
Abstract
Objective. The perception of emotion and behavior is different between adolescents and their parents. Parent-adolescent agreement on emotional and behavioral problems has not been well researched. The aim of this study was to explore and compare how well the information from themselves matches with the judgments by their parents in terms of emotional and behavioral problems. Methods. The cross-sectional study was conducted using the self-report and parent-report Strengths and Difficulties Questionnaire (SDQ). A total of 1254 Japanese school adolescents aged 12 to 18 and their parents were assessed almost the same time. The results were analyzed using the paired t-test and 2-way analysis of variance for the discrepancies of parent-adolescent agreements in each age and gender groups. Results. Adolescents obtained higher total difficulty and all subscales scores of SDQ than their parents. The effect of grade on the self/parent discrepancy scores were significantly observed on the conduct problems (P < .001), hyperactivity (P = .009), and prosocial behavior (P < .001). The effect of gender was shown significantly on the emotional problems (P < .001), conduct problems (P < .001), and peer problems (P = .002). Conclusion. Adolescents reported more problems than their parents did. For comprehensive evaluation of adolescents’ mental health, it is necessary to draw information from both the adolescents themselves and their parents, and pay attention to the gap between adolescents and their parents’ perception.
Keywords
Introduction
Mental health problems affect 10% to 20% of children and adolescents worldwide,1,2 and recent study indicates that about 10% in Japan among adolescents were affected mental health problems. 3 Therefore, child and adolescent psychiatrists have an important role in treating mental disorder in childhood. In general, child and adolescent psychiatrists usually use questionnaire answered by parents or caregivers to measure mental state of children in the field of child and adolescent psychiatry; however, adolescents sometimes hide the state of mind to their parents. 4 Therefore, questionnaire answered by parents orothers was not always clearly perceived the mental state of their adolescents. For the reason, we usually use questionnaire answered by not only parents but also adolescents themselves. Although using self-report questionnaire to assess adolescent psychopathology is cost-effective and time-saving, perception is subjective, and readily influenced by various factors in informants like adolescents and parents, as well as factors in the illness and the environment. Hence, the discrepancies are seen in the different ratings by different informants.
The Strengths and Difficulties Questionnaire (SDQ) is widely used in community, clinical, and research settings to screen for externalizing and internalizing problems.5-7 SDQ consists of 25 items covering 5 subscales relating to emotional symptoms, conduct problems, peer problems, hyperactivity/inattention, and prosocial behavior. SDQ has been translated into many languages, and exists in 3 versions: parent, teacher, and a self-rating version for older children. The SDQ is not a replacement of the Child Behavior Check List (CBCL), however it has the greater advantage in psychological questionnaire which is shorter and quicker than the CBCL. 8 In previous studies, parent-adolescent agreement between parent-report SDQ and self-report SDQ scales were acceptable in community samples.9,10 However, Li et al 11 reported that parent-adolescent agreements assessed by parent-report and self-report SDQ ranged from low to medium. To date, there are no reports about the agreement between parents and adolescents on emotional and behavioral problems using SDQ in Japanese community adolescents. To examine our hypothesis that the perception of emotional and behavior problems between adolescents and their parents is different and the self/parent discrepancy exist, therefore it is necessary to explore the self/parent discrepancy using the same questionnaire. The aim of this study was to clarify the pattern of parent-adolescent agreements on adolescents’ emotional and behavioral problems among school-aged adolescents in Japan using parent-report SDQ and self-report SDQ.
Methods
Participants and Instruments
Participates were recruited adolescents from the local community who participated in the Toon Child Study, which was designed to review the lifestyle and behavior of adolescents. 12 The Toon Child Study was conducted in 2009 and all junior high school and high school students of Toon city (n = 1878) were involved. The total population of Toon city during that year was approximately 35 000. The average income level in the surveyed area was 4.2 million JPY (equivalent to 40 thousand US dollars), the same as the national average. Questionnaires including the SDQ were provided to the parents or primary caregivers. The response rate of questionnaires was 90.9% in students and 82.5% in parents. Of which, we intended for 1254 adolescents aged 12 to 18 years (males: 635, females: 619) which were able to obtain valid responses from both adolescents and their parents. The participants were divided at each grade in junior high school and in high school.
Measures
The parent-report SDQ was used to assess parents’ perception of their adolescent children’s difficulties and strengths. SDQ includes 25 items scored 0 for “not true,” 1 for “somewhat true,” and 2 for “certainly true.” The scores of emotional symptoms, conduct problems, hyperactivity/inattention, and peer problems can be summed to generate a total difficulty score ranging from 0 to 40. The prosocial scale gives a score for positive prosocial behavior and this sum in not included in the total difficulties score. A higher score indicates more difficulties or strengths.
The self-report SDQ was to assess adolescents’ perception of their own difficulties. The 25 items cover the same attributes as the parent-report SDQ. For most items, the only difference between the parent-rated and self-report SDQ is a grammatical change from third person to first person. The Japanese version of the SDQ was reported with a high homogenous internal consistency (α = .77) and appears to be approximately as reliable as the original English questionnaire. 13 In the present study sample (n = 1254), the Cronbach’s alpha coefficients for self-report SDQ was .665, parent-report SDQ was .679.
Statistical Analysis
Each score is expressed as a mean and standard deviation (SD). All statistical analyzes were divided by grade and gender. The reason is that emotional and behavioral problems of adolescents change with age and are different among male and female. Scores of self-report SDQ and parent-report SDQ were compared by the paired t-test. To measure the self/parent discrepancies, we subtracted self-report SDQ scores from parent-report SDQ for total and subscale scores. Higher scores in the absolute values indicated more discrepancies between adolescents and their parents. Next, 2-way analysis of variance (ANOVA) was used to compare the discrepancies with regard to each gender and grade. All statistical analyses were conducted using the Statistical Package for Social Sciences (SPSS) version 22 for Windows. The significance level was set at P < .05, and all P were 2-tailed.
Ethics
This study was approved by the Institutional Review Board of Ehime University Graduate School of Medicine (IRB No. 0909008). Questionnaires were provided to the adolescents and their parents or primary caregivers, together with written information about the project. Participants were informed that they could freely choose whether or not to participate in this study and were reassured that their choice would not affect their school life in any way. A signed informed consent and participants assent were obtained from the adolescents/parents of each participant.
Result
Tables 1 and 2 show the mean of total and subscale scores of SDQ in male and female adolescents and to compare each score between adolescents and their parents. The mean scores of total difficulties assessed by self-report SDQ were significantly higher than the score of parent-report SDQ in both genders. Further, subscale scores of self-report SDQ were significantly higher in the all subscales except for prosocial behavior score than the scores of parent-report SDQ in both genders and all grades from the first grade of junior high school to the third grade of high school. In terms of prosocial behavior, the score of only the first grade and the third grades of high school male adolescents were significantly lower than those of parents. In female, the scores of the first, second, and third scores of high school adolescents were significantly lower than those of parents.
Chronological Distribution of Self-Report and Parent-Report SDQ Scores in Male (Age Range 12-18 years).
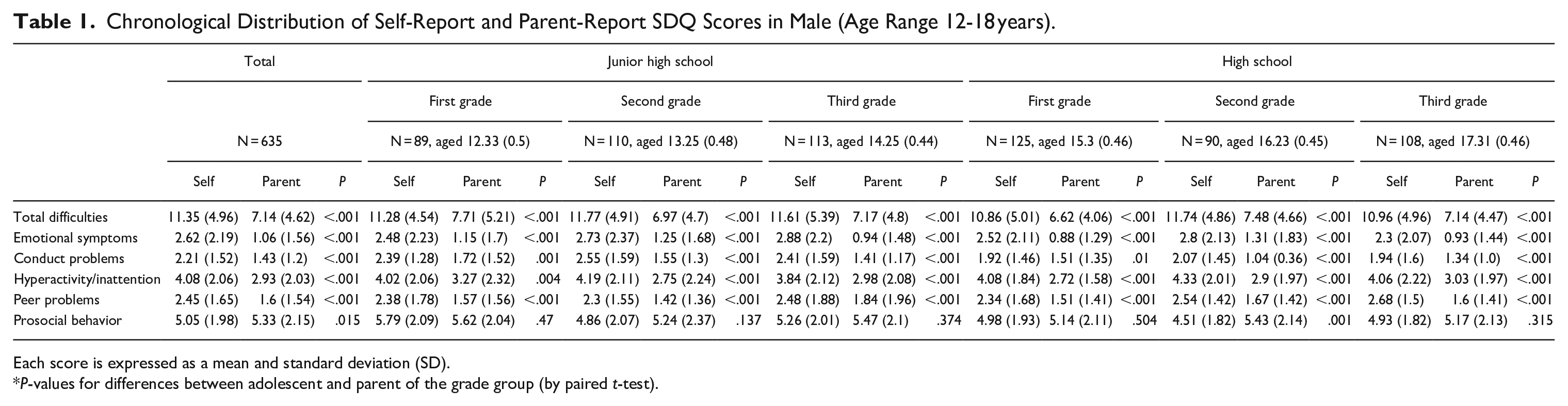
Each score is expressed as a mean and standard deviation (SD).
P-values for differences between adolescent and parent of the grade group (by paired t-test).
Chronological Distribution of Self-Report and Parent-Report SDQ in Female (Age Range 12-18 years).

Each score is expressed as a mean and standard deviation (SD).
P-values for differences between adolescent and parent of the grade group (by paired t-test).
The self/parent discrepancy scores in gender and grades and interaction of gender × grades were analyzed with the 2-way ANOVA (Table 3). There were no effects of interaction of gender and grade (age) at total difficulty score and each subscale score.
The Self/Parent Discrepancies of SDQ Scores with Regard to Each Gender and Grade.
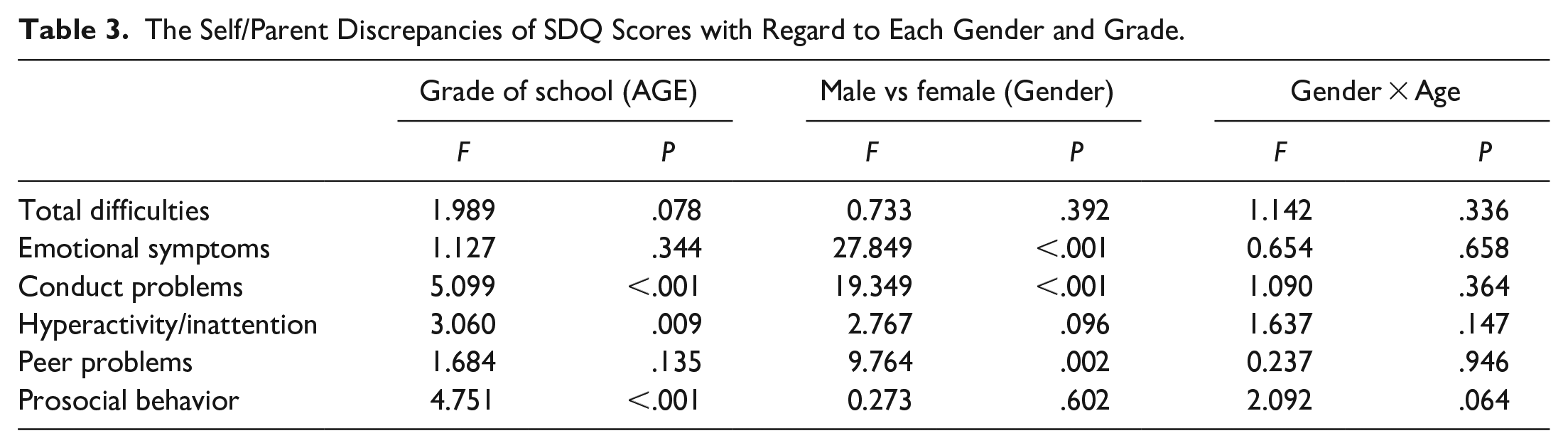
In terms of effect of grade on the self/parent discrepancy scores, there were significant differences on the conduct problems (P < .001), hyperactivity/inattention (P = .009), and prosocial behavior (P < .001). The self/parent discrepancy scores on the conduct problems were 0.55 (1.56) in junior high school and 0.59 (1.75) in high school, on the hyperactivity/inattention were 1.37 (2.12) in junior high school and 1.10 (2.34) in high school, and prosocial behavior were—0.48 (2.33) in junior high school and—0.12 (2.42) in high school both gender. In terms of effect of gender on the self/parent discrepancy scores, the results showed that a significant self/parent discrepancy scores in the effect of gender on the emotional symptoms (P < .001), conduct problems (P < .001), and peer problems (P = .002). These results indicate that females rated higher discrepancy scores on the emotional symptoms than males, on the other hand, in conduct problems, males rated higher discrepancy scores than females. Moreover, males of discrepancy score were significantly higher scores in the subscale of peer problems.
Discussion
This study estimated the parent-adolescent agreements and self/parent discrepancy on emotional and behavioral problems among Japanese adolescents aged 12 to 18 years using SDQ. The present study identified the higher almost subscales of SDQ evaluated by adolescents themselves compared to SDQ scores evaluated by parents. Previous studies reported that there was significant difference between the scores of self-report SDQ and parent-report SDQ in children with sensory organ problems.14,15 Parents who have adolescents with vocal problems reported more peer relationship problems of SDQ than their adolescents themselves aged 11 to 18 years. 14 Anmyr et al 15 reported that children aged 9 to 15 years with cochlear implants have greater total difficulties, emotional symptoms, and conduct problems according to the self-report SDQ than parent-report SDQ. Although there are few reports about the agreement between parents and adolescents in community-based study, there was a high correlation between self- and parent-reports.16,17 Wang et al 17 reported that the score of Youth Self-Report on emotional and behavioral problems were higher than those of parent-report CBCL, and factors that increased informant discrepancies on emotion and behavioral problems were boys and older age among Chinese community adolescents aged 11 to 18 years.
This study also demonstrated the comparison of the self/parent discrepancies by gender and grade. Female students had significantly higher self/parent discrepancy score of emotional symptoms than male students. Adolescents may be more sensitive to minor disturbances and report them even if those disturbances are less visible for their parents; therefore, the discrepancy of self/parent perception on emotional problems increased. The present study might show that reports from parents are not adequate for the evaluation of mental state of adolescents, especially internalizing problems such as emotional problems. The self/parent discrepancies of conduct problems were associated with both grades and genders. Delinquency, defined as conduct that is out of accord with accepted behavior, was more common in early adolescence (age 12) among males than females, 18 and male adolescents tend to hide their problems of behavior for their parents rather than females. The self/parent discrepancy of hyperactivity/inattention was associated with grades. The symptom severity of Attention-deficit hyperactivity disorder (ADHD) has been reported to decline with aging.19,20 In terms of peer problems, male discrepancy scores were significantly higher than female scores. Sensitivity to peer stress in boys may be more reflected outward-directed behaviors such as conduct problems and peer problems, whereas in girls may be reflected in inward emotional responses. 21 In prosocial behavior, the self/parent discrepancy of prosocial problems was associated with grades. The score of prosocial behaviors in parents were higher than that of adolescents. This result suggested that parents might overestimate their daughters’ or sons’ prosocial behavior. The self/parent discrepancies could show the characteristics of adolescents in detail. Theunissen et al 22 reported that the SDQ parent-form could provide additional information about externalizing problems, including conduct problems and hyperactivity/inattention in adolescents by comparison with the self-report. In clinical settings, some various questionnaires or rating scales will be useful to investigate mental problems for adolescents; however clinical interviews to adolescents, parents, and additionally teachers should be given for primary consideration. In the community, gap between self- and parent perception should be addressed.
The present study has several limitations. First, study participants were recruited from public junior and high schools in rural areas. Although some participants in high schools lived in suburban or urban area, our findings may not be generalizable to the entire Japanese adolescent population. Second, with regard to the internal consistency of the instrument, the Cronbach α values for the SDQ was at a moderate level.
In conclusion, adolescents reported more problems than their parents did. Adolescents with mental health problems are likely to according to be multifactorial factors such as their daily life, psychiatric problems, family, and school. For comprehensive evaluation of adolescents’ mental health, it is necessary to draw information from both the adolescents themselves and their parents, additionally from their teachers.
Footnotes
Author Contributions
FH conceived the original idea of the study, and design the study. KN and RH performed the data analysis. KK drafted and wrote the manuscript. HU supervised to the statistical analysis and interpretation. YO and SU supervised to study design, and revision of the manuscript. All authors contributed to the final manuscript, and agreed to the publication of the article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.