
Abstract
Background. Inappropriate complementary feeding practices are amongst the key causes of child undernutrition. It rises the risk of undernutrition, illness, and mortality among children. Objectives. This study was aimed to determine the pooled prevalence of MMF practice and associated factors among children aged 6 to 23 months in Ethiopia. Methods. The search was conducted by using the following electronic databases; PubMed/MEDLINE, HINARI, EMBASE, Google Scholar, Web of Science, Scopus, African journals, and Google for grey literature. The publication bias was determined by using a funnel plot and Egger’s test. The heterogeneity between the studies was checked by using I2 statistic. The subgroup analysis was done by sample size, region, and year of publication. Result. A total of 20 studies with 12 656 study participants were included in the present systematic review and meta-analysis. The pooled prevalence of MMF practice among children aged 6 to 23 months in Ethiopia was estimated to be 63.80% (95%CI: 56.59, 71.01). PNC visit (AOR = 1.90, 95%CI [1.31, 2.49]), wealth index (AOR = 2.11, 95%CI [1.42, 2.81]) and age of child (AOR = 5.75, 95%CI [4.25, 7.26]) were factors significantly associated with MMF among children aged 6 to 23 months. Conclusion. The findings showed that the pooled prevalence of MMF among children aged 6 to 23 months in Ethiopia was relatively low. PNC visit, wealth index and age of child were factors significantly associated with MMF among children aged 6 to 23 months. Therefore, community-based health education concerning the recommended MMF among children aged 6 to 23 months is required to take place.
Background
A suitable nutrition is crucial for health and development of the children. 1 MMF is a proportion of breastfed and non-breastfed among children 6 to 23 months of age who receive solid, semi-solid, or soft foods but also comprising milk feeds for non-breastfed children the minimum number of times or more. 2 The homemade complementary foods are principally based on cereals and legumes in Ethiopia. The consumption of micronutrients like iron, zinc, and calcium from homemade complementary foods was very low. 3 However, appropriate complementary feeding practice is vital for the growth and development of the children. 4 The indicators which reflects diet quality for young children are required for programs and in some research contexts. 5
Starting from 6 months of age, infants, and young children are at an augmented risk of malnutrition. 6 Six to twenty-four months of age is the period of most serious time for the development of the infant. 7 Whereas, a time from birth to 2 years of age would provide a chance for the promotion of health, growth, and behavioral development of children. 8 Furthermore, women of child-bearing age, infants and young children are the principally nutritional susceptible periods of the life cycle. 9 Maternal and child undernutrition is vastly widespread in low-and middle-income countries leading in the considerable rises in mortality and overall disease burden. 10
Directly or indirectly, undernutrition is accounted for around 35% of deaths in children less than 5 years of age worldwide. It is also a principal cause of disability in children. 1 Unsuitable complementary feeding in infants and children may rise the risk of undernutrition, illness and mortality. 11 Even the suboptimal complementary feeding practices found to lead to a quick rise in the magnitude of stunting in young children from 6 months age. 12 This is because of that suboptimal feeding practices were found to be associated with malnutrition. 13 Besides, inappropriate duration of announcing complementary food would deprive the infant for optimum nutrition. Whereas, this would cause for undernutrition, and augmented morbidity and mortality. 14 It is the main challenge to attain an optimum Infant and young child feeding practices in developing and developed countries. Inappropriate infant and young child feeding practices attributed to about 40% deaths of under 2 years age worldwide. 15
In developing countries, about 19.4% of children <5 years of age were underweight and 29.9% were stunted in the year 2011. Undernutrition leads to around one third of deaths in children <5 years of age. 7 Whereas, a report of World Health Organization 1 showed that about 32% (186 million) of children under 5 years of age were stunted and 10% (55 million) were wasted in developing countries. Malnutrition is a main community health problem in developing countries. If household food insecurity is combined with poor child feeding patterns, it would lead to malnutrition. 8 In Ethiopia, the poor nutritional status of children and women has been a critical problem for numerous years. 16 To improve infant and young child feeding, designing of the effective programmes that consider the understanding of the local condition and an efficient process for prioritizing interventions are required. 12
Undernutrition remains the public critical issues. So that, the present meta-analysis could be significant in providing the essential information. This is because gaining the evidence for the MMF and associated factors among children aged 6 to 23 months in Ethiopia could encourage the healthcare providers, stakeholders, policy makers and implementers, nutritionist and government to focus on the nutritional status of the children. Further, they could develop different strategies to prevent the morbidity and mortality associated with the inappropriate feeding practice of the children based on this evidence.
Review Questions
What is the pooled prevalence of MMF practice among children aged 6 to 23 months in Ethiopia?
What are the factors associated with the MMF practice among children aged 6 to 23 months in Ethiopia?
Methods
Study Setting
The present study was conducted in Ethiopia. Ethiopia is found in the Horn of Africa with a total area of 1 100 000 km2. In the world, it is the 13th most populous country, whereas, the 2nd most populous in Africa. The national capital and largest city is called Addis Ababa. 17
Search Strategies
The search was conducted by the using the following electronic databases; PubMed/MEDLINE, HINARI, EMBASE, Google Scholar, Web of Science, Scopus, African journals, and Google for grey literature. Overall, all electronic search methods were used to find the relevant studies accordingly. The search was done by using the following keywords; “Acceptable diet,” “complementary feeding,” “Minimum Meal Frequency,” “Associated Factors,” “determinant factors,” “Factors,” “Children 6 to 23 months,” and “Ethiopia.” During this, “AND” and “OR” Boolean operators were employed to integrate the keywords.
Eligibility Criteria
Inclusion Criteria
Exclusion Criteria
Articles with poor quality and articles in which the outcome variable was not clearly defined and measured were excluded from the meta-analysis.
Outcome of Interest
In the present systematic review and meta-analysis, primary outcome was the prevalence of MMF practice among children aged 6 to 23 months, which was reported within the original articles. Likewise, the secondary outcome was factors associated with the MMF practice among children aged 6 to 23 months which was reported within the original studies.
Data Extraction
All studies obtained from all databases were exported to Endnote version 8 software and the duplicates were removed. Finally, all studies were exported to Microsoft Excel spreadsheet. The Titles and abstracts of studies retrieved using the search strategy and those from additional sources were screened to identify studies that satisfy the inclusion criteria. Then studies that satisfy the inclusion criteria by title or abstract screening were undergo full text review for eligibility and data extraction. The Preferred Reporting Item for Systematic Review and Meta-Analyses (PRISMA) flowchart was used for the stepwise inclusion and exclusion of the articles. The first author, publication year, regions, study area, sample size, prevalence and 95%CI for factors were included in to the data extraction format.
Quality Assessment
The Newcastle–Ottawa Scale (NOS) quality assessment criteria were used to include the studies. The quality of each study was assessed by using modified NOS for cross-sectional studies. It has 10 points in 3 domains of modified NOS components for observational studies. So that, the studies which were scored ≥5 out of 10 points were included in the final analysis. 18
Data Processing and Analysis
Random effect model was employed to estimate the pooled prevalence of MMF practice among children aged 6 to 23 months. The analysis was conducted by using STATA version 11 statistical software after extraction of the articles in Microsoft Excel spreadsheet format were completed. The heterogeneity among the included studies was assessed by using Cochrane Q-test and I 2 statistics. The publication bias was measured by using Egger’s test. Subgroup analysis was done based on the region, category of publication year and sample size category. Finally, the forest plot format was used to display the pooled prevalence with 95%Cl.
Reporting the Results
In the present systematic review and meta-analysis, the results were reported based on the PRISMA 2009 checklist. 19 Furthermore, tables, figures and narrative summaries were used to report the findings.
Result
A total of 643 articles were identified through the search strategies. They were retrieved from PubMed/MEDLINE, HINARI, EMBASE, Google Scholar, Web of Science, Scopus, African journals, and Google for grey literature. Out of 643, 336 articles were excluded due to duplication. Of the remaining 307 articles, 281 articles were excluded after reviewing of the titles and abstracts because of they were not related. Then, 26 full-text articles were assessed for eligibility based on the pre-setted criteria and 6 articles were excluded with a reason. Lastly, 20 articles were met the eligibility criteria and included in to the meta-analysis (Figure 1).

PRISMA flowchart diagram of the study selection for systematic review and meta-analysis on the prevalence of MMF practice and its associated factors among children aged 6 to 23 months in Ethiopia.
Features of the Included Studies
Among the studies published up to April 18/2021 in Ethiopia, 20 studies were included into the present systematic review and meta-analysis. The study design of all these studies were a cross-sectional. The smallest sample size was 200, while the largest was 1034. The smallest prevalence of MMF practice among children aged 6 to 23 months in Ethiopia was 33%, while the largest was 94.5%. Further, 12 656 study participants were involved to determine the pooled prevalence of MMF practice among children aged 6 to 23 months in Ethiopia (Table 1).
Characteristics of the Studies Included in the Systematic Review and Meta-Analysis on the Prevalence of MMF Practice and Its Associated Factors among Children Aged 6 to 23 Months in Ethiopia.

Heterogeneity and Publication Bias
The heterogeneity and publication bias of the studies included in the meta-analysis were assessed. After doing this, the result indicated that there is a significant heterogeneity among studies (I2 = 98.9%, P = .000). The publication bias was determined by using Egger’s tests. According to the result, it was not statistically significant (P = .077). Besides, the funnel plot shows the symmetrical distribution of the included articles, this suggests there is no evidence for publication bias for this meta-analysis (Figure 2).

Funnel plot with 95% confidence limits of the pooled prevalence of MMF practice among children aged 6 to 23 Months in Ethiopia.
Sensitivity Analysis
Sensitivity analyses using the random effects model revealed that no single study influenced the overall prevalence of MMF practice among children aged 6 to 23 months (Figure 3).

The result of sensitivity analysis of 20 studies conducted on MMF practice among children aged 6 to 23 months in Ethiopia.
Prevalence of Minimum Meal Frequency
This meta-analysis was used the random effect model to estimate the pooled prevalence of MMF practice among children aged 6 to 23 months in Ethiopia, which was 63.80% (95%CI: 56.59, 71.01). The level of heterogeneity was (I2 = 98.9%: P = .000) (Figure 4).

Forest plot of pooled prevalence of MMF practice among children aged 6 to 23 months in Ethiopia.
Subgroup Analysis
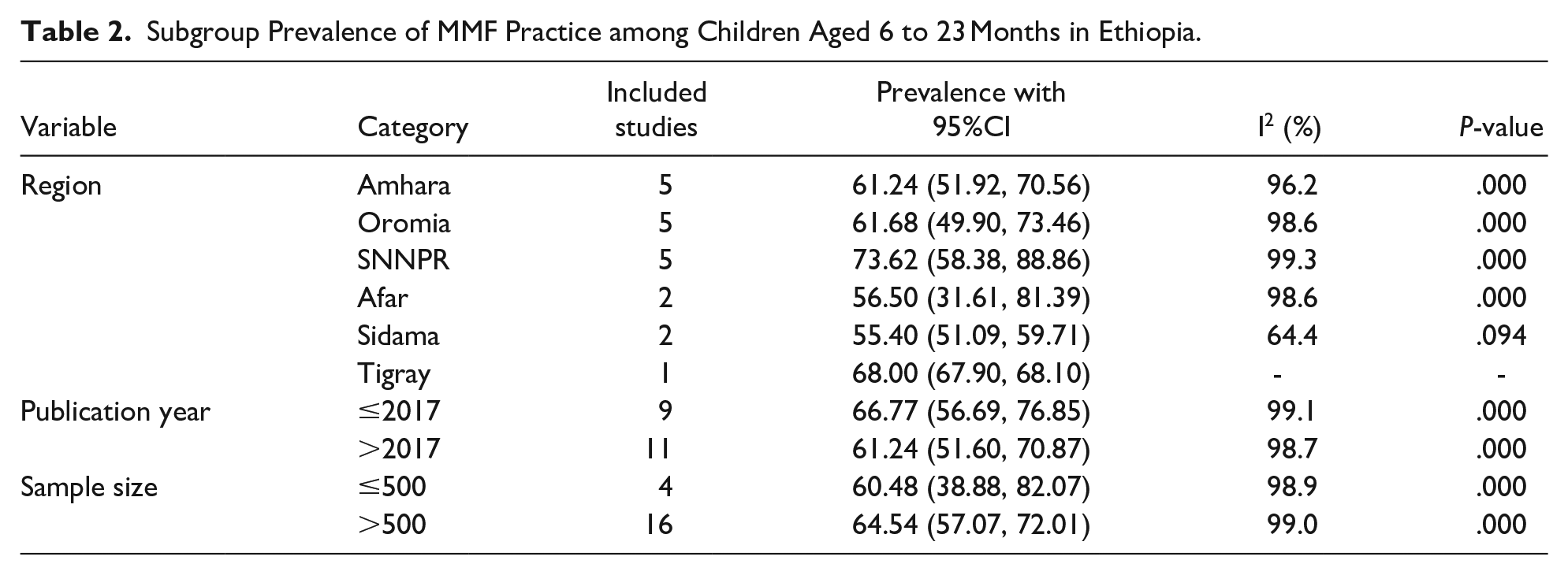
Due to the presence of a significant level of heterogeneity among the included studies, subgroup analysis was required to be conducted. During this, sub-group analysis was deployed using region, publication year, and sample size to determine the pooled prevalence of MMF practice to identify the sources of heterogeneity. Accordingly, the pooled prevalence of MMF practice was 61.24% in Amhara region, 61.68% in Oromia region, 73.62% in SNNPR, 56.50% in Afar region, and 55.40% in Sidama region. Whereas, 60.48% for sample size ≤500 and 64.54 for sample size >500. Furthermore, it was 66.77 for studies published ≤2017 year and 61.24% for the studies published after 2017 year (Table 2).
Subgroup Prevalence of MMF Practice among Children Aged 6 to 23 Months in Ethiopia.
Associated Factors
According to the present meta-analysis, postnatal care (PNC) visit, wealth index and the age of children were factors significantly associated with MMF practice among children aged 6 to 23 months in Ethiopia.
PNC Visit
Based on the pooled effects of 2 cross-sectional studies,25,28 mothers who had PNC visit were 1.90 times more likely to provide the recommended MMF for children aged 6 to 23 months (AOR = 1.90, 95%CI [1.31, 2.49], I2 = 0.0%, P = .596) than mothers who had no PNC visits (Figure 5).

The overall pooled odds ratio of the association between PNC visit and the MMF practice among children aged 6 to 23 months in Ethiopia.
Wealth Index
Based on the pooled effects of 2 cross-sectional studies,25,32 rich family were 2.11 times more likely to provide the recommended MMF for children aged 6 to 23 months than poor family (AOR = 2.11, 95%CI [1.42, 2.81], I2 = 0.0%, P = .493) (Figure 6).

The overall pooled odds ratio of the association between wealth index and the MMF practice among children aged 6 to 23 months in Ethiopia.
Age of Child
Based on the pooled effects of the 3 cross-sectional studies,20,25,28 children aged 18 to 23 months were 5.75 more likely to receive the recommended MMF than children aged 6 to 11 months (AOR = 5.75, 95%CI [4.25, 7.26], I2 = 25.5%, P = .261) (Figure 7).

The overall pooled odds ratio of the association between age of child and the MMF practice among children aged 6 to 23 months in Ethiopia.
Discussion
Among children <2 years of age, inappropriate feeding practice rises the risk of undernutrition, illness, and mortality. Understanding the level of MMF practice among children aged 6 to 23 months in Ethiopia would help in policy making and implementing, developing the significant strategies to prevent undernutrition and the associated morbidity and mortality among these children. So that, the present systematic review and meta-analysis was aimed to determine the pooled prevalence of MMF practice and associated factors among children aged 6 to 23 months in Ethiopia. Finally, the present systematic review and meta-analysis revealed that the pooled prevalence of MMF practice among children aged 6 to 23 months in Ethiopia was estimated to be 63.80% (95%CI: 56.59, 71.01).
This finding was lower when compared with the study conducted in China (75.1%), 40 Tanzania (82%), 41 Rwanda (83%), 42 Benin (75.4%), 43 Pakistan (84.7%), 44 Mongolia (92.1%), 45 Nepal (76.6%), 46 Sri Lanka (88%), 47 Bangladesh (81.06%), 48 Mosul city (79.1%) 49 and Kenya (88.3%). 50 The variation might be due to the difference in the tools used, awareness of undernutrition-related morbidity and mortality, sociodemographic characteristics of the study population and child nutritional management policy. Furthermore, active involvement of stakeholders, health professionals, and the government on the child nutrition could bring the variation. This finding was consistent with the study conducted in Ghana (57.3%). 51 However, this finding was higher than the study conducted in metropolitan city (52%), 52 Nigeria (33.6%), 53 India (41.5%), 54 Burkina Faso (24.37%), 55 Uttar Pradesh (50.9%), 56 Iran (42.7%), 57 Indonesia (53.0%). 58 The possible justification could be that the difference in the sociodemographic characteristics of the study population.
The subgroup analysis in the present systematic review and meta-analysis showed that the pooled prevalence of MMF practice was lowest in Sidama region 55.40% (95%CI: 51.09, 59.71) and highest in SNNPR region 73.62% (95%CI: 58.38, 88.86). It was lower for sample size ≤500 60.48% (95%CI: 38.88, 82.07) and higher for the sample size >500 64.54% (95% CI: 57.07, 72.01). Furthermore, it was higher for the studies published ≤2017 year 66.77% (95%CI: 56.69, 76.85) and lower for the studies published after 2017 year 61.24% (95% CI: 51.60, 70.87).
The present systematic review and meta-analysis revealed that mothers who had PNC visit was 1.90 times more likely to provide the recommended MMF for children aged 6 to 23 months (AOR = 1.90, 95%CI [1.31, 2.49]) than mothers who had no PNC visits. In fact, during the PNC visit, the mother would be advised by the health profession on duty about her child nutrition, telling her that the inappropriate child feeding would lead to the morbidity and mortality. This would improve the knowledge of the mother concerning to her child nutrition. Knowing this, the mother would provide the meal as per recommendation.
The rich family was 2.11 times more likely to provide the recommended MMF for children aged 6 to 23 months than poor family (AOR = 2.11, 95%CI [1.42, 2.81]). This was supported by the conducted in India. 54 The possible justification could be that since there is no problem with the availability of the food, the mother would provide the meal to her child. Even if she is not fully aware about the recommended MMF, there could be the chance of giving the food to her child because of the accessibility of the food. Likewise, children aged 18 to 23 months were 5.75 more likely to receive the recommended MMF than children aged 6 to 11 months (AOR = 5.75, 95%CI [4.25, 7.26]). This was supported by the study conducted in Bangladesh, Indonesia and Malawi.48,58,59 This was also supported by the study conducted in Ghana, the increase in the child’s age (18-23 months) was positively associated (β = 1.387, P < .01) with achieving the needed MMF. 60
Conclusion
The present systematic review and meta-analysis showed that the pooled prevalence of MMF among children aged 6 to 23 months in Ethiopia was relatively low. PNC visit, wealth index and age of child were factors significantly associated with MMF among children aged 6 to 23 months. These findings could encourage the healthcare providers, stakeholders, policy makers and implementers, nutritionist, and government to focus on the nutritional status of the children. Further, they could develop different strategies to prevent the morbidity and mortality associated with the inappropriate feeding practice of the children based on this evidence. Finally, based on these findings, the author recommends that community-based health education concerning the recommended MMF among children aged 6 to 23 months is required to take place.
Limitation of the Study
The present meta-analysis was not accomplished without the limitations. It was difficult to consider some of the associated factors with MMF among children aged 6 to 23 months because of they were not measured consistently across various studies. Therefore, these should be considered in the future studies. Besides, future studies are needed to be conducted to identify factors associated with MMF among children aged 6 to 23 months.
Footnotes
Author Contributions
Addisu Dabi Wake contributed to the conception of the study, data analysis, drafting or revising the article, gave final approval of the version to be published, and agrees to be accountable for all aspects of the work.
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.
Data Sharing Statement
The data used to support the findings of this study are on the hands of the corresponding author.