
Abstract
Health literacy is a critically important determinant of health and is influenced by access to supportive social networks and services. Global investment in education throughout the life course is required to support health literacy development. The aim of this review is to characterize the role, responsibilities, and the optimal setting for the emergent role of a Health Literacy Mediator (HLM). A scoping review of recent literature was conducted. The review revealed a lack of consensus on who should be teaching health literacy, and variability in confidence when teaching health literacy. Professionals reported facing barriers such as a lack of time, a lack of knowledge, and recognized that the health literacy needs of children worldwide are not being met. Further research into the role of HLM is required to determine who is best suited to this role and what their responsibilities will be to ensure consistent health literacy education.
Introduction
Health is a critically important international priority 1 and has been recognized in the Shanghai Declaration as a key sustainable development goal in the 21st century. 2 Health literacy (HL) helps to promote this goal, as it supports positive, active, and autonomous health decisions. 3 This will be essential to reduce the global impact of communicable and non-communicable diseases. The Shanghai Declaration refers to HL as a critical determinant of health and urged global investment to enhance HL throughout the life-course and in all educational settings. 2 HL, which can be a product of health education and health promotion, has recently been defined as a social determinant in its own right. 4 The social determinants of health (SDH) are “the conditions in which people are born, grow, live, work, and age.” 5 They include a range of factors that influence health, many of which the individual has limited control over; for example, agriculture and food production.5,6 However, some factors are modifiable, such as HL.
The definition of health literacy has evolved over time. Bröder and Carvalho 7 provide a useful definition for children and young people, explaining it as “a social and relational construct that encompasses how health-related, multimodal information from various sources is accessed, understood, appraised, and communicated and used to inform decision-making in different situations in health (care) settings and contexts of everyday life, while taking into account social, cognitive, and legal dependence.” This recognizes that HL is contextually dependent and that it should be referred to as a complex relationship between the individual, the community, and the health services they seek to access rather than an individual attribute. 8 By increasing the HL of an individual, one may also increase the HL of those around them and vice versa. This phenomenon is referred to distributed health literacy (DHL). 9 Edwards et al 9 describe DHL as the mediation of the development and practice of HL between families, friends, and communities by sharing knowledge, facilitating learning, contributing their own skills, and supporting decision making. Therefore, children’s HL can be promoted or hindered by social structures, relationships, and societal demands. 7 This description highlights the importance of creating systems around children that develop and encourage HL, and schools provide an important setting to achieve this aim. 10
Education is another important SDH. Education can be used as a tool to help support individuals to develop the assets they need to make informed health decisions and navigate the health care system. 11 Education can occur in formal (eg, school) or informal (eg, home) settings and a range of professionals have a responsibility to educate children and youth. For example, health education is outlined in both teacher and nurse competency standards in Australia.12,13 This inclusion emphasizes that HL education should not be the sole responsibility of 1 professional group, but rather a collective effort. The Australian Quality and Safety Commission has called for a collaborative effort in addressing HL in today’s society. This would include embedding HL into systems and policies on an organizational level, ensuring open and effective communication between all involved parties, and integrating HL into education. 14 This is consistent with the recommendation made in the Marmot 15 Review that a whole-of-system approach to supporting primary health interventions is necessary.
One way to overcome health inequities, enhance collaboration of healthcare professionals, educators, and families, and drive HL education could be to introduce a new position in the form of a Health Literacy Mediator (HLM) within communities. This is an emergent role, and no definition could be located in the scholarly or gray literature. Using existing definitions for health education, 16 health promotion, 17 and health literate organisations 18 as a guide, we formed the following definition of a HLM: “A person or group of people dedicated to providing learning experiences and opportunities to enable individuals and communities to overcome inequities perpetuated by their social determinants and increase their HL assets to improve their health outcomes.” This definition allows researchers to compare existing HL interventions and identify HLM that are already practising within communities. At present, Patient Navigators and/or Health Coaches are existing roles in United States of America, United Kingdom, China, and Australia. These roles help to facilitate and support a patient’s journey through the healthcare system, seeking to empower patients to respond to the health challenges specific to them.19-22 A HLM is imagined to be more all-encompassing than these current roles and to have a stronger focus on capacity building everyone, not just those accessing health services. Having a HLM in the community could contribute to helping people to keep well and out of hospitals.
The HL needs of children and youth worldwide are not being adequately addressed.15,23 Despite health education efforts that emphasize HL, limited research has addressed the effects of HL interventions within specific settings, for examples within school or community sites. 24 As there are currently no defined roles for a HLM the question arises, how would a HLM look and work in practice? This is the topic of discussion for the present scoping review. Given the new and explorative nature of this topic, we proposed the following questions to guide data collection: (1) What are the roles, responsibilities, and the optimal setting for a HLM? (2) Can a HLM have an impact on redressing the health inequities in communities?
Method
A systematic scoping review methodology was considered appropriate given that the topic is broad, and there is lack of general consensus on how the phenomenon of interest is characterized. 25 Systematic scoping reviews aim to explore how a topic has been studied or approached in the current literature, making them distinct from systematic reviews. 26 This review was conducted in alignment with the Joanna Briggs Institute reviewers’ manual, the Preferred Reporting Items for Systematic reviews and Meta-Analyses extension for Scoping Reviews (PRISMA-ScR) checklist, and Arksey and O’Malley’s 26 methodological framework.27,28
A combination of the Population, Concept and Context (PCC), and the Population, Intervention, Context, Outcome (PICO) was used to identify keywords (Table 1), which were refined in consultation with the research team (MS, NK, VC and RN) and a specialist research librarian. The intervention was defined as a person or group of people fulfilling the role of a HLM, the concept was HL, the population was children and young people (0-18 years of age), the context was the location where the intervention was taking place, and the outcome was how HL had been changed.
Summary of Search Terms.

All studies included were identified using a comprehensive and systematic search of the literature. This took place between 10th September 2020 and 28th October 2020. The 3-stage approach outlined by the JBI for scoping reviews was adopted. 28
Stage 1: Pilot search and screening was carried out in a single database (CINAHL Complete) which led to refinement of search terms, search strategy, and finalization of the inclusion and exclusion criteria (Table 2).
Stage 2: The final search was conducted in 7 databases: CINAHL Complete, Education Source, Emcare, ERIC, PsycINFO, Web of Science, and PubMed via Ovid. For each database, specific terms (for example, ways to link search terms) were used when relevant and supplemented by Boolean operators “OR” and “AND,” keyword searching of the concept terms, synonyms, and plurals.
Stage 3: The last step in the literature search involved screening the reference lists of the retrieved articles to cross-reference results and ensure relevant articles were not missed in the final search.
Inclusion and Exclusion Criteria for Scoping Review.
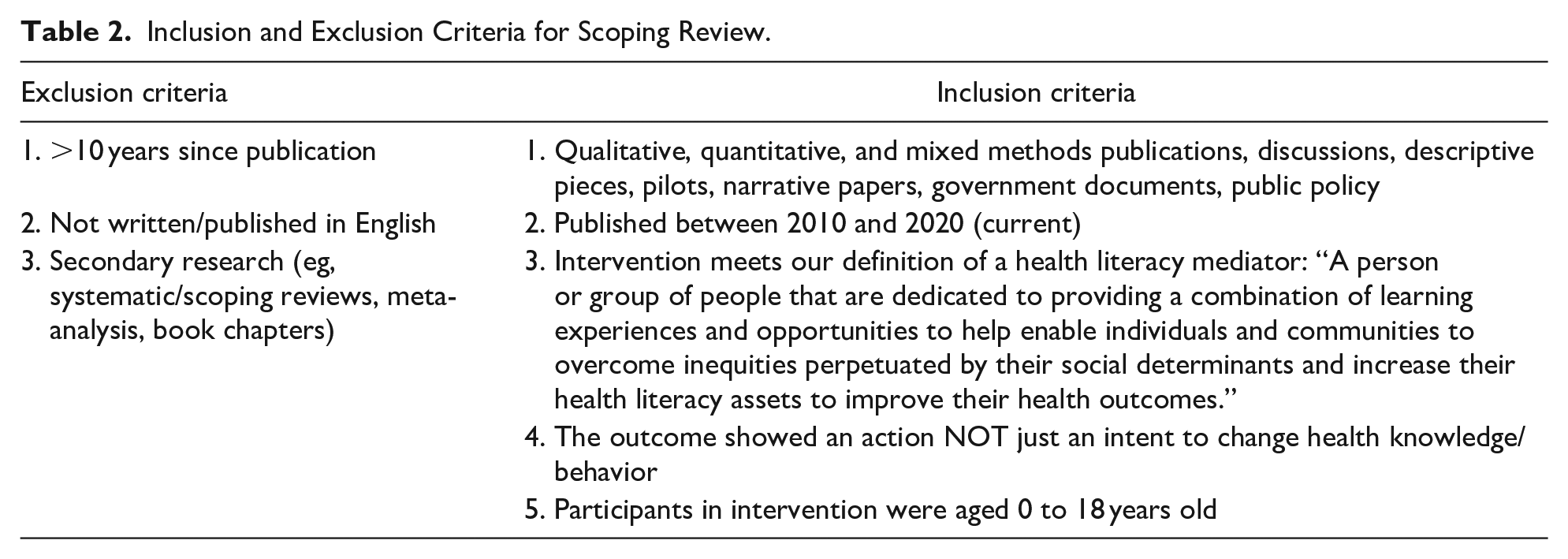
Published peer reviewed literature with a focus on health topics, behaviors or knowledge with a specific focus on action (not self-reported intent to change) were considered for inclusion. Only primary research articles were included in the review. Searches were limited to the years 2010 to 2020 for recency, and to the English language because of practical constraints.
Charting the data refers to the process of data extraction used by the JBI for scoping reviews. 28 The citations from all retrieved articles were exported into EndNote X9, where they were organized, and duplicates were removed (Figure 1). All articles were then screened at a title and abstract level against the inclusion and exclusion criteria by 1 reviewer (MS) and sorted into 3 categories: “yes,” “no,” and “maybe.” A second screening of the articles from both the “yes” and “maybe” categories was conducted by 2 reviewers from the research team (MS and RN) using Covidence software. A PRISMA-ScR chart outlining the search process for the scoping review and the results of the search was created. 27 Relevant data from the final articles were extracted and summarized under categories as devised by the research team. The research question and sub question guided the development of the data extraction categories. Tables were developed to thematically organize data from the final articles so that results could be reported succinctly and logically. The final articles did not undergo a critical appraisal process to review the risk of bias in studies, heterogeneity, and publication bias, as this is not an integral requirement for a scoping review.25,26,28

PRISMA flow chart. Search process and results from databases: CINAHL, Education Source, Emcare, ERIC, PsycINFO, PubMed, and Web of Science.
Ethical Approval and Informed Consent
Ethics approval and informed consent were not required for this scoping review of the international literature.
Results
The search yielded 5902 articles from 7 databases (Figure 1). Once the inclusion and exclusion criteria were applied at title and abstract level, 41 articles remained for full text screening. The independent review process used Covidence software, which identified 14 conflicts between the research team members. These were discussed in detail until consensus was achieved. The final 29 articles that met the study criteria were reviewed and the key information was extracted (see Supplemental Table).
From the 29 studies, 6 common major findings were extracted (Table 3). Within the final articles, a number of different health education interventions and initiatives were mentioned. Researchers used a range of different study designs, underlying theories or frameworks, settings, outcome measures, and methods for data collection and analysis. However, only 38% articles (n = 11) directly measured HL. The majority reported a change in health-related knowledge or behaviors (82%, n = 24). The following recurring themes were recognized as limitations for a sustainable program: the need for ongoing support, the importance of relationships, educator confidence, cost, time, and staffing.
Findings from the Scoping Review of International Literature Describing the Key Characteristics of HLM.

Note: Grey shading indicates that the study findings described the corresponding key characteristics of a HLM.
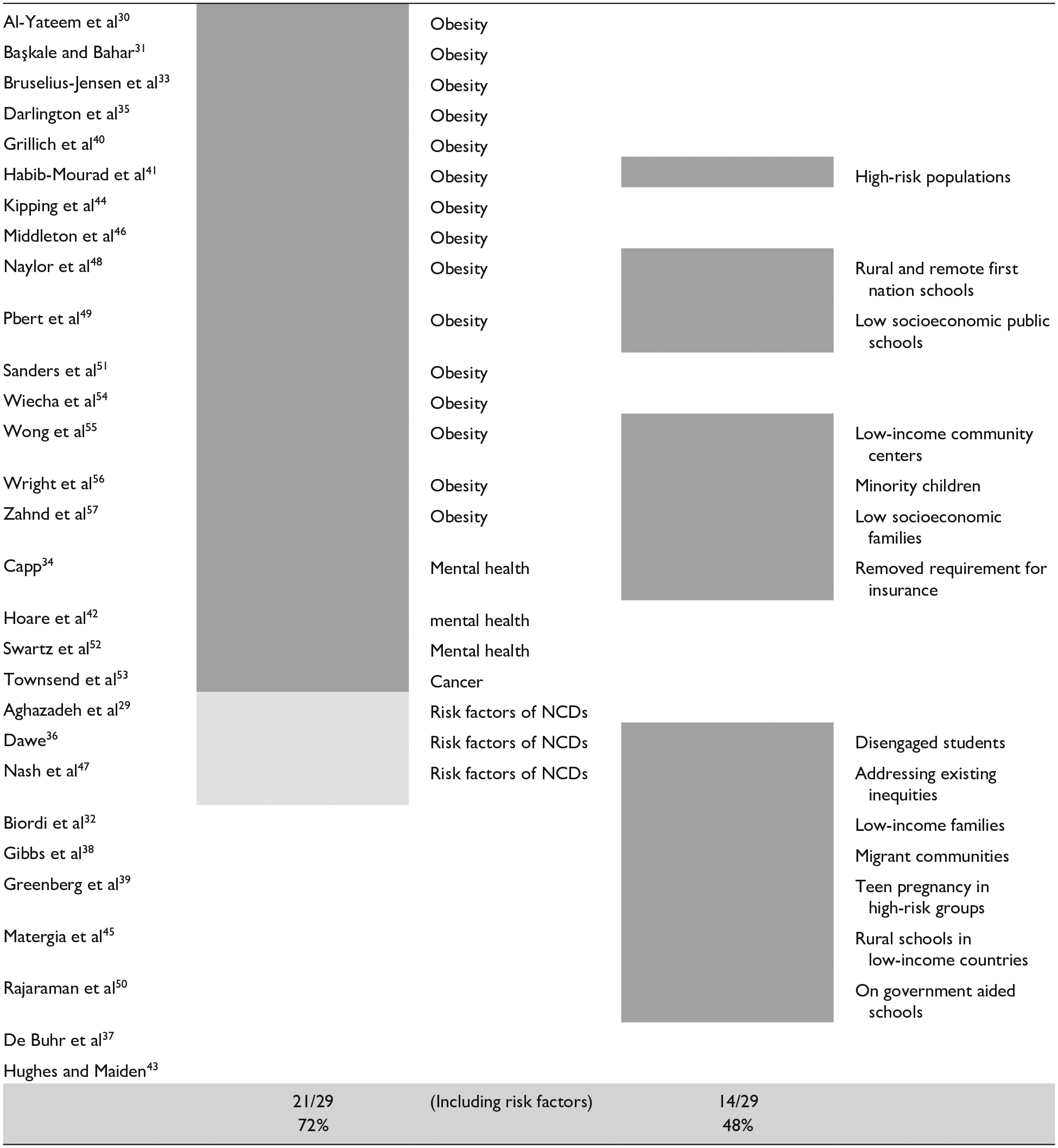
The majority of the HL interventions focused on non-communicable diseases (NCD) or their associated risk factors (72%, n = 21). Obesity was the most common risk factor considered, included in 15 of the 20 NCD focused articles. Less than half (48%, n = 14) of the articles described a focus on inequities in their participating communities (Table 4).
Non-Communicable Diseases and Inequity.


Note: Grey shading indicates that the study findings focused on NCD and/or inequities.
The interventions were delivered via different approaches (Table 5). Eighteen of the approaches described a Train-the-Trainer (TTT) type model (62%, n = 18) and used multiple groups of people in the process. An integrated approach occurred in 45% (n = 13) of studies, where the intervention was combined with existing curriculum/service being offered. Several key positions were identified as consistent with the definition of a HLM. The majority were teachers (38%, n = 11), followed by nurses (20%, n = 6).
Health Literacy Education.

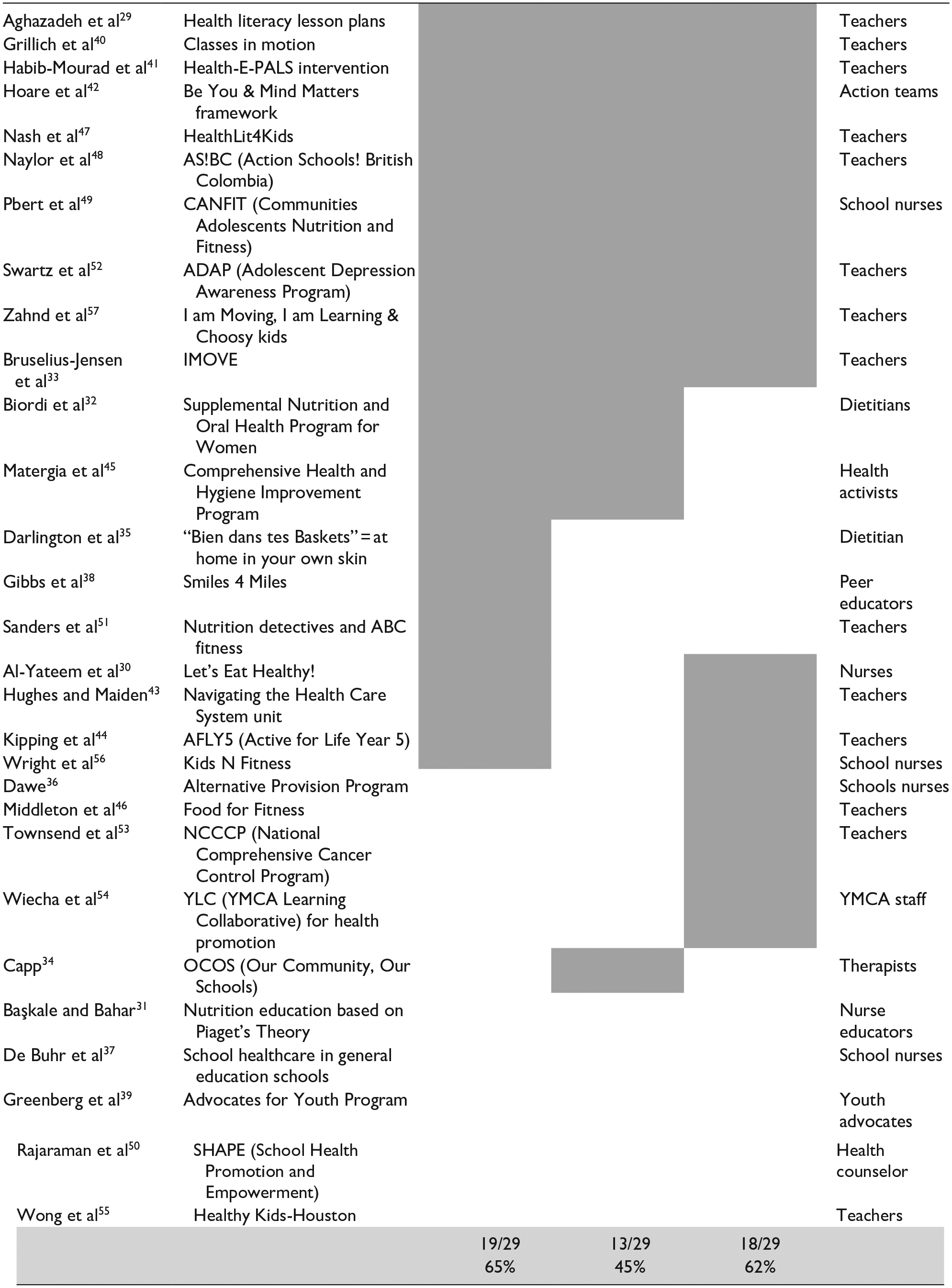
Note: Grey shading indicates which implementation approach the study used.
Train-the-trainer (TTT) = An approach where the intervention is initially taught to a person(s), who, in turn, go on to train other people within their organization or community.
Integrated = The intervention was combined within the existing curriculum and not a standalone topic/lesson.
Internal = The person(s) acting as the HLM were pre-existing staff members of that organization.
Discussion
From the results of this scoping review 6 key findings were identified in the literature. These were (1) directing HL education at children, (2) recognized importance of relationships, support, and training, (3) reported health knowledge acquisition, (4) reported changes in health behaviors, (5) reported changes in educator confidence knowledge and behaviors, (6) HL education limited by cost, time or staffing constraints. These key findings, and subsequent additional findings, have helped inform the development of the 5 themed discussion points that respond to the 2 research questions: What are the roles, responsibilities, and the optimal setting for a HLM? And can a HLM have an impact on redressing the health inequities in communities?
Health Knowledge and Health Behavior
In terms of interventions that included health knowledge acquisition as a reported outcome, the majority described an improvement in participants’ HL (Table 3). This suggests that the HLM has the potential to increase health knowledge in their individual settings. However, not all studies reported on knowledge as its own entity. A variety of techniques were used to engage participating students, including integrated lesson plans, whole-of-school approaches, a focus on student self-efficacy, and encouraging students to self-report their health knowledge. Integrated lessons were utilized in 13 articles (Table 5).
As evidenced by the literature, the benefits of employing an integrated lesson model are that it can facilitate a positive perception of the learning environment and set the learner up for long-term success.58,59 Many of these articles, for example Zahnd et al 57 and Swartz et al 52 indicate that health knowledge is promoted through an integrated approach (Table 3). Interestingly, only Naylor et al, 48 Middleton et al 46 and Nash et al 47 utilized a whole-of-school approach in their interventions (Table 5). They described that by using this method the children made self-reports on changes to their health, and the teachers could see a number of “healthy changes” for the children, as well as the whole-school environment. Self-report is a useful mechanism to encourage self-reflection (known to be a higher-order education practice); however, it has limitations. 60 Some of the studies used both self-report and performance-based tests, which gives greater confidence in their findings.31,33,40,44,48,49,55,56 Using a combination of self-report and performance-based assessments to establish HL asset acquisition could be valuable when measuring the influence of a HLM in the future. An integrated and whole-school approach can positively affect the HL of individuals, the broader school community, and promote cultural change within the educational setting. Therefore, these factors are important for a HLM to consider in their role and responsibilities. A HLM can impact health knowledge acquisition, which in turn has the potential to impact health behaviors.
Health behaviors post HLM intervention were determined through both subjective (self-report, observation, incident report) and objective measures (BMI, height, steps). The majority of the studies demonstrated changes to health behaviors (Table 3). Nutrition-focused studies found that by implementing their specific interventions (run by an HLM) the participants demonstrated positive changes in their health behavior.31,41,44,49 However, a minority of studies found no post-intervention changes in participants’ physical measures (weight, height, BMI),31,49 health behaviours,44,55 or health outcomes. 40 In addition, Bruselius-Jensen et al 33 found that while overall children learned new health-related knowledge, only a subset of participants learned to reflect critically on how to apply health recommendations in their everyday behaviors. This finding serves as a reminder that improvements in health behaviours will not always follow an individual’s knowledge acquisition. This could be explained by individual choices, but it is also critical that we consider the impact of people’s SDH on their own behaviour. 61
It is important that we define HL broadly and recognize the role of an individual’s social networks, as well as the responsibility of the services they are trying to access. Despite health knowledge improving in the majority of studies, not all demonstrate a change in health behaviors.29,36,37,43,46 This finding of no significant change is supported by others, stating that knowledge alone will not lead to a change in behavior.62-64 To change others’ behaviors, a HLM must be capable of promoting knowledge acquisition to enable individuals to autonomously make health-promoting decisions. A HLM with these attributes will be important in reducing the incidence of NCD and addressing the inequity perpetuated by inadequate HL that exists.
Inequity and Non-Communicable Disease
The social determinants of health (SDH) have the potential to perpetuate inequity in our communities.
5
HL has been recognized as a SDH of health in its own right, capable of redressing inequity.7,65 Improving HL has now been widely recognized as a key strategy in overcoming inequitable health disparities.
66
The current review revealed that only 48% (n = 14/29) of authors were conscious of how they could address the inequities in their communities. In those 14 articles, inequity was categorized in the following ways: low income (n = 7/14), a focus on minority groups (n = 6/14) and addressing existing inequities (n = 1/14) (Table 4). For example, Nash et al
47
utilized an action plan to help schools to support HL development, underpinned by the “Optimizing Health Literacy and Access”
Distinct from “equality,” the term “equity” refers to not all individuals having the same opportunities and abilities. With this in mind, a HLM could mediate and ensure activities and services respond to the child and the current needs of their family and community. 68 Gibbs et al 38 found that when implementing their smiles-4-miles community-based child oral health promotion, aimed at migrant families in Australia, the involvement of the cultural partners was a critical factor in recruiting participants and reviewing the promotion to ensure it met those families’ needs. A HLM therefore needs to be culturally competent, considerate of their context and able to harness the local wisdom in their program delivery. By doing this they can ensure they are efficient and effective educators of HL whose services respond directly to inequity.
People from lower socioeconomic backgrounds tend to have poorer health outcomes when they experience NCDs. 69 NCDs and their associated burden can be mitigated by empowering people to address common risk factors earlier in the life course. 70 The majority of the health interventions outlined in the final papers in this scoping review focused on NCDs or their risk factors (72%, n = 21) (Table 4). The most common emphasis was on obesity, with 15 out of the 20 NCDs targeting this issue. As highlighted by Marmot and Bell 69 we cannot solve obesity in isolation from inequity and the social determinants of health (such as agriculture, transport, housing, employment) (p. 10). Other NCDs that the HLM focused on included mental health, cancer prevention and more general risk factors, such as risk-taking behaviors.
Health Literacy in Childhood
Many health behaviors, attitudes, and knowledge are formed during childhood, making this period an appropriate time to commence HL education.61,71 Indeed, as shown in Table 3, many of the studies did provide HL education during the childhood years, with a median age of 10 years. For example, Aghazadeh et al, 29 Hoare et al 42 and Wright et al 56 recommended that HL should be developed concurrently with childhood health behaviors. In contrast, papers by Bruselius-Jensen et al, 33 Greenberg et al 39 and Hughes and Maiden 43 suggest that adolescence is an appropriate life stage to implement HL education, as this is a key transition period into adulthood. We argue that HL development should commence earlier in the life course, during childhood, but should continue, or be revisited, during adolescence. This would allow HL to be promoted as part of lifelong learning, developed through formal and informal learning opportunities at school and in the household.2,15
The potential for community-based settings to positively impact HL has been clearly established.38,55 A study by Wong et al 55 focused on nutrition literacy at a community center. This program was run by external providers who had no prior understanding of the specific needs of the students. The program demonstrated positive results with a reported improvement in knowledge, but no reported change in health behaviors. Wong et al 55 concluded that children under the age of twelve are mostly too young to independently control their food intake. These authors concluded that while community centers may positively influence health knowledge, schools may be more suitable to HL interventions as they have a broader reach. Despite the search not outlining a specific inclusion setting for a HLM, the majority of studies were conducted in schools (80%, n = 23/9) (Supplemental Table). This suggests that schools or formal education have been recognized as a key setting in which to implement HL interventions and a HLM could help to support this process.
Schools promote learning and children spend a significant amount of time there.34,36,42,45 Schools also have the potential to reach many children in the population irrespective of external factors such as socioeconomic status.61,71 This promotes an equitable and universal approach to facilitating HL development. Further, studies by Middleton et al 46 and Naylor et al 48 found that when nutrition programs were implemented in schools, they improved the whole school environment, as well as the population at which the intervention was aimed. The benefits of adopting interventions in school settings are many and include having the facilities to support ongoing interventions (repetition and scaffolding of learning), teachers and schools’ staff knowledge of the needs of their students, and schools being highly connected to the broader community. A HLM could support teachers in promoting and sustaining HL education, overseeing whole-of-school action plans and promoting a focus on health in the classroom. Additionally, other education-based settings such as after-school care, camps, and childcare could also be appropriate. For example, Wiecha et al 54 demonstrated a positive impact on healthy diets, physical activity, and screen time when they created a collaborative, supportive organizational approach involving after-school care services.
Relationships and trust are critical to HL interventions. This assertion was supported by a number of studies in this review (Table 3). For example, one study discussed how trust-building is a time-intensive but essential part of effective interventions, and that relationships take time to develop. 39 Dawe 36 reported on an alternative provision program, introduced by the school nurse, that covered a range of health topics and encouraged participants to take responsibility for their own health. This program strengthened the relationship between the school nurse (acting as HLM) and members of the school community (including teachers and students). In contrast, the interventions that relied on an external provider to come in and act as the HLM found it challenging and time-consuming to form these relationships with staff and students.34,45,50 However, it was recognized that these relationships were important for continuing success. Given the ongoing relationship between students, teachers, parents, and community members in schools, the school setting is ideally suited for a HLM to be positioned.
Distributed health literacy occurs when an individual benefits from the HL of others within their social networks. Students, friends, family, colleagues, and other members of the community mediate the development and practice of HL by sharing knowledge, facilitating learning, contributing their own skills, and supporting decision-making. 9 This review identified several articles with a school-based intervention that reported a transfer of knowledge and behaviors into the home environment.30,46,47 In addition, Başkale and Bahar 31 noted that after mothers were given nutrition education as a part of a school-wide intervention, their children’s health behaviors improved with “healthy food” consumption increasing further. It is important to note that not all children will have the independence to change their health behaviors in the home environment, 31 given their autonomy will be influenced by their SD.3,65 Change is a collaborative process between the child, their family, and their broader community. This in an important finding as it suggests that educating few to become health literate, could impact many.
Knowledge and Confidence of Educators
The HL of parents, families, and other people in the social context of a child is critical for their health development and their overall wellbeing. 37 In a formal educational setting, the HL of the teacher is an important factor in their ability to teach HL. A recent review by Otten et al 72 summarizes the experience of teachers’ professional development and self-confidence in HL education. The review, along with other literature, emphasized that to increase self-efficacy and positively impact the rate at which teachers implement health concepts in classrooms, teachers’ confidence in being able to teach health needs to be improved and supported.73-77 De Buhr et al 37 identified that teachers often feel their own HL is not sufficient to teach children, despite HL being included in the curriculum they are required to teach (Table 3). This is concerning, as 38% (n = 11) of health interventions identified by this study required the teacher to take on the role of the HLM (Table 5). Professional development has been shown to lead to an improved confidence and efficacy to teach health literacy. 77 A HLM could help to overcome this issue by supporting teachers in delivering HL education. For example, Aghazadeh et al 29 and Hughes and Maiden 43 noted that by teaching HL, staff reported developing new skills, creating team “drive,” enhancing staff relationships, and improving their own HL.
Teachers within a formal educational setting are an obvious choice to act in the role of a HLM. However, school-based nurses are equally well-situated to facilitate the teaching of health to students, in both the educational setting and the broader community. 78 Of the health interventions identified by this study, 20% (n = 6) of articles recognized nurses as the HLM (Table 5). For example, De Buhr et al 37 conducted a pilot study in Germany where school nurses received additional training and then implemented a flexible intervention to suit the schools that they worked in. The trained nurses provided separate health education sessions that followed a prescribed curriculum. As a result, the school nurses were accepted as experts in health-related topics by the extended school community and were able to improve the HL of the students, as well as the students’ educators and families. 37 Despite the positive outcomes, this article highlighted some of the limitations of having nurses as HLM. The main concerns were from the nurses themselves, as they stated that lack of time, inadequate training on how to teach their required topics and insufficient resources being available. These constraints were echoed by Dawe, 36 who found that limited school nurse numbers and increasing demands on school nurse time result in health education and promotion not being deemed as a priority within their role. This is concerning as the Nursing competency standards outline that it is a standard of practice for nurses to provide information and education to enhance people’s control over health. 13 If health education and promotion were delivered in schools to support HL development it could be key to addressing the increasing NCD burden globally.
For the reasons outlined above, formal education appears to provide a situation wherein teachers are trained to teach children, but do not have the training or perceived competence to teach HL and health topics. In contrast, nurses are trained in health and have good HL skills but are not specifically educated in how to best teach children. A HLM could resolve this situation by bridging the gap between the 2 roles. Further, a HLM could train others and build capacity within schools to produce health-literate organizations. 18 This approach is consistent with the Train-the-Trainer model (Table 5) employed by the majority of the articles in this review. For example, Sanders et al 51 looked in depth at this model for their fitness intervention and found that the staff and teachers appreciated the consistency and structure of training as well as the ongoing support from the professionals acting as the trainers.
Barriers to Health Literacy
Although most of the interventions in the present scoping review demonstrated positive impacts on HL, there were still a range of factors that were perceived as barriers in implementing HL education. The main factors indicated were cost, staffing availability, and time (Table 3). From the studies that reported on limitations, lack of time within the classroom schedule prevented the teachers, who were acting as HLMs, from implementing the school-based programs to the best of their ability and effect.43,44,51 This same issue was reported by Dawe 36 when their school nurses attempted to implement a classroom intervention. This issue indicates that it is hard to find designated time in the curriculum to employ such interventions. In addition, the lack of staffing or inadequately trained staff also influence how well the HL interventions were implemented. Townsend et al 53 stated that the main barries to implementation they experienced were changes in staff workload and staff movement. This resulted in teachers having to be continuously trained to maintain the program. Finally, additional costs for implementing programs were also an issue. For a sustainable intervention, costs that schools 51 or households 41 incurred must be kept minimal. A HLM has the potential to overcome these limiting factors by being a constant person within that school environment to promote the value of HL and train other staff on how to provide health education designed to develop health-literate children capable of making positive health decisions now and in the future.
Conclusion
This scoping review highlights the need for further research related to the development of the role of a HLM. Health literacy interventions are currently being implemented in schools and communities internationally. However, in general they do not always prioritize the health inequities within communities and could do more to enhance collaboration with healthcare professionals, educators, and families, to drive health literacy education. This review confirms that there is a lack of consensus on who should be teaching health literacy and that the confidence to teach health literacy differs between individuals and institutions. Barriers that professionals reported facing included a lack of time and a lack of knowledge. The emergent role of a HLM should be guided by the existing OpHeLiA principles and encompass cultural competence, confidence in providing education on HL and provide support to those around them. This would enable a HLM to promote positive HL of individuals, build relationships within communities and encourage a wider culture change. One crucial step forward will be to engage key stakeholders in meaningful discussions to co-design and agree upon the roles and responsibilities for a HLM in their current settings. This will ensure that the role is accepted, locally relevant, tailored to the needs of the community and able to address the health inequities that currently exist. A health literacy mediator is a cross-sector priority for education, health, and community leaders, which must be prioritized locally, nationally, and globally in order to redress inequities and combat the NCD epidemic.
Supplemental Material
sj-pdf-1-gph-10.1177_2333794X211025401 – Supplemental material for An International Review to Characterize the Role, Responsibilities, and Optimal Setting for Health Literacy Mediators
Supplemental material, sj-pdf-1-gph-10.1177_2333794X211025401 for An International Review to Characterize the Role, Responsibilities, and Optimal Setting for Health Literacy Mediators by Madeline Spencer, Nenagh Kemp, Vaughan Cruickshank, Claire Otten and Rosie Nash in Global Pediatric Health
Footnotes
Author Contributions
MS: contributed to conception and design; contributed to acquisition, analysis, and interpretation; drafted manuscript; critically revised manuscript; gave final approval; agrees to be accountable for all aspects of work ensuring integrity and accuracy. NK: contributed to conception and design; contributed to acquisition and interpretation; drafted manuscript; critically revised manuscript; gave final approval; agrees to be accountable for all aspects of work ensuring integrity and accuracy. VC: contributed to conception and design; contributed to acquisition and interpretation; drafted manuscript; critically revised manuscript; gave final approval; agrees to be accountable for all aspects of work ensuring integrity and accuracy. CO: contributed to interpretation; drafted manuscript; gave final approval; agrees to be accountable for all aspects of work ensuring integrity and accuracy. RN: contributed to conception and design; contributed to acquisition, analysis, and interpretation; drafted manuscript; critically revised manuscript; gave final approval; agrees to be accountable for all aspects of work ensuring integrity and accuracy.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was made possible by a PhD scholarship from the College of Health and Medicine from the University of Tasmania awarded to M. Spencer. And also, Higher Degree Research (HDR) funding from the University of Tasmania awarded to M. Spencer to cover publication fees. All the other authors have received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.