
Abstract
Intestinal parasitic infections are the major public health problem globally, mostly in developing countries. World Health Organization recommends deworming to all at-risk people living in endemic areas as a prevention or intervention strategy. Therefore this study aimed to assess the deworming coverage and its predictors among Ethiopian children aged 24-59 months. The study analyzed retrospectively cross-sectional data on a weighted sample of 5,948 children aged 24-59 months nested within 645 clusters after extracting from the Ethiopian Demographic health survey. Bivariable and multivariable logistic regression was employed to assess the association of variables. Predictors at p-value < 0.25 were entered into the multivariable logistic regression model, and statistical significance was declared at P-value < 0.05. In this study, the prevalence of maternal reported deworming supplements among children aged 24-59 months was 15.1%. Predictive variables significantly associated with deworming supplementation include maternal media exposure, maternal control of household healthcare decisions, institutional healthcare delivery, and child vitamin-A supplementation. Having history of a diarrheal disease, maternal and paternal education, and family size were also statistically significant predictors of deworming supplements. Therefore, deworming supplementation among children is low. Maternal education and employment, paternal education, family size, decision-making process, maternal media exposure, place of delivery, vitamin-A supplementation, and a having history of diarrhea were predictors of deworming supplements. Multifaceted interventions aimed at those predictors should be given emphasis.
Introduction
Intestinal parasitic infections are remaining the major public health problems affecting 3.5 billion people globally and 450 million were ill as a result of these infections, the majority being children. The majority of parasites are concentrated in developing countries mainly in sub-Saharan Africa. It is estimated that more than 10.5 million new cases are reported annually and the commonest intestinal parasites are Ascaris lumbricoides, hookworms, Trichuris trichiura, Giardia lamblia, Entamoeba histolytica, and Schistosomas. 1 A systematic review and meta-analysis conducted in Ethiopia showed that the pooled prevalence of intestinal parasites among pre-school and school children was 48% which ranged from 42% to 53%. 2
According to a World Health Organization (WHO) report, over 270 million pre-school and over 600 million school children live in areas where the parasites are intensively transmitted and need treatment and preventive interventions. 3 Globally, the mean global deworming coverage in pre-school children was estimated at 36% in 50 soil-transmitted helminths (STH)-endemic countries between 2004 and 2017. The sub-national coverage ranged from 0.5% to 87.5%, and within-country variation was greater than between-country variation in coverage. 4 In 2009, over 300 million preschool and school-age children were dewormed in endemic countries, corresponding to 35% of the children at risk. The global target is to cover at least 75% of these at-risk children. 5
Under-5 years of age children are more prone to intestinal parasites because of their weak immunity and also habitually they play in fecal contaminated soil that needs special care and follow-up. 6 Risk factors for these infections include poor personal hygiene, lack of sanitation, and low socioeconomic status. This factor makes most developing countries to be affected. In most of the developing countries, more than half the population have poor sanitation, with the countries with the lowest coverage concentrated in Sub-saharan Africa and Southern Asia. 7
Intestinal parasites cause significant morbidity and mortality in endemic countries. They can produce a wide range of symptoms including intestinal manifestations (diarrhea, abdominal pain), general malaise, weakness, and chronic intestinal blood loss that result in anemia. It can also impair the nutritional status in many ways, sometimes causing death due to intestinal bleeding, diarrhea, or dysentery. It can also cause loss of appetite and reducing the absorption of micronutrients (gastroenteropathy) which contribute to impaired gut immune function and oral vaccine failure. Additionally, they can cause complications that require surgical intervention like intestinal obstruction and rectal prolapse. Moreover, concomitant infections with other parasite species are frequent and may have additional effects on nutritional status and organ pathology. Apart from the above effects, they also affect physical growth and cognitive development leading to poor school performance and absenteeism in children, reduced work productivity in adults, and adverse pregnancy outcomes.8-10
Preventive chemotherapy (deworming) is an important part of a comprehensive package to eliminate morbidity due to soil-transmitted helminths in at-risk populations. Evidence shows that preventive chemotherapy, or the periodic large-scale administration of anthelminthic medicines to populations at risk, can dramatically reduce the burden of worms caused by soil-transmitted helminth infections. 11
WHO recommends deworming without a previous individual diagnosis to all at-risk people living in endemic areas. This intervention reduces morbidity by reducing the worm burden. 8 It is recommended to all children living in endemic areas once a year when the prevalence of soil-transmitted helminthic infections in the community is over 20%, and twice a year when the prevalence of soil-transmitted helminthic infections in the community is over 50%. A recent meta-analysis indicates that deworming leads to improvements in appetite which results in gaining extra weight, height, mid-upper arm circumference, and skinfold thickness. 5
Ethiopia has been launching selected deworming programs to control intestinal parasitic infections among preschool-age children to reduce their morbidity and mortality. 12 Despite the presence of selective deworming drugs for under-5 children and the promotion of health education through health extension workers, intestinal parasitic infections are the leading cause of morbidity and mortality. This is impeding the efforts to achieve sustainable development. 13 Little has been known about deworming and its predictors among under-5 children. This study aims to assess deworming coverage and its predictors among Ethiopian children aged 24 to 59 months.
Methods
Data Source and Study Subjects
This study used the dataset of children included in the Ethiopian Demographic Health Survey (EDHS) 2016. EDHS is part of the international Demographic and Health Survey program (DHS), led by the United States Agency for International Development (USAID), in collaboration with other organizations and host countries. 14
In Ethiopia, the DHS has been conducted every 5 years since 2000. The latest survey was conducted in 2016. 15 The full data set of EDHS 2016 is available and accessible on the DHS program website: http://dhsprogram.com/data/dataset/Ethiopia StandardDHS 2016.cfm. The survey was designed to be representative at both national and regional levels. 15 Children 24 to 59 months of age, with deworming supplementation level record, were included in this work.
Sample Size and Sampling Methodology
EDHS 2016 followed a stratified, two-stage cluster design in sample selection. Census enumeration areas (EAs) were the primary sampling units. The sample included 645 EAs (202 urban and 443 rural). The secondary sampling units were households. In the second stage of sampling, a fixed number of 28 households were selected from each cluster (EAs), by systematic random sampling. More information about the methodology of EDHS 2016 can be found in the report of the main findings of the survey. 2 All children in the selected households were included and data were collected on various health and nutrition variables, including deworming supplementation for children aged 6 to 59 months. This work was focused on children aged 24 to 59 months because deworming as a supplement in the Ethiopian context is mostly given for children above 24 months of age. As a result data extraction was done only for those children aged 24 to 59 months. Finally, the total weighted sample size was 5948 children (Figure 1).

Flow chart of sample selection.
Study Variables
Outcome variable: The outcome variable was deworming supplementation. It is a binary outcome variable and coded as 0 if the child didn’t take deworming supplementation and coded as 1 if the child took deworming supplementation.
Independent variables: The selection of the independent variables was guided by the literature and availability of the variable in the DHS dataset. The variables were categorized into 3 groups: household, maternal, and child healthcare-related factors.
Household factors: Place of residence, family size, number of under-five children within the household, household wealth index, and decision-maker of household on health care utilization.
Maternal factors: Maternal age, marital status, religion, education status, and current occupation. Antenatal care (ANC) visits, postnatal care, and nutritional counseling were not incorporated in the final model because of having a missing value of greater than 10%.
Child factors: Sex, age, birth order, having a history of diarrhea 2 weeks preceding the survey, and vitamin-A supplement use 6 months preceding the survey.
Statistical Analysis
The analysis was done taking into account the complex design of the survey; such that the estimates provided were done based on the weighted data and taking into account the cluster design of the study. Sample weights were applied to compensate for the unequal probability of selection of study participants by region of residence.
Small regions were oversampled to ensure data representativeness at regional levels. Thus, following the DHS methodology, sample weights were applied to ensure the data resembles the national population distribution. A detailed explanation of the sampling weighting procedures can be found in the EDHS 2016 report. 15
Bi-variable logistic regression analysis was done to evaluate the relation of each independent variable with deworming supplementation. Variables with P < .20 in the bi-variable analysis were included in the final regression analysis. Statistical significance of a variable was declared at P ≤ .05 in the final multivariable logistic regression. All data analyzes were conducted using STATA version 14. Model fitness was assessed using a Hosmer and Lomeshow chi-square test and it was P = .342, which shows the model was fit. The model classification was 85.1%.
Results
Socio-Demographic Characteristics of Study Participants
The mean (±SD) age of mothers (years) and children (months) were 30.3(±6.4) and 41.6(±10.4), respectively. More than two-thirds (69.4%) of mothers were not attended formal education. The majority (89.5%) of study participants were from a rural residence. Near to half (48.5%) of households were from the poor wealth index category (Table 1).
Socio-Demographic Characteristics of Study Participants Among Ethiopian Children Aged 24-59 Months.

Single, divorced, widowed, separated.
Healthcare-Related Characteristics of Study Participants
More than three-fourth (79.9%) of study participants gave birth at home for the index child, and less than one-third of mothers (31.5%) had media exposure. Only 15.1% of children supplemented with deworming prior to the survey. More than half (55.3%) of children did not take VAS 6 months before the survey (Table 2).
Maternal and Child Health Care Related Characteristics Among Ethiopian Children Aged 24-59 Months.

Factors Associated with Deworming Supplementation
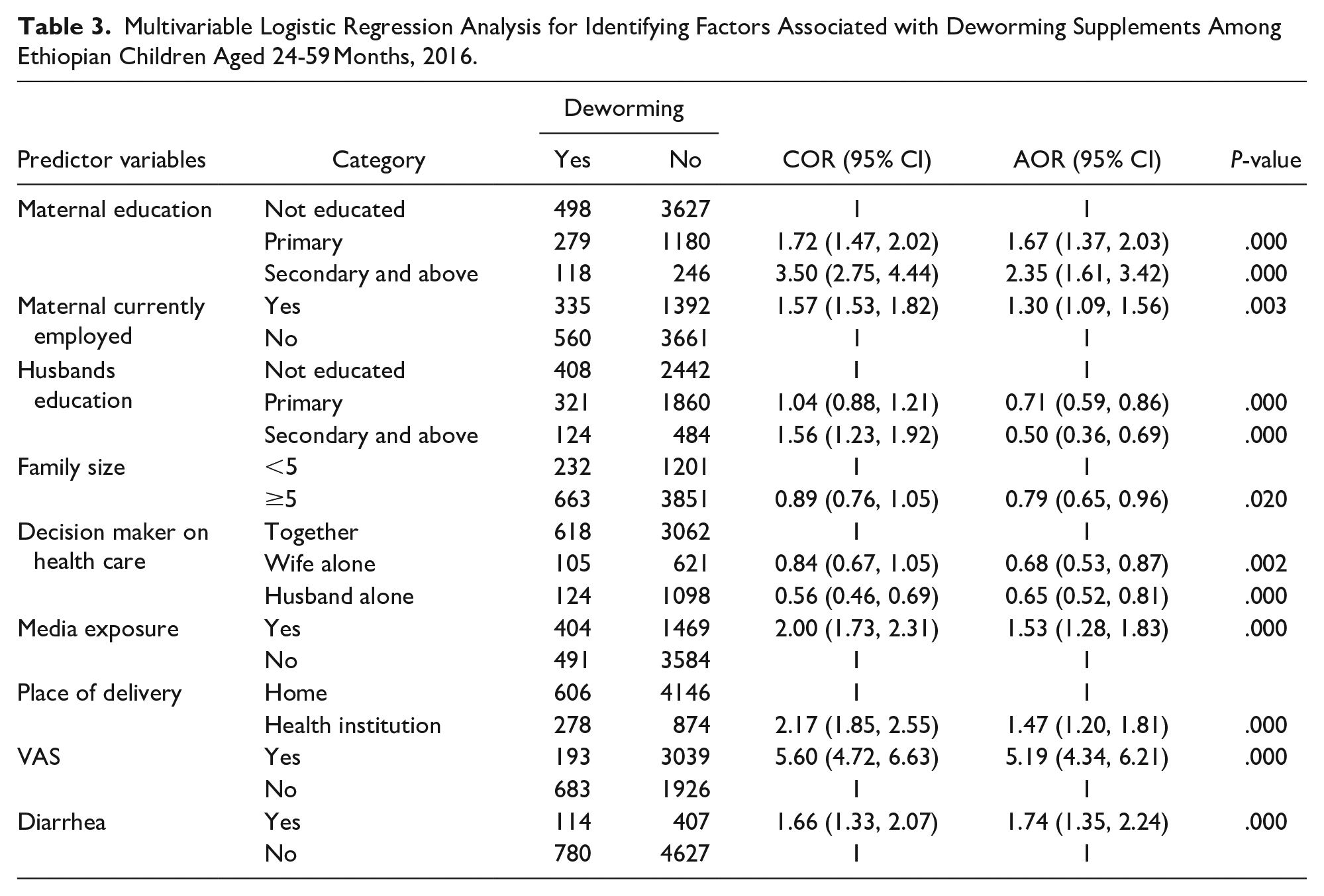
Predictor variables that showed statistically significant association at binary logistic regression at P-value <.20 were considered for the final multivariable logistic regression model. In this final model maternal education and current employment status, paternal education, family size, decision-making process on healthcare-related issues, media exposure, place of delivery, VAS, and a having history of diarrhea 2 weeks before the survey were found to be statistically significant predictors of child deworming supplements (Table 3).
Multivariable Logistic Regression Analysis for Identifying Factors Associated with Deworming Supplements Among Ethiopian Children Aged 24-59 Months, 2016.
Discussion
This study showed that the prevalence of deworming supplementation among children aged 24 to 59 months was 15.1% (95% CI: 14%, 16%). This finding was lower than a study conducted in Nigeria, in which periodic deworming among pre-school children was 42%. 16 It is also lower than a national deworming coverages of Burundi, Myanmar, and the Philippines in which 80.1%, 93.6%, and 75.7% of children were received deworming supplementation, respectively. 17 A study conducted in Zambia revealed that the health campion deworming coverage rate in 2012 was 93.4%, which is higher than this finding. 18 It is also lower than a study conducted in Kenya in which 19.6% of children get deworming supplements. 19 The possible discrepancies in those findings might be the difference in socio-demographic characteristics, sample size, and difference in population and study settings.
This study revealed that children whose mothers attended secondary and above, and primary level of education were more than 2 times and 67% more likely to get deworming supplementation than children whose mothers didn’t attend formal education, respectively. This finding was in line with a study conducted in Ghana. 20 This could be as mothers’ educational level increases her knowledge and practice towards child healthcare practice will be improved.21,22
This study showed that children whose mothers were employed at the time of the survey were 30% more likely to receive deworming than their counterparts. This finding was supported by a study done in Ghana, which revealed that employed mothers were more likely to utilize deworming for their children relative to unemployed mothers. 20 The employment rate might depend on education 23 and exposure to the importance of supplements. 24
In addition, this study also revealed that paternal education is found to be negatively associated with childhood deworming, unlike other studies in which paternal education status is supportive for child healthcare practices. 25 Children whose fathers attend secondary and above, and primary level of education were 50% and 29% less likely to get deworming supplementation than children whose fathers didn’t attend formal education, respectively. This might be explained by when fathers are more educated they will give emphasis to their job and even pass their time at work far from their family, by which they might not have time caring for their children.
Moreover, children from households having a family size of 5 and more were 21% less likely to take deworming supplements. As family size increases they deserve more attention and need more time. As a result, it might be difficult to fill all the needed care for children. Regarding the decision-making process on healthcare, children from only paternal and only maternal decision-makers were 35%, and 32% less likely to take deworming supplements than children from family’s whose paternal and maternal decide together. The influence of women’s autonomy on the use of health care appears to be an important determinant.26-30
This study also showed that children whose mothers had media exposure were 53% more likely to get deworming supplementation. This is consistent with a study done in Nigeria that showed that maternal media exposure increases maternal awareness of healthcare. 31 It was also supported by another study done in India, which showed that media exposure increases maternal health service utilization. 32 The possible explanation might be those mothers who had media exposure might get health education about the importance of deworming supplementation, by which maternal attitude, knowledge, and practice will be improved.
In this study children who were delivered at health-institutions were 47% more likely to receive deworming supplementation. This finding was supported by a study conducted in Kenya in which the place where caregivers seek health services (district hospital versus other health institutions), are significant predictors for deworming supplementation. 19 This might be mothers who get birth at the health institutions might get health education about the importance of deworming supplementation.
Furthermore, children who received vitamin A supplementation (VAS) 6 months before the survey were more than 5 times more likely to receive deworming supplementation. This could be VAS and deworming supplements are provided integratively both in terms of program logistics and added health impact. 33 Another explanation could be mothers who are aware of the importance of VAS might be more likely to be aware of deworming supplementation.
Children having a history of a diarrheal disease 2 weeks prior were 74% more likely to get deworming tablets. The possible explanation might be, intestinal parasites might cause diarrheal disease and they might get treatment for worms and by which more likely to get counseling services regarding deworming supplementation.
Conclusions
The magnitude of deworming supplementation among children aged 24 to 59 months was lower than global deworming programs aim to reach 75% of at-risk preschool-age children by 2020.34,35 This study revealed that the predictors for child deworming supplementation are multifactorial. Therefore public health interventions should aim to increase deworming coverage, which decreases the tropically neglected intestinal parasitosis burden, by considering those factors.
Footnotes
Acknowledgements
Special thanks goes to EDHS program for providing the data set.
Author’s Contributions
GFM conceptualized and designed the study. GFM, FWF and SSA performed the analysis, and interpreted the result. All the authors wrote and revised the manuscript jointly, and approved the final submission of the study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval and Consent to Participate
The data sets are extracted from EDHS 2016. The ethical approval and consent form of is stated in the EDHS 2016.
Availability of Data and Materials
The datasets generated and/or analyzed during the current study are available from the corresponding author on reasonable request.