
Abstract
Introduction:
Non-communicable disease contributes to over 42 million deaths worldwide and it is estimated that 86% of non-communicable disease-related mortalities happen in low and middle-income countries. Understanding health-seeking behaviors like initiating care at the right time, with the right provider and maintaining regularity of care seeking is a prelude for a successful management of non-communicable diseases. Therefore, the aim of this systematic review and meta-analysis was to assess the pooled prevalence of health-seeking behavior for non-communicable disease and associated factors worldwide.
Method:
Preferred Reporting Items for Systematic Reviews and Meta-Analysis checklist guideline was followed for this review and meta-analysis. Electronic data base, PubMed, EMBASE, Medline, Web of science, Google scholar and Science direct were used to retrieve studies reported in English language with publication year since 2018 worldwide. Studies reporting proportion of health-seeking behavior for non-communicable disease were evaluated. The pooled prevalence, odds ratio and confidence interval were calculated using Stata version 17 software. The quality of studies included in this review was checked using modified Newcastle-Ottawa scale for observational study checklist.
Result:
Ten studies which involved 63,498 patients with non-communicable disease were included in this review. The pooled estimated proportion of health-seeking behavior among non-communicable diseases patients from health facilities were 56% (95% CI: 44–68). Older age > 60, urban residency, being of female gender, high educational status, getting support during treatment, knowledge on non-communicable disease, having more than one non-communicable disease, presences of health insurance and middle and upper economic class were factors positively associated with health-seeking behavior for non-communicable diseases.
Conclusion:
Despite the fact that more than half of patients with non-communicable diseases have health-seeking behavior in health facilities, still, there are a considerable number of individuals with non-communicable diseases having no health-seeking behavior worldwide. Therefore, organizations working for the welfare of human betterment would do well in implementing strategies that could improve health-seeking behavior that would help to reduce the burdens on health systems and prevent premature death from non-communicable diseases.
Introduction
Non-communicable diseases (NCDs) are the top causes of premature mortality and disability globally, even though low- and middle-income countries are disproportionately affected. 1 NCDs contributed to over 42 million deaths worldwide (74.4% of all deaths) in 2019. It is estimated that 86% of all NCD mortalities happen in low- and middle-income countries. The four major NCDs were cardiovascular diseases, cancers, chronic respiratory diseases, and diabetes. 2 NCDs have posed an enormous risk to human health due to their high prevalence and associated mortality. 3 The risk factors of NCDs were classified as modifiable (Physical inactivity, tobacco use, alcohol consumption and unhealthy diets) and non-modifiable factors (age, gender, genetics, and race). 4
Tackling NCD is the top priority agenda of the sustainable development goal (target goal: 3.4) which calls for action to lower NCD-related mortality. 5 To effectively combat the burdens of NCD, prevention mechanisms besides the provision of early screening and timely treatment are required; however, many low-income countries lack adequate resources and holistic approach that work across health system and provide the means required to tackle NCDs. 6 NCDs are an undeniable global challenge, increasing and multiplying with age, and are associated with higher and disproportional use patterns of health services. 7
Primary health care (PHC) service approach, which deals with health in a comprehensive way, including the promotion, prevention, and control of diseases, can be useful in both high and low resource settings. 8 Further, a PHC-based approach also provides opportunities for communities to better access appropriate healthcare, which ensures more significant equity, efficiency, effectiveness, safety, and timeliness, empowers service users, and helps healthcare providers to achieve better health outcomes at lower costs.
Health-seeking behavior is one of the main determinant factors of populations’ health outcomes with the spirit of utilization of health services. 9 Health-seeking behavior is defined as any action undertaken by individuals who perceive themselves to have a health problem or being ill to find an appropriate remedy. 10
Health-seeking behaviors (e.g., initiating care at the right time, with the right provider; maintaining regularity of care seeking) are a prelude for a successful management of NCD. An individual’s tendency to seek out health care is influenced by a variety of factors, including socioeconomic conditions, age, gender, financial means, their own perceived health status and illness, type of illness, as well as the available health services and access to them. 11 Delaying seeking the right diagnosis and care can have negative consequences, including higher mortality. 12 In order to prevent and manage early NCD, it is crucial to understand the dynamics of health care seeking among peoples with these chronic diseases. The strategies created should guarantee continuity of care at a price that is affordable to everyone. 13 However, there was no systematic review and meta-analysis that determines health-seeking behavior for the availability of evidence to support policy-making and promote health-seeking behavior. Therefore, this systematic review and meta-analysis aimed to assess the pooled prevalence of health-seeking behavior on non-communicable disease and associated factors and to summarize the reasons for not seeking care for NCDs.
Methods
Search strategies
This systematic review and meta-analysis was conducted to estimate the pooled proportion of health-seeking behavior and to summarize the reasons for not seeking care for NCDs. Preferred reporting items of systematic review and meta-analysis (PRISMA) flow diagram standards (Figure 1) and PRISMA checklist were used during the review process. Electronic database such as PubMed, EMBASE, Medline, Web of science, Google scholar, and Science direct were used to retrieve studies reported in English language with publication year from 2018 to 30 May 2030.The search was conducted from 30 May to 20 June 2023.
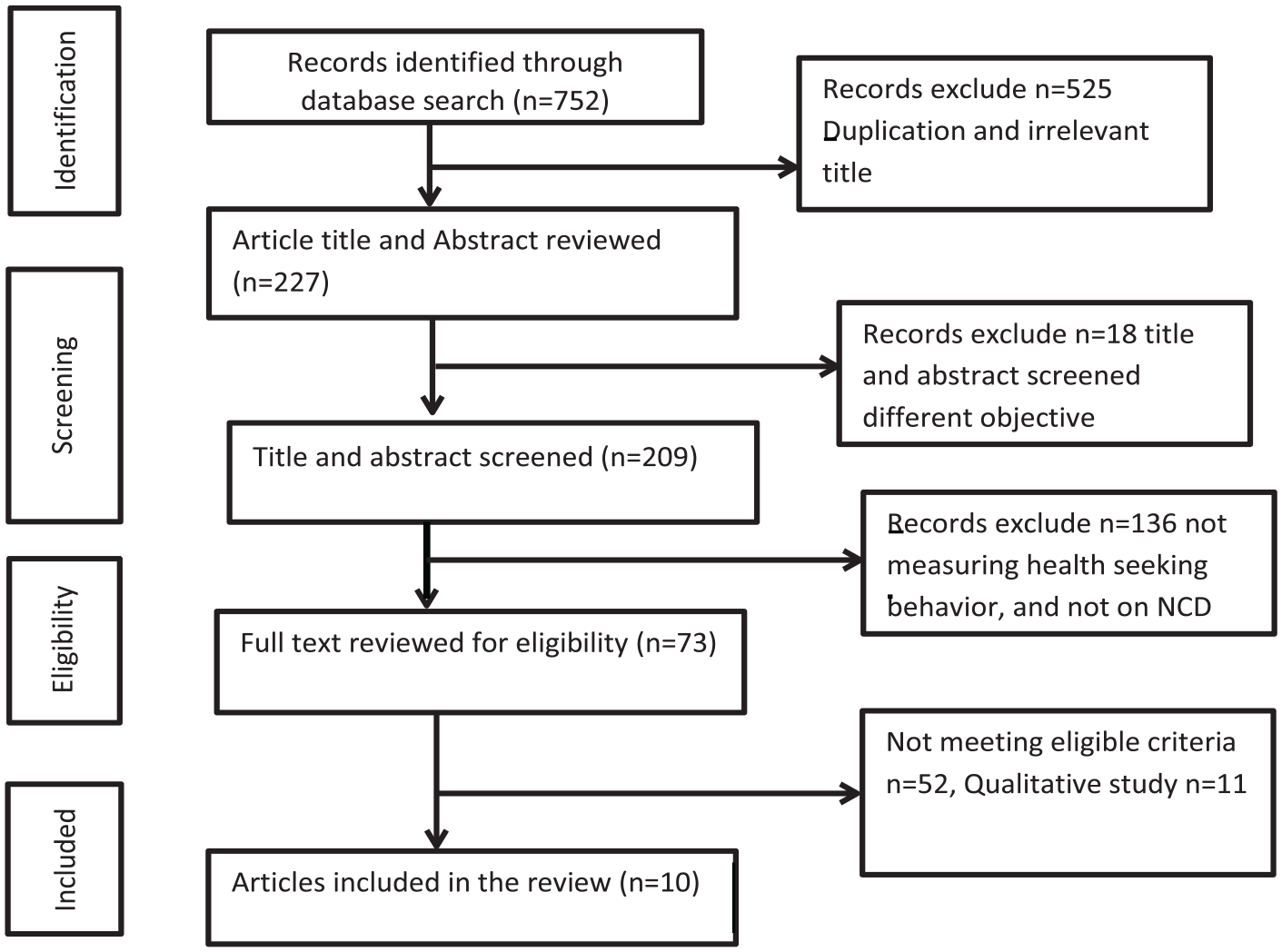
Preferred reporting items for systematic review and meta-analysis.
The search strategies were conducted by combining keywords using AND/OR Boolean terms “Health-seeking behavior,” “Health care utilization,” “health seeking,” “non-communicable disease” both in medical subject heading and free text terms.
The protocol for this systematic review and meta-analysis is registered in International Prospective Register of Systematic Reviews (PROSPERO) and obtained a registration number CRD42023432616.
Inclusion and exclusion criteria
Cross sectional study, cohort study, and case study that report health-seeking behavior on NCD were included. Studies conducted both at community and facility levels were included. Publication year from 2018 to up-to-date and English language were other inclusion criteria. Exclusion criteria were language other than English, duplicated articles and not measuring proportion of health-seeking behavior for non-communicable disease. The search was conducted from May 30 to 15 June 2023. Two authors (TFA and ETF) independently conducted the search and screened the studies based on the title and abstract at the initial steps. In the next step, both authors selected for full text based on eligibility criteria independently. In case of disagreement, the two authors’ disagreements were resolved by the decision of the third author (EKB).
Study quality assessment
The quality assessment of the studies included in this systematic review and meta-analysis were done using Newcastle-Ottawa scale (NOS). 14 This tool has ten points with three domains of modified NOS components for observational studies.The studies which have a score ⩾5were included. 14 Quality assesment was done independantly by two authors and in case of disagreement, a third author checked for the quality and consensus was reached by the third author’s decision (Table 1).
Quality assesment using modified NOS for observational studies included in this systematic review and meta analyis, 2023.

Y= Yes; N = No
Selection of the study
The articles were initially selected based on the study’s objectives and screening based on their titles and abstracts. In the second step, the articles that did not meet the inclusion requirements were eliminated. After this, the eligible articles were further screened by reading the full texts, and those that did not meet the inclusion criteria were excluded. Finally, the eligible full-text articles that fulfilled the inclusion criteria were included in the review.
Data extraction
Data were extracted on a Microsoft Excel spreadsheet from the included studies. Information was extracted based on the studies’ characteristics: name of first authors, publication year, study settings, sample size, and proportion of health-seeking behavior. Also, information was extracted based on characteristics of participants such as age, sex, and type of disease.
Statistical analysis
Data analysis was conducted using STATA version 17 (Stata Corp., College Station, TX, USA). A random effect model meta-analysis was employed to estimate the pooled proportion of health care seekers. The heterogeneity among effect sizes of the included studies was evaluated using the Q test results with a significance difference of p < 0.1 and a I2 static value >75%. 13 Potential publication bias was assessed by a funnel plot. The reasons why patients were not seeking health care from health facilities were summarized using qualitative thematic analysis.
Results
Out of 752 records obtained through electronic database, only 10 articles met the inclusion criteria and were included in this review. After duplicate records were removed, 227 records were reviewed by title and abstract. Seventy-three were included for full text review. Finally, ten studies were included in the review after applying inclusion and exclusion criteria (Figure 1).
Characteristics of study included in the review and meta-analysis
From ten articles included, eight15–18,20,22–24 were community-based cross-sectional studies while two19,21 were health facility-based cross-sectional studies. The total study participants recruited in the study was 63,498 adults with NCDs. The smallest sample size of the included studies was 100 study participants 19 and the largest one 45,151 (Table 2). 16
Characteristics of included studies on health-seeking behavior for non-communicable disease systematic review and meta-analysis, 2023.

Pooled prevalence of Health-seeking behavior for non-communicable disease
The pooled prevalence of health-seeking behavior for NCDs among adults globally was 56% with (95% CI: 44–68). Based on tau square (between-studies variance), tau = 2482.89 and I2 = 99.64% with p value < 0.005 which indicates there is statistically significant heterogeneity among studies (Figure 2).

Forest plot of the pooled prevalence of health-seeking behavior for non-communicable disease worldwide.
Publication bias
The funnel plot shows the symmetric distribution of effect size against the standard error that is evidence for no publication bias and the Egger test p = 0.6269 also revealed it (Figure 3).
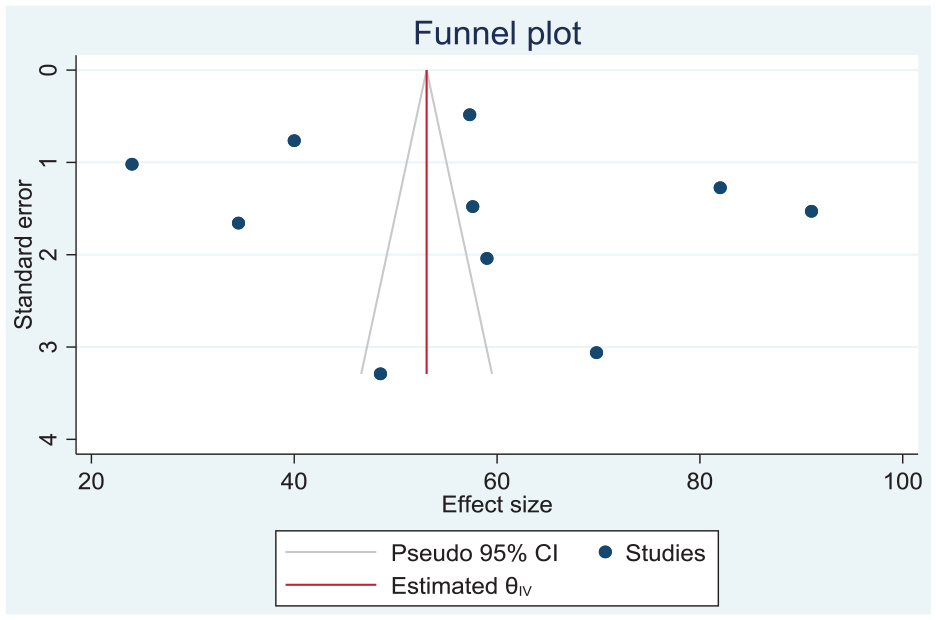
Funnel plot to cheek publication bias of studies included in the review and meta-analysis.
Subgroup analysis based on publication year
The subgroup analysis based on publication year shows there is difference in health-seeking behavior for non-communicable disease from time to time. The highest prevalence 67% (95% CI: 30–104) was observed during the year 2023 and the lowest prevalence 50% (95% CI: 36–65) during the year 2022 for health-seeking behavior for NCDs among adults worldwide (Figure 4).
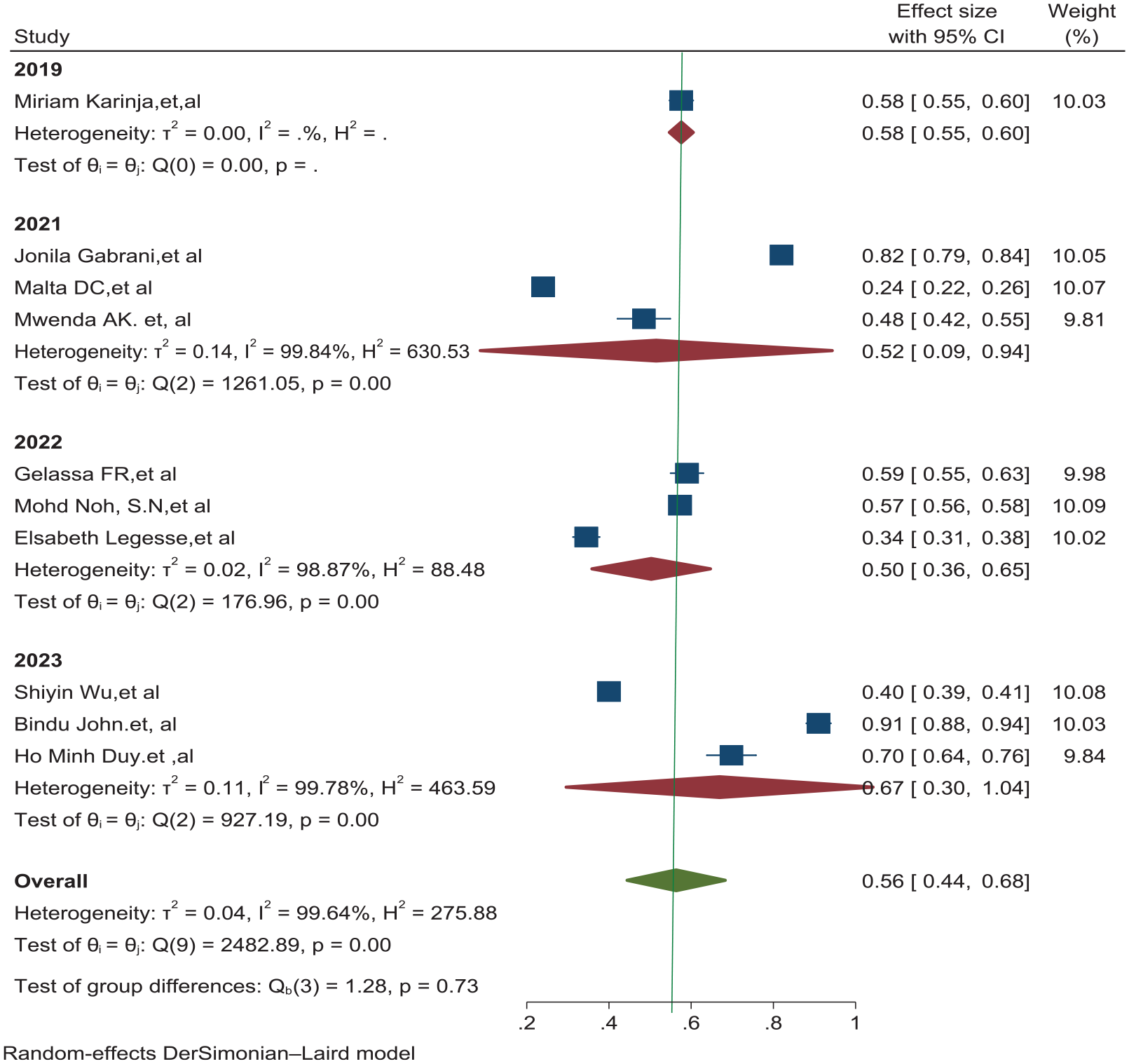
Subgroup analysis based on publication year on health-seeking behavior for non-communicable disease worldwide.
Subgroup analysis based on study setting
The subgroup analysis based on study setting indicates there is difference in health-seeking behavior for NCDs. The highest prevalence 67% (95% CI: 28–111) was observed in the study setting based on health facility and lowest was community-based prevalence 53% (95% CI: 41–65) of health-seeking behavior for NCDs among adults worldwide (Figure 5).

Subgroup analysis based on the study settings used for health-seeking behavior for non-communicable disease worldwide.
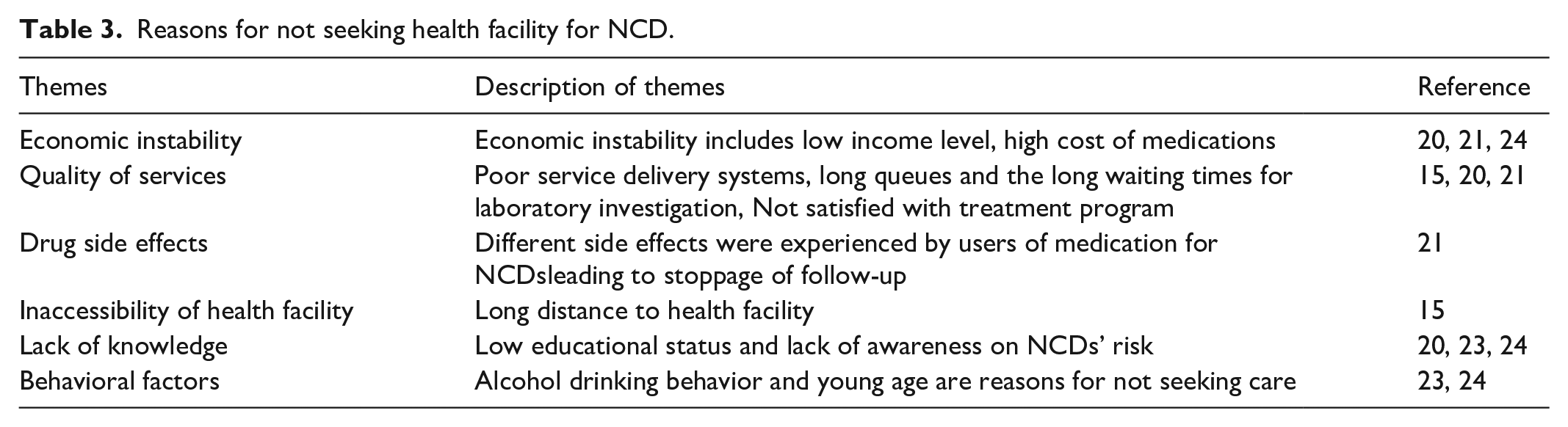
Reason for not having health-seeking behavior
Low educational status, rural residency, low economic status, young age, lack of health insurance, being male, lack of support during treatment, alcohol consumption and lack of knowledge on NCD risk factors were contributing factors for not having health-seeking behavior for NCD (Table 3).
Reasons for not seeking health facility for NCD.
Factors associated with health-seeking behavior for non-communicable disease
This meta-analysis identifies different factors associated with health-seeking behavior for non-communicable diseases worldwide. Among these are older age > 60,15,17 having hypertension OR urban residency, 15 being female gender, 17 Educational status high school and above,17,23 getting support during treatment, being hospitalized in the past, alcohol consumption, 20 being government employed, perceived as having good health status, 22 presence of NCD in the family members, knowledge of NCD risks, having more than one NCD, presence of health insurance, needing health care counseling, and economic class being middle and upper. 24
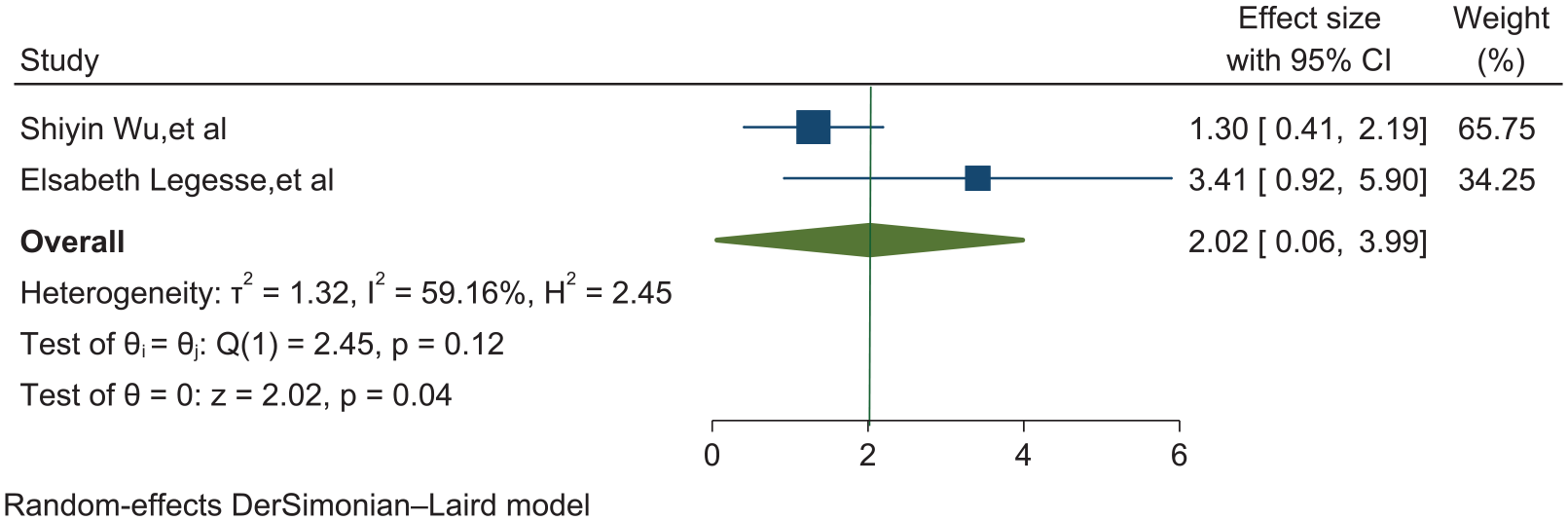
Association of educational status and health-seeking behavior
This meta-analysis provided evidence that adults who had educational status of high school and above were significantly associated with health-seeking behavior for NCDs with adjusted odds ratio (AOR = 2.02, 95% CI: 0.06–3.99). This implies that educational status of high school and above was two times more likely to promote health-seeking behavior for NCDs compared with those who had educational status of illiterate (Figure 6).
Association of educational status and health-seeking behavior for non-communicable disease.
Association of age and health-seeking behavior
This meta-analysis provided evidence that the study participants of age greater than 60 years were significantly associated with health-seeking behavior for NCDs at health facility with adjusted odds ratio (AOR = 1.03, 95% CI: 0.09–1.96). This indicates that adults of age > 60 years were 1.03 times more likely to seek care for NCDs compared to adults aged 18–59 years (Figure 7).

Association of age and health-seeking behavior for non-communicable disease.
Discussion
Understanding health-seeking behavior is important to tackle the emerging threats and premature death from NCDs.25,26 In the world there are few studies that determine health-seeking behavior for NCDs. This systematic review and meta-analysis was performed to produce pooled estimates of the worldwide magnitude of health-seeking behavior for non-communicable disease and associated factors among adults with NCD globally.
In this systematic review and meta-analysis data, a total of 63,498 adults with NCD from ten studies were pooled to estimate the proportion of health-seeking behavior from health facilities.
In this review, the pooled proportion of health-seeking behavior from health facilities were 56%(95% CI: 44–68). These findings were in lined with review done in Ethiopia. 27 This implies that only half of adults with NCDs engaged in health-seeking behavior, which encourages stakeholders and policy makers to direct their efforts to promote the society’s health by creating demand, and promoting innovative methods for NCD health-seeking behavior.
NCD patients who were getting support from family members had good health-seeking behavior. This is in line with the study done in the pacific region and India.28,29 The possible reason might be that patients getting family support helps them to remember their follow-up date and there is also a possibility of getting economic support to cover their medical expenses.
NCD patients who had experience of hospitalization in the previous year had positive health-seeking behavior. This study is in line with studies done in Ethiopia and Zimbabwe.25,27 This might be due to the patients’ experience of hospitalization giving them more awareness on the consequences of NCDs.
NCD patients with higher economic status had better health-seeking behavior. This is in line with studies done in Zambia, the pacific region and India.25,27–29 The possible explanation might be good economic status helps individuals being able to afford medication cost.
Educational status of elementary and above, older age and knowledge of NCD was significantly associated with health-seeking behavior. This might be because older age patients and educated people have greater awareness on NCDs’ risk factors and seriousness of the disease.
The common reasons and contributing factors for not seeking health care from health facility for NCD were low educational status, rural residency, low economic status, young age, lack of health insurance, support during treatment, alcohol consumption and lack of knowledge on NCD risk factors. These findings were comparable with review done in middle- and low-income countries and in Pakistan26,30,31 which found reasons for delay in seeking care from health facility were low educational status and low economic status.
This review revealed that being of young age groups was one of the barriers for health-seeking behavior. This is similar with a study done in Bangladesh. 32 This might be due to that younger age groups were not having sufficient knowledge on risk factors and consequences of NCDs.
The subgroup analysis by publication year demonstrates that the pooled proportion of health-seeking behavior for NCDs increase from time to time that is highest at 67% (95% CI: 30–104, I2 = 99.78) by 2023 and also subgroup analysis by study setting revealed there is high variation in health facility-based study at 67% (95% CI: 28–111, I2 = 99.27) compared to community-based study at 53% (95% CI: 41–65, I2 = 99.62). The possible justification might be that health facility-based study participants might have higher probability of reporting positive health-seeking behavior. The heterogeneity remained high in both groups which suggests more uniform effects of studies for the behavior across the world. Overall, we found high heterogeneity across the studies, which might be due to different study settings, data collection techniques and instruments, study participants and sample size.
The main strengths of this systematic review and meta-analysis were conducting random effect model to address heterogeneity among different studies included in the review and sub group analysis that was done to explore potential sources of heterogeneity. This review is not out of limitation studies included in the review use different measurement tools that might introduce bias.
Conclusion
Health-seeking behavior has a significant effect on prevention and control of NCD by initiating early screening, treatment and follow-up, contributing toward a reduction of premature death by NCD. This review revealed that globally, only half of adults with NCDs engage in health-seeking behavior from health facilities. This results in a significant impact on global health systems and causes a high rate of premature death. There are several contributing factors for low health-seeking behavior worldwide. Some of these include lack of social support, low economic and educational status, alcohol consumption, lack of health insurance and lack of knowledge about NCD. Therefore, policy makers and concerned stake holders should give emphasis for promotion of health-seeking behavior.
Supplemental Material
sj-docx-1-smo-10.1177_20503121231215236 – Supplemental material for Health-seeking behavior among non-communicable disease patients globally, systematic review and meta-analysis
Supplemental material, sj-docx-1-smo-10.1177_20503121231215236 for Health-seeking behavior among non-communicable disease patients globally, systematic review and meta-analysis by Tadele Fentabil Anagaw, Elyas Melaku Mazengia, Eyob Ketema Bogale, Eneyew Talie Fenta, Habitu Birhan Eshetu, Natnael Kebede, Sintayehu Shiferaw Gelaw, Amare Zewdie and Tadele Derbew Kassie in SAGE Open Medicine
Footnotes
Acknowledgements
We acknowledge all authors who contributed for the success of this review.
Authors’ contribution
All authors made a significant contribution to the work reported, whether it be in the conception, data extraction, quality control, analysis and interpretation of results and preparation of the manuscript. Critically reviewing the manuscript and giving final approval of the version to be published, all authors have agreed on the journal to which the article has been submitted and agree to be accountable for all aspects of the work.
Availability of data
All data generated and analyzed during this review were included in the published article as supporting file.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical clearance
Not applicable.
Consent for publication
Not applicable.
ORCID iDs
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.