subscale and total difficulties scores, not including missing values. Specifically, the missing data were as follows: conduct problems, 205 students (5.9%); hyperactivity, 134 (3.9%); emotional symptoms, 225 (6.5%); and peer problems, 166 (4.8%). The majority of adolescents in this study showed mental health scores within the normal range on all SDQ subscales and for total difficulties, but some students did show borderline and abnormal scores. Specifically, the highest prevalence of borderline (19.3%) and abnormal (19.6%) scores were on the conduct problems subscale; the prevalence for abnormal score defined as borderline score plus abnormal score was also the highest for conduct problems at 38.9% (95% CI: 39.7-43.1). The students’ overall average mental health measured as the SDQ total difficulties score was 31.6% (95% CI: 35.9-39.4), which was in the borderline range.

A distribution of mental health problems of adolescents in West Java.
Table 2 shows the distribution of the adolescents’ mental health scores based on their socio-demographic characteristics. The values in the “Abnormal” column reflect the students’ borderline scores added to their abnormal scores in each category. The highest percentage of mental and emotional disorders, 42.2%, occurred among students whose fathers had a junior high school education. Students whose mothers had attended no education also had a high percentage, 40.6%, of mental health disorders.
Mental Health Status by Socio-Demographic Variables.

Table 3 shows the associations between SDQ subscale scores and socio-demographic characteristics. There were significant associations between conduct problems with sex, education, residence, father’s education, between hyperactivity with father’s education, between emotional symptoms with sex, residence, father’s education, between peer problems with sex, residence, and between total difficulties with education, residence.
Association Between SDQ Subscale With Socio-Demographic Characteristics.
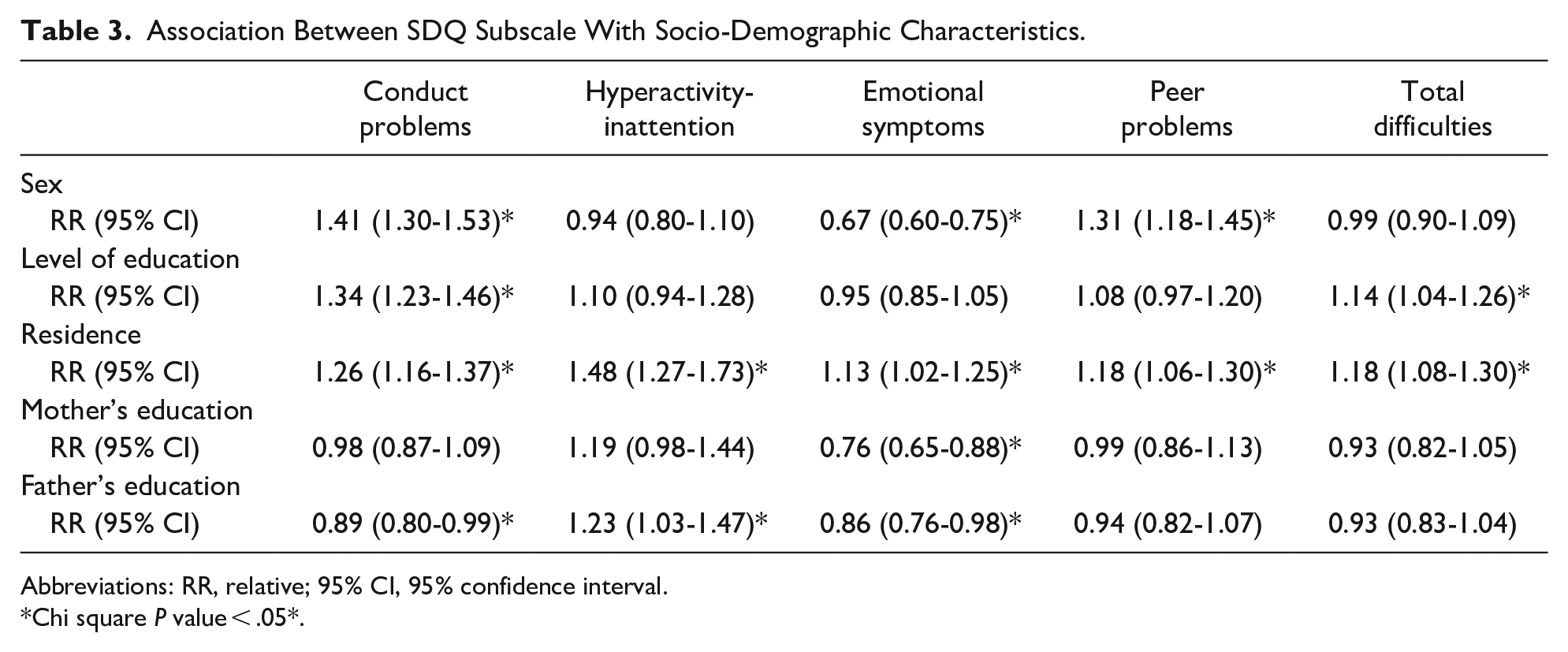
Abbreviations: RR, relative; 95% CI, 95% confidence interval.
Chi square P value < .05*.
Discussion
The prevalence of mental health problems measured on all 4 SDQ scales were lower for this study’s population of 12- to 17-year-old junior and senior high school students from 32 schools across West Java province, Indonesia, than were the prevalence in a study in Tanzania (hyperactivity, 17%; peer problems, 63%; emotional symptoms, 40%; conduct problems, 45%) but higher than prevalence in Vietnam.16,17 Moreover, the overall prevalence of mental health problems among the adolescents in the current study, 31.6%, was lower than that from a previous study in Indonesia (60.17%) that used secondary data from a different questionnaire. 18 However, the prevalence was still higher than the prevalence reported by the WHO, 10% to 20%. Poor mental health among adolescents in low- and middle-income countries continues to be a serious public health issue that needs to be addressed as part of basic development goals.
The prevalence of mental health problems was slightly higher among the female adolescents in this study than was that for the boys, 37.8% versus 37.4%. These results are consistent with previous findings from high-income countries (Australia and the UK) and from 2 other provinces in Indonesia.19-21 In contrast, there were no significant associations between gender and adolescents’ mental health problems in similar research conducted in Egypt, Iran, and Vietnam.6,16,22 The data in Table 3 do show significant associations with gender for conduct problems, peer problems, and emotional symptoms. The co-occurrence rate of conduct disorder itself and depression is much higher than expected by chance, which can be explained by the discovery of the common neural mechanism of behavioral problems and depression, which leads to the observed high comorbidity rate. 23
Puberty affects the development of mental and emotional health problems in both genders, and girls might present with more emotional health symptoms related to the onset of menstruation and the accompanying hormone changes. Differences by gender in mental and emotional health symptoms could also arise because of the different social environment factors the genders face in addition to different biological processes or gene expression mechanisms, and the interactions between biological and environmental factors could also vary by gender.3,16 Female adolescents might be more susceptible to emotional or mental stress related to social pressures around them.2,24 Furthermore, different parenting styles can also cause differences in mental and emotional problems between the genders, especially in terms of behavior control. 25 In terms of differences in actual symptoms, female adolescents often experience internalizing symptoms such as depression, anxiety, withdrawal from social interactions, and somatic complaints, whereas boys show more externalizing behaviors.7,22
This study also revealed more prevalent mental and emotional health problems among the junior high school adolescents than among the high school students, and a study in East Java in Indonesia showed a similar result. 21 The high prevalence of symptoms in the junior high students might reflect the difficulties young teens experience in the transition between elementary and junior high school as well as the general transitions from youth into adolescence and teen years. Junior high school students face changes in teaching methods between elementary and junior high school and in their roles as students in addition to the biological, emotional, and hormonal changes that are occurring at the same time.2,25 In addition, increasing age and personal maturity among adolescents also increase their abilities to adapt to the changes in developmental tasks as well as in the transition from junior to senior high school. 24 Therefore, older adolescents are less likely to experience mental health problems than are the younger age groups.5,6,21
Junior high school students experience more externalizing problems, while high school teenagers begin showing internalizing symptoms; for instance, risk-taking behavior is more prominent in junior high school adolescents while anxiety and depressive emotions are more prominent in high school students.6,20 The findings in Table 3 indicate significant associations between education level and both mental health and conduct problems, in contrast with a study in Nigeria in which there were no significant associations between adolescent education level and any of the SDQ subscales. 26
In comparing prevalence of adolescent mental health problems in rural versus urban communities, the highest prevalence, 47.1%, occurred in a rural district, Majalengka. The findings in this study were similar to earlier findings of significant differences between urban and semi-urban areas in adolescent mental emotional problems in 2 other areas in West Java (Sumedang District and Cirebon City) and in China.7,27 Although one of the factors associated with mental health problems in adolescents is socioeconomic status including place of residence, 4 such problems also occur because of factors such as family and peer relationships and other environmental factors based on location of residence.
Urban and semi-urban or rural areas have different characteristics related to family, peers, and community environments. Urban areas have higher populations, which can increase stress among residents, which in turn can manifest in adolescents as strong emotional reactions including anger, crime, and juvenile delinquency; less-urban areas have lower population densities and residents are less emotional, which creates more peaceful environments. Meanwhile, urban areas have more competitiveness, which can lead to conflict and anger, whereas semi-urban and rural areas uphold mutualism and traditional culture, and this could make teens in these areas more sensitive and emotionally stable.
Teens in urban areas tend to have stronger emotional symptoms, more behavior problems, higher hyperactivity levels, and more problems with peer-to-peer relationships and overall mental health, whereas behavior in semi-urban areas tends to be more pro-social. This more cooperative social environment in semi-urban areas could be a protective factor against mental and emotional problems.7,22,27 The findings from this study, however, contradict prior findings: Here, adolescents who lived in villages in West Java showed higher scores for behavioral and emotional problems than did the adolescents who lived in cities. This is likely related to the disadvantages of living in rural areas such as poverty and poor education opportunities. 7
Another variable in the present study that was associated with adolescents’ mental and emotional health was parents’ highest education levels. The young people in this study whose mothers had low education showed a higher prevalence of abnormal mental health scores, consistent with multiple earlier previous findings of higher SDQ subscale scores among teens with low maternal education levels. 6 Based on this, the study also reported that parents with higher education are more likely to exhibit active parenting behavior, and this association is partly due to their increased ability and knowledge to obtain more resources. 28 Adolescents whose fathers had only completed junior high school showed the highest prevalence in this study of conduct problems, which was consistent with findings from Egypt and China of higher SDQ subscale scores for adolescents with low paternal education levels.6,7 Hu et al 29 also observed this correlation in a study in China, that is, people with high education have better job opportunities than people with low education. In addition, a study in the United States of America (USA) found that compared with high-income families, the hospitalization rate of children with conduct disorders in low-income families is 1.5 times higher. 30
One limitation of this study is that only a few socio-demographic variables were analyzed; other researchers could study additional variables such as ethnicity. However, these findings could adequately generalize to broader populations of Indonesian teens because the study was conducted in the most densely populated area of Indonesia.
Conclusion
This study’s findings demonstrated that among 2 socio-demographic characteristics, residence in an urban or rural area and highest education level completed showed associations with mental and emotional health issues among adolescents in West Java province in Indonesia as measured the scores on the Strengths and Disabilities Questionnaire subscales and the total difficulties scale. Other factors associated with higher prevalence of borderline and abnormal subscale scores were female and junior high versus senior high school student status as well as residence in Majalengka, a rural district, and having a low educated father and mother.
Footnotes
Acknowledgements
The authors thank Dr. Deni Kurniadi Sunjaya, MD, DESS Department of Public Health Universitas Padjadjaran for advice in statistic methodology and Raisa Mentari Moeis, MD for language editing of this manuscript.
Author Contributions
Each author has made substantial contributors to the conception and design of the work; or acquisition, analysis or interpretation of data; or revised it to have approved the submitted version and agreed to be accountable for all aspects of work ensuring integrity and accuracy.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by Academic Leadership grant-in-aid under name Meita Dhamayanti from Universitas Padjadjaran.
Ethic Statement
This study was conducted after an approval is obtained from the Research Ethics Committee Universitas Padjadjaran with a registration number of 244/UN6.C1.3.2/KEPK/PN/2016.