
Abstract
Objectives:
Non-communicable diseases are non-infectious health conditions caused by genetic, physiological, environmental, and behavioral factors. Currently, non-communicable diseases account for almost two-thirds of deaths globally. This study aimed to explore the patients’ adherence level to the key recommendations, and the main barriers toward the practice of healthy behaviors among non-communicable diseases patients.
Method:
This cross-sectional study was conducted among a representative sample of non-communicable diseases patients, receiving care in five primary healthcare centers in the Gaza Strip, Palestine. An interview-based questionnaire about demographics, medical history, and barriers toward the practice of healthy behaviors was developed and collected based on the health belief model and the theory of planned behaviors. Independent samples t-test, one-way analysis of variance, chi-square, and Fisher’s exact test were used for analysis.
Results:
Four hundred patients with non-communicable diseases, aged (53.06 ± 10.03) years old, (56.8% females and 43.3% males) were included in this study. The patient’s adherence was reported as 50.1%, standard deviation = 18.3 in terms of attended regular physical activity, and 44.0%, standard deviation = 15.4 in terms of eating a healthy diet. The main barriers to being active among patients were lack of accessibility to materials, lack of social support, and lack of reminder; while in terms of eating a healthy diet were lack of accessibility to materials, lack of social support, and lack of self-efficacy.
Conclusion:
The non-communicable diseases patients’ adherence to healthy behaviors is suboptimal. Varied implementation strategies targeting the main barriers are extremely required to enhance the access to physical activity infrastructure, affordable healthy diet options, and to reinforce the change toward healthy behaviors at all levels.
Keywords
Introduction
Non-communicable diseases (NCDs) are non-infectious health conditions caused by genetic, physiological, environmental, and behavioral factors. 1 Chronic diseases are identified as a major public health concern worldwide, and contribute to a large burden of diseases in high-income countries, and increasing rapidly in low- and middle-income countries. 2 The World Health Organization (WHO) estimated that NCDs including cardiovascular diseases (CVDs), cancer, diabetes, and chronic respiratory diseases were responsible for 41 million deaths yearly and account for 71% of all deaths worldwide; most of NCDs death (74%) and the majority of premature deaths (82%) occur in low- and middle-income states. 3 By 2030, around 80% of those deaths will come from low- and middle-income countries, with the prediction of about 52 million deaths yearly. 4 Like other low- and middle-income countries, Palestine is experiencing a quick epidemiological transition, with increasing the burden of NCDs. 5 It was estimated that nearly two-thirds of elderly Palestinians complain from NCDs. 6 Gaza Strip is part of Occupied Palestinian Territory which characteristic by high densely peopled territory, with a total number of populations around two million, more than 70% of them are registered as refugees, it was estimated that the prevalence of overweight and obesity among the Palestinian population was 62.4% and 24.4%, respectively.7,8 Gaza Strip since 2007 under siege which influencing all aspects of life, more than half of the population suffering from poverty, majority of the people had received aids, around 80% of peoples are dependent on food aids. 9 In 2016, CVDs remain the first leading cause of death among Palestinians, accounting for 30.6% of deaths recorded; cancer was the second leading cause of death, with 14.0% of deaths; complications of diabetes came in the fourth rank with a proportion of 8.0%. 10 The four main diseases that account for the majority of deaths from NCDs include CVDs, cancers, chronic respiratory diseases, and diabetes. 4 Importantly, these four NCDs share common behavioral risk factors including tobacco use, unhealthy diet, physical inactivity, and harmful use of alcohol. 4 Recently, there is a wide scientific and public health policy agreement that these factors contribute significantly to NCDs morbidity and mortality. 11 The WHO developed a package of essential NCDs interventions (WHO-PEN), which is the minimum standard for NCDs to strengthen national capacity to integrate and scale up care of NCDs in primary health care centers (PHCs) in low-resource settings. 12 In 2013, the Palestinian Ministry of Health introduced the WHO-PEN in primary health care. 13 The introduction of the WHO-PEN approach, including the training of employees, adapting record keeping and the health information system, and support supervision, has delegated most NCDs management responsibilities to general physicians and nurses working in PHCs. 13 Besides, WHO-PEN protocol 2 is a significant tool in the implementation process, which is concerned with health education and counseling on healthy behaviors for NCDs patients. 12 It included instructions to educate the NCDs patients to take regular physical activity, eat a healthy diet, stop tobacco and harmful use of alcohol, and attend regular medical follow-up. 14 In Gaza Strip, Palestine, a recent study demonstrated that more than half (57.7%) of PHCs had all of the counseling services recommended by the WHO-PEN protocol 2 including counseling on healthy behaviors for NCDs patients and family in terms of smoking, diet, alcohol and physical activity. 15 Another study conducted in Gaza Strip showed that only 12.5% of health care professionals claimed that they are rarely or never adherence to counseling on healthy behaviors in terms of physical activity and 19.5% in terms of a healthy diet based on WHO-PEN protocol 2. 16
Modifications of barriers toward the practice of healthy behaviors can lead to great benefits for NCDs patients. 14 Based on the health belief model and theory of planned behavior,17,18 there were seven main determinants of human behaviors including perceived self-efficacy, perceived social acceptability, perceived action efficacy, cues for action, accessibility of materials, perceived susceptibility, and perceived severity. In addition, to encourage people to follow a healthy lifestyle, a suitable understanding of the barriers, particularly changeable barriers, faced by patients who received counseling on healthy behaviors is essential, and identifying these barriers by healthcare providers can help behavior alteration. 19 This study aimed to explore the NCDs patients’ adherence level to the key recommendations on healthy behaviors provided by general physicians and nurses working in the PHCs, and the main barriers toward the practice of healthy behaviors to take regular physical activity and eat a healthy diet among NCDs patients in the PHCs in Gaza Strip, Palestine.
Methods
Study participants
This cross-sectional study was conducted from September 2019 to May 2020, among a representative sample of NCDs patients (both genders, aged ⩾18 years), selected by a convenience sampling method from patients receiving care in five PHCs in Gaza Strip, Palestine. Participants were selected from the five Gaza Strip governorates based on the population density; Gaza Strip is divided into five smaller governorates, which include North Gaza, Gaza, Deir Al Balah, Khan-Yunis, and Rafah. 15 The five PHCs were selected purposively to include the centers with high utilization and attendance of NCDs services in each governorate of Gaza Strip, Palestine.
Eligibility criteria
Inclusion criteria include patients with one of the major NCDs (CVDs, chronic respiratory disease, cancer, and diabetes), both genders, aged ⩾18 years, and registered and receiving treatment in the five selected Ministry of Health, PHCs in Gaza Strip.
Exclusion criteria include patients who did not receive treatment in the five selected PHCs, or their medical files are not available. In addition, pregnant, lactating women, and patients with other types of NCDs illness such as multiple sclerosis and osteoarthritis were also excluded from the study.
Sample size and sampling
The traditional equation (Cochran) was used to calculate the sample size, 20 and the estimated sample size according to the equation is 384 cases, with a margin of error of 5% and confidence level of 95%. In addition, the sample size was increased to 400 cases; chosen were distributed based on the population density in the five Gaza Strip governorates. 21 The study sample was distributed in each governorate (North Gaza, Gaza City, Mid Zone, Khan Younis, and Rafah) as follows 78, 137, 58, 78, and 49 patients, respectively.
Data collection
A structured questionnaire was used to collect data from NCDs patients via individual interviews during clinic work hours. Data were collected by five data collectors after one full day of training about the study scope and purposes, questionnaire items, and possible areas for misunderstanding.
Study instrument
Based on the health belief model and the theory of planned behavior,17,18 the questionnaire was developed after reviewing the previous appropriate studies questionnaires.22–24 A preliminary questionnaire with 14-items to assess barriers of adherence to healthy behaviors (of regular physical activity and eat a healthy diet) among NCDs patients and the seven main determinants of human behaviors were surveyed. In addition, nine-items to assess the socio-demographic characteristics of the patients, and seven-items to exploring the adherence level to healthy behaviors were also included. The healthy behaviors recommendations are defined based on WHO-PEN protocol 2 for all NCDs patients. 14 A 5-point Likert-type scale was used for response categories with the rating scale of “always,” “often,” “sometimes,” “rarely,” and “never.” For main perceived barriers responses categorized to yes or no. “always,” “often,” and “sometimes” consider as Yes and “rarely” and “never “consider as No.
Translation and validation of the questionnaire
The cross-cultural guideline process was employed in the translation of the questionnaire. 25 Face and content validity were checked for the final Arabic draft questionnaire, independently validated by seven experts (researchers, health experts, head nurse, and family doctors). Content validity index was calculated to rate the relevance of the questionnaire items. 26 All items were rated as relevant. Minor changes in the language and the construction were done. Then, the questionnaire was piloted among 30 of the eligible NCDs patients, and the results of the pilot study showed a good overall Cronbach’s alphas of 0.85.
Data analysis
The SPSS software version 22 was used for the statistical analysis. Characteristics of the sample were described by descriptive statistics. Frequencies and percentages were used to describe categorical variables, whereas mean values and standard deviations (SDs) were used to represent continuous variables. The Shapiro–Wilk test was used to test the normality of quantitative variables. Independent-samples t-test, one-way analysis of variance (ANOVA), chi-square, and Fisher’s exact test were used for analysis. p-values of less than 0.05 were considered statistically significant.
Results
Characteristics of the study participants
The characteristics of the study participants are summarized in Table 1. A total of 400 patients with NCDs, aged (53.06 ± 10.03) years old were included in this study. Approximately half of the respondents (56.8%) were females, 46.8% had a university degree, 45.5% jobless or retired, and only 7.8% of the participants were a smoker. Most of the study respondents (74.8%) were married, about two-third had incomes less than 2000 new Israeli shekel (NIS) per month, and 88% were above 40 years old.
Characteristics of the study participants.

SD: standard deviation; NIS: new Israeli shekel; NCDs: non-communicable diseases.
Data are expressed as percentage for different categorical variables.
Other includes cancer or cancer + hypertension + diabetes mellitus or diabetes mellitus + cardiovascular diseases or hypertension + cardiovascular diseases or diabetes mellitus + hypertension + cardiovascular diseases.
NCDs patient’s adherence level to the key recommendations of healthy behaviors
In addition, Table 2 shows that the adherence mean scores across the key recommendations of healthy behaviors (take regular physical activity and eat a healthy diet) were reported as 50.1%, SD = 18.3 in terms of attended regular physical activity, and 44.04%, SD = 15.4 in terms of eating a heart-healthy diet. Only 16.8% of patients claimed that they always and often progressively increase physical activity to moderate levels, and only 1.8% of patients reported that they always and often eat 400–500 g of fruits and vegetables per day as recommendations.
NCDs patient’s adherence level to the key recommendations of healthy behaviors.
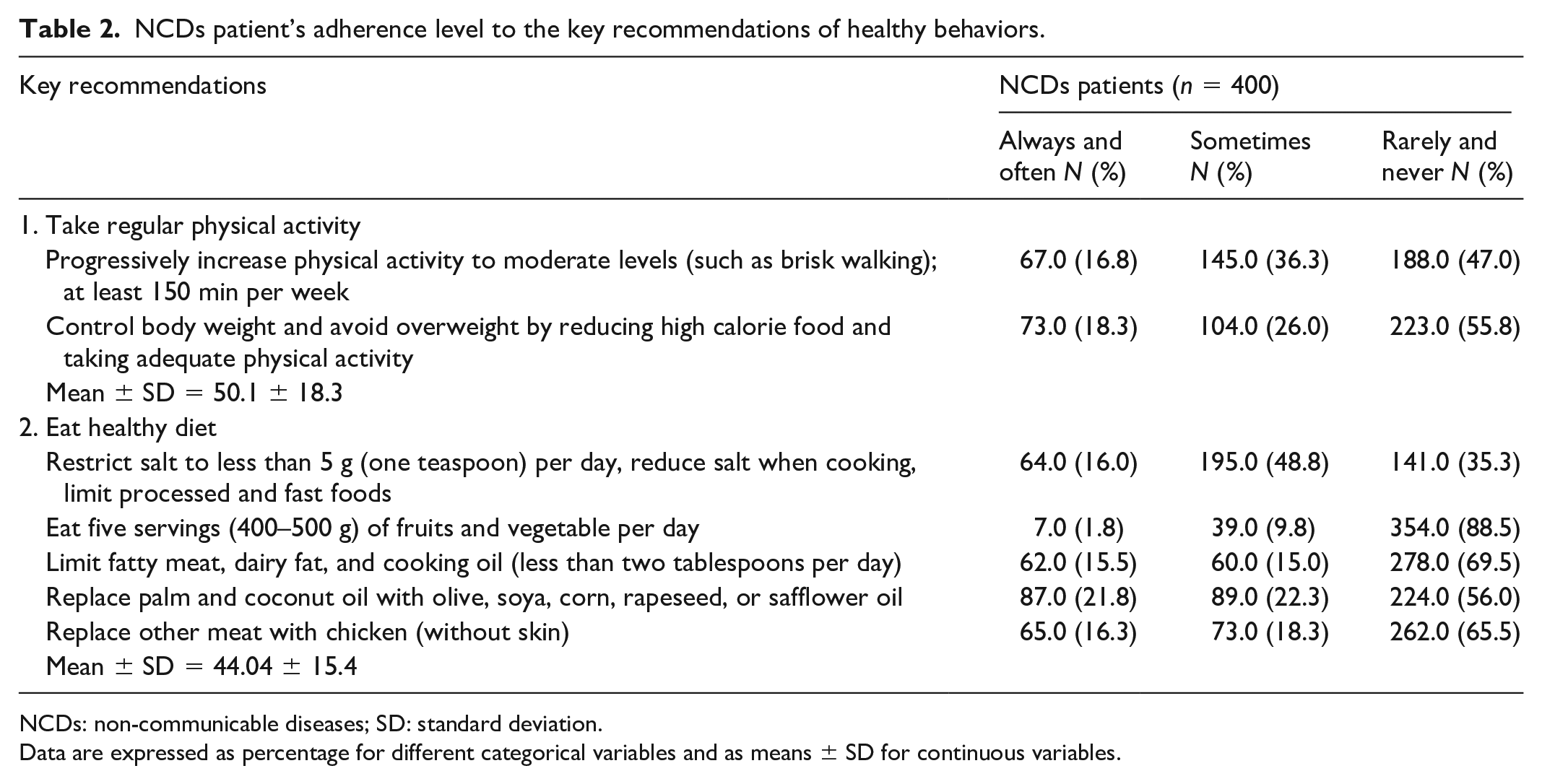
NCDs: non-communicable diseases; SD: standard deviation.
Data are expressed as percentage for different categorical variables and as means ± SD for continuous variables.
Characteristics of the study participants in relation to adherence level to the key recommendations
Furthermore, Table 3 demonstrated that in terms of taking regular physical activity, the mean scores were statistically significant differences between different age groups, education level, and occupation status. The age group less than 40 years old were more physically active compared to other age groups (55.8%, SD = 17.2), and the age group between 40 and 60 years old were more physically inactive (48.2%, SD = 18.8). The participants with postgraduate certificates were more physically active compared to other education levels (61.1%, SD = 13.7), and the participants with primary education were more physically inactive (46.2%, SD = 20.1). The jobless participants were more physically active compared to others (54.4%, SD = 17.9), and the employed participants were more physically inactive (47.6%, SD = 18.9). In terms of eating a healthy diet, all attributes mean scores (gender, age, marital status, smoking status, education level, occupation status, income, and NCDs types) were statistically significant differences, except marital status and smoking status. The adherence to eating a healthy diet was more, among females were 46.2%, SD = 16.9, compared to males, among the participants less than 40-year-old were 46.6%, SD = 18.3, compared to others age groups, among the postgraduate certificates participants were (65.1%, SD = 21.2), compared to other groups, among the jobless participants were (46.9%, SD = 16.2), compared to retired and employed, among the participants who had income more than 3000 NIS were (53.0%, SD = 17.2), compared to other groups, and among the patients with CVDs were (60.9%, SD = 12.9), compared to the patients with other types of NCDs.
Characteristics of the study participants in relation to adherence level to the key recommendations.
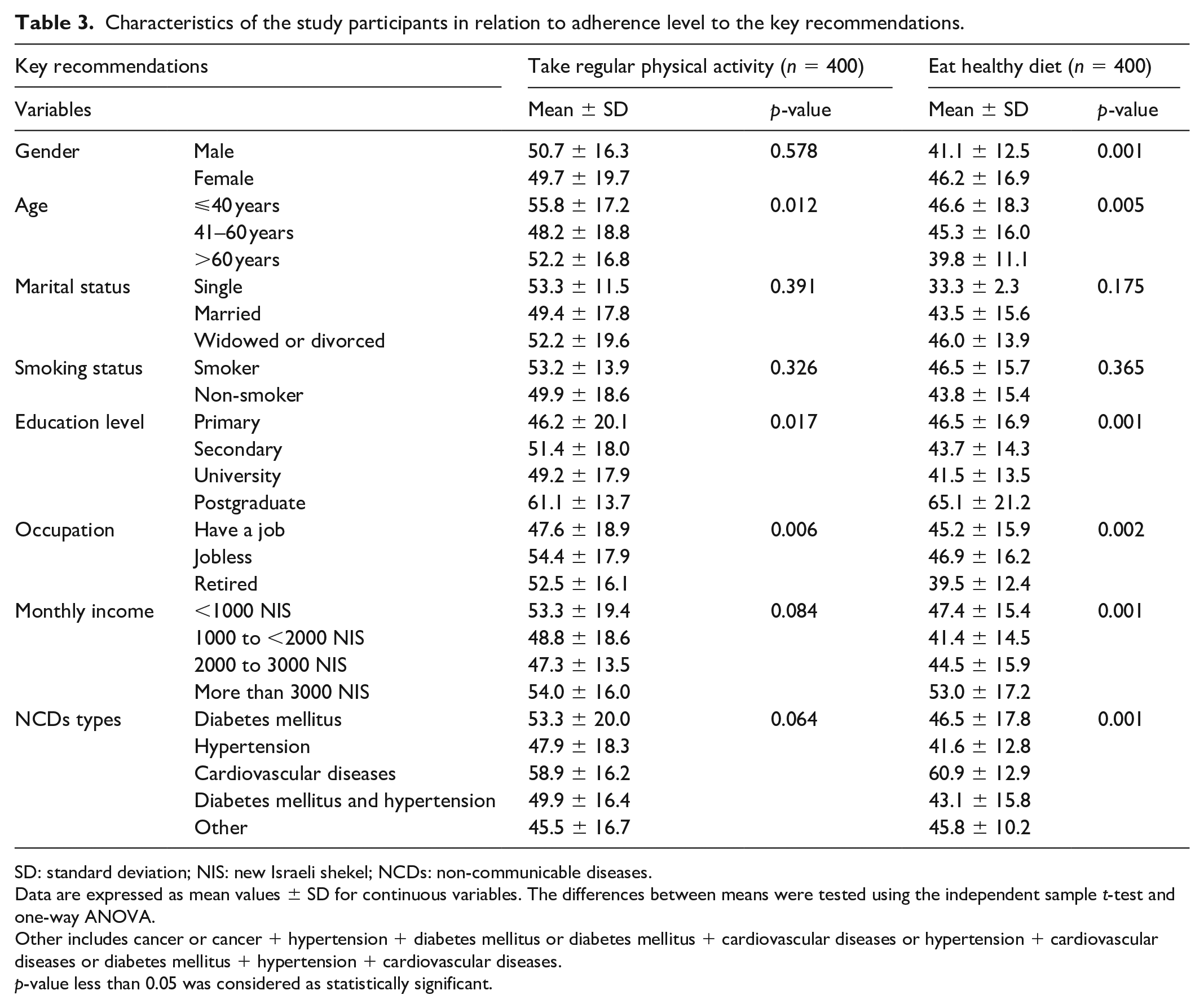
SD: standard deviation; NIS: new Israeli shekel; NCDs: non-communicable diseases.
Data are expressed as mean values ± SD for continuous variables. The differences between means were tested using the independent sample t-test and one-way ANOVA.
Other includes cancer or cancer + hypertension + diabetes mellitus or diabetes mellitus + cardiovascular diseases or hypertension + cardiovascular diseases or diabetes mellitus + hypertension + cardiovascular diseases.
p-value less than 0.05 was considered as statistically significant.
Characteristics of the study participants in relation to barriers toward practice of physical activity
Moreover, Table 4 demonstrated that the majority (92.0%) of participants believed that by adhering to physical activity, the NCDs will be under control, and 82.0% of the participants believed that non-compliance to physical activity will lead to serious NCDs complications. The main perceived barrier to being active was lack of accessibility of materials (98.4%), which was significantly higher among widowed, divorced, primary education level, and was significantly lower among employed as well as hypertensive patients. The lack of social support ranked as a second barrier to being active (55.5%), which was significantly higher among retired and CVDs patients and was significantly lower among females, smokers, and income class between 1000 and <2000 NIS. The lack of reminder to action ranked as a third barrier to being active (54.8%), which was significantly higher among retired, CVDs patients, and the highest income group and was significantly lower among female as well as primary education level patients.
Characteristics of the study participants in relation to barriers toward practice of physical activity.
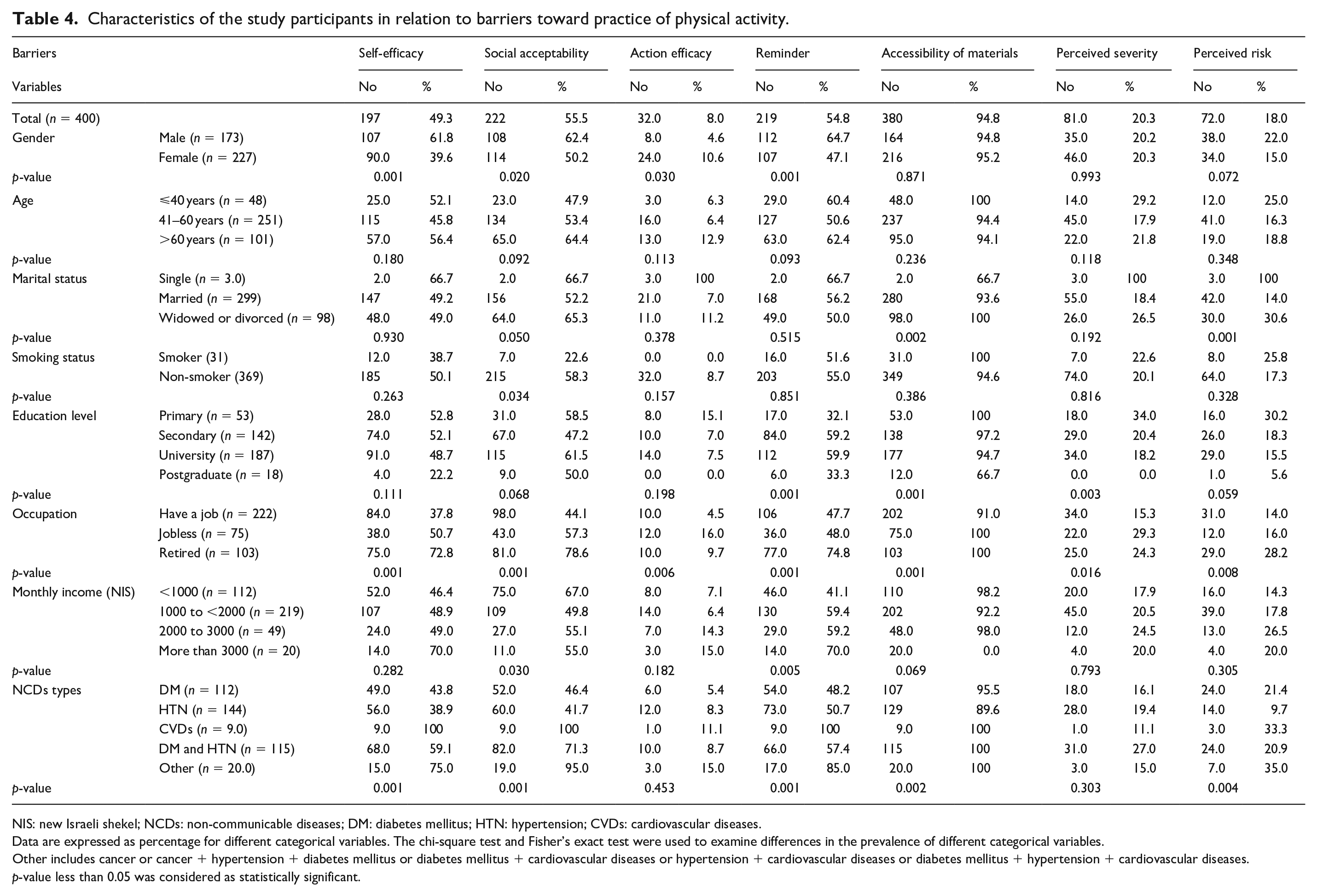
NIS: new Israeli shekel; NCDs: non-communicable diseases; DM: diabetes mellitus; HTN: hypertension; CVDs: cardiovascular diseases.
Data are expressed as percentage for different categorical variables. The chi-square test and Fisher’s exact test were used to examine differences in the prevalence of different categorical variables.
Other includes cancer or cancer + hypertension + diabetes mellitus or diabetes mellitus + cardiovascular diseases or hypertension + cardiovascular diseases or diabetes mellitus + hypertension + cardiovascular diseases.
p-value less than 0.05 was considered as statistically significant.
Characteristics of the study participants in relation to barriers toward practice of healthy diet
In addition, Table 5 demonstrated that the vast majority of participants (88.7%) believed that by adhering to eating a healthy diet the NCDs will be under control, and the majority (81.0%) of participants believed that the NCD a serious health condition. The main perceived barrier to adherence to the eating of a healthy diet was the lack of accessibility to materials (96.0%), which was significantly higher among primary education patients. The lack of social support ranked as a second barrier to eating a healthy diet (63%), which was significantly higher among males, smokers, retired, and the lowest income group. The lack of self-efficacy ranked as a third barrier to eating a healthy diet (61%), which was significantly lower among females, primary education level, and the highest income group.
Characteristics of the study participants in relation to barriers toward practice of healthy diet.

NIS: new Israeli shekel; NCDs: non-communicable diseases; DM: diabetes mellitus; HTN: hypertension; CVDs: cardiovascular diseases.
Data are expressed as percentage for different categorical variables. The chi-square test and Fisher’s exact test were used to examine differences in the prevalence of different categorical variables.
Other includes cancer or cancer + hypertension + diabetes mellitus or diabetes mellitus + cardiovascular diseases or hypertension + cardiovascular diseases or diabetes mellitus + hypertension + cardiovascular diseases.
p-value less than 0.05 was considered as statistically significant.
Discussion
This study’s findings give initial evidence of the NCDs patient’s adherence level to healthy behaviors, as well as main perceived barriers to being active and eat a healthy diet among NCDs patients in the Palestinian context. Healthy behaviors change can be reached by developed strategies; these strategies need a full understanding of perceived barriers to reach them. 27 The study demonstrated that the NCDs patients’ compliance mean score to take regular physical activity was 50.1%, SD = 18.3 and compliance to eat a healthy diet was 44.0%, SD = 15.4. The main barriers to being active among patients were lack of accessibility to materials, lack of social support, and lack of reminder, while in terms of eating a healthy diet were lack of accessibility to materials, lack of social support, and lack of self-efficacy.
First, the NCDs patients’ compliance mean score to take regular physical activity was 50.1%, SD = 18.3, In the United States, studies conducted demonstrated that 34%–69% of diabetes patients attended the physical activity, and 9%–31% of them attended regular physical activity as recommendations. 28 In Saudi Arabia, 49.5% of NCDs patients claimed that they do some type of exercise, 43.2% do walking, and only 5.9% do brisk walking, 29 and 43.6% of diabetes patients followed exercises. 30 In South Africa, 65% of NCDs patients claimed that they were moderately active. 31 In Pakistan, a study demonstrated that 23.6% of hypertensive patients usually do physical activity. 32
Second, this study findings showed that the NCDs patients’ compliance to eat a healthy diet was 44.0%, SD = 15.4. In Saudi Arabia, more than 50% of diabetes patients did not comply with the American Diabetes Association’s recommendations in terms of diet, 33 and another study demonstrated that 56.7% of diabetes patients followed a healthy diet. 30 In Pakistan, 55.1% of hypertensive patients were having salt restriction. 32
It is clear that being younger, higher education, and jobless participants were more adherence to the key recommendations. The possible explanation for that the adherence to the key recommendations needs more free time (young and jobless patients) may have more leisure time or free time, which gives them more opportunity to practice physical activity or eat a healthy diet. Higher education patients may be due to their understanding of the nature of disease consequences and the associated mortality.
The main perceived barriers to being active among NCDs patients were the lack of accessibility of materials, lack of social support, and lack of reminder. The vast majority of participants (92.0%) believed that by adhering to eat a healthy diet the NCDs will be under control, the majority (82.0%) of participants believed that non-compliance to physical activity may lead to a serious NCDs complication, and approximately 80% believed that the NCDs is a serious health condition. The lack of accessibility to materials, lack of social support, and lack of self-efficacy were the main perceived barriers among NCDs patients to eat a healthy diet, the vast majority of participants (88.8%) believed that by adhering to eat a healthy diet the NCDs will be under control, 80.5% believed non-compliance to a healthy diet may lead to a serious NCDs complication, and the majority (81.0%) of participants believed that the NCD is a serious health condition. For both, take regular physical activity and eat a healthy diet, the lack of accessibility to materials and lack of social support ranked as the first and second perceived barriers for compliance, this study’s findings are consistent with previous studies that defined lack of resources or materials and lack of social support as the main barrier to attending healthy behaviors.22–24 The possible explanation for the inaccessibility to materials may be that the Gaza Strip since 2007 has been under a siege that affects all aspects of life, with a poverty rate of 53%, and 79% of the people had received aids. 34 In addition, around 80% of people in the Gaza Strip are dependent on food aids, 35 it is difficult for people facing these challenges join a club or buy suitable equipment for attending the physical activity, and buy different foods recommended such as different types of fruits and vegetables and a special type of oil or meat. The second-ranked barrier was lack of social support; any efforts to change toward healthy behaviors from patients will take place in a social setting. 36 So, it is believed that social can promote adherence by providing help in activities. 37 Interventions include family support can have better results in compliance among patients. 38 A previous study conducted showed that social support can increase the duration of physical activity by about 44%. 39 The third main perceived barrier in terms of physical activity was lack of reminder, which was significantly higher among retired, CVDs patients, highest income group and was significantly lower among female as well as primary education level patients, 67.4% of male participants claimed that they are forgetting to attended regular physical activity, and 74.8% of retired patient, our findings consistent with previous studies which defined lack of reminder to act as main barriers adherence to healthy behaviors.22,40 The third main perceived barrier in terms of eating a healthy diet in this study was lack of self-efficacy; the lack of self-efficacy in previous studies was defined as the most determinant of healthy behaviors.41,42 Feeling a deficit or if an individual believes that he cannot alter the behavior, then he will not even try to change it and try to adopt healthy behaviors.19,43 The evidence showed that the preliminary stage of change toward healthy behaviors is important to increase self-efficacy; so, success in the preliminary stage will increase self-efficacy and failure will increase the frustration through individuals. 19 Therefore, the people who are educated to start with simple and reachable healthy behaviors can build-up self-confidence and be more effective to change toward healthy behaviors. 44
A possible limitation of the study is the dependence on self-reported data, which could lead to recall bias and social desirability bias. Small sample size can be also one of the limitations of this study, in spite of that, this study provides preliminary results about NCDs patients’ adherence level to healthy behaviors, as well as main perceived barriers to being active and eat a healthy diet among NCDs patients in the Palestinian context.
Conclusion
The NCDs patients’ adherence to healthy behaviors is suboptimal. Varied implementation strategies targeting the main barriers are extremely required to enhance the access to physical activity infrastructure, affordable healthy diet options, and to reinforce the change toward healthy behaviors at all levels.
Supplemental Material
sj-pdf-1-smo-10.1177_20503121211029179 – Supplemental material for Barriers toward the practice of healthy behaviors among patients with non-communicable diseases in Gaza Strip, Palestine
Supplemental material, sj-pdf-1-smo-10.1177_20503121211029179 for Barriers toward the practice of healthy behaviors among patients with non-communicable diseases in Gaza Strip, Palestine by Ahmed Hassan Albelbeisi, Ali Albelbeisi, Abdel Hamid El Bilbeisi, Mahmoud Taleb, Amirhossein Takian and Ali Akbari-Sari in SAGE Open Medicine
Footnotes
Acknowledgements
The authors thank the staff and participants in the Palestinian Ministry of Health, PHCs for their important contributions to the study.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
The study protocol was approved by the Ethics Committee of Tehran University of Medical Sciences (Code: IR.TUMS.REC.1398.349) and by the Palestinian Health Research Council (Helsinki Ethical Committee of Research PHRC/HC/599/19). In addition, written informed consent was also obtained from each participant.
Informed consent
Written informed consent was also obtained from each participant.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.