
Abstract
Objectives:
Over the last decades, large number of children living with human immunodeficiency virus (HIV) have been successfully enrolled in care and initiated treatment. However, treatment failure is still a major challenge in the track, missing far too many children. National-level evidence on antiretroviral therapy failure and its associated factors among children receiving highly active antiretroviral therapy is required to alleviate this challenge.
Methods:
PubMed/Medline, EMBASE, CINAHL, Cochrane library, Google, and Google Scholar databases were used to access eligible studies. This meta-analysis was reported according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses guidelines. In addition, Newcastle–Ottawa Scale quality assessment was applied for critical appraisal. Cochran’s Q statistic, funnel asymmetry plot, and Egger’s test were used to assess heterogeneity and publication bias. Random effect model was computed to explore the pooled burden of treatment failure and its associated factors among children living with HIV. Odds ratio with 95% confidence interval was considered to identify associated factors.
Result:
The overall pooled prevalence of treatment failure among children living with HIV was 16.6%. Whereas virological, immunological, and clinical failure were 4.49%, 5.41%, and 5.71% respectively, where either of parent is deceased (odds ratio = 2.13, 95% confidence interval: 1.4–3.3), opportunistic infection (odds ratio = 1.67, 95% confidence interval: 1.1–2.5), absence of disclosure of status (odds ratio = 1.6, 95% confidence interval: 1.0–2.5), advanced World Health Organization stage (odds ratio = 4.2, 95% confidence interval: 1.6–10.5), and drug substitution (odds ratio = 2.0, 95% CI: 1.5–2.7) were significantly associated factors.
Conclusion:
The pooled prevalence of treatment failure among children living with HIV in Ethiopia was lower when compared to most African countries. Accordingly, either prevention or early treatment of opportunistic infection and advanced World Health Organization clinical stages, special care for children whose either parents are deceased, advocating disclosure of status, and avoiding drug substitution as much as possible were still needed to prevent treatment failure.
Introduction
Globally, there is remarkable progress toward controlling the HIV pandemic, yet we are still missing far too many children living with HIV. 1 Children are increasingly getting infected at alarming rates, and consequently, dying from Acquired Immune Deficiency Syndrome (AIDS). Nearly 150,000 new HIV infections were recorded among children aged under 15 years in 2019 (four times higher than 2018 targets), of which more than 70% found in Sub-Saharan Africa (SSA). 2 Approximately every minute and half, a child is newly infected with HIV, bringing the total number of children living with HIV to 2.8 million. 3
Approximately 5% of all people living with HIV, 9% of new HIV infections, and 14% of all AIDS-related deaths occur among children. 4 A review of existing evidence showed that nearly 8% of all deaths among children on highly active antiretroviral therapy (HAART) occurred in SSA. 5 East and Southern Africa share the largest burden of children with HIV infection, with around 1.1 million children living with HIV. 6 Treatment coverage among children globally is extremely low, only 53% of the estimated 1.8 million children were found on treatment in 2019, 7 while in Eastern and Southern Africa regions, only 58% pediatric HAART was recorded. 8
In Ethiopia, large number of children living with HIV have been successfully enrolled in care and initiated on HAART. 9 However, treatment failure remains a challenge, when there is virological, immunological, and clinical failure, resulting in emergence of opportunistic infections (OIs). Some barriers lead to treatment failure including weak monitoring of the quality of interventions, limited linkage of positive clients, loss to follow-up, low data quality, and gaps in use of program data. 10 Treatment failure can be detected either clinically, immunologically, or virologically. According to global evidence, treatment failure among children living with HIV was significant and highest in low- and middle-income countries, particularly in Latin America and SSA. 11 Treatment failure leads to the use of second-line antiretroviral drugs, which in turn leads to higher patient costs, limited treatment options and success of therapy, increased risk of HIV transmission, and drug toxicity. All these issues call for action at the community level.12,13
In Ethiopia, treatment failure among children living with HIV ranges from 7.7% 14 to 23.8%. 15 In order to provide evidence for national policy makers, the national-level pooled evidence on treatment failure and its associated factors among children living with HIV is mandatory. Therefore, this is the first review aimed at, first, finding the pooled burden of HIV treatment failure among children living with HIV in Ethiopia, and second, reviewing those factors that contribute to this burden of treatment failure at national level. The findings from this study will inform health care professionals and provide important evidence to health policy makers and implementers, and play a great role in achieving HIV/AIDS targets.
Methodology
Reporting and searching strategies
This systematic review and meta-analysis was reported based on the Preferred Reporting Items for Systematic Reviews and Meta-Analyses Protocols (PRISMA) guidelines 16 (Supplemental Appendix 1). At first, studies related to our topic were searched using major medical electronic databases such as PubMed/Medline, EMBASE, Cochrane library, Web of Science World Health Organization’s (WHO) Hinari portal (which includes the SCOPUS, African Index Medicus, and African Journals Online databases), and Google Scholar. In addition, cross references of identified studies, academic institution online library and websites, and local shelves were used to access additional studies and gray literatures. The key terms such as burden, prevalence, magnitude, treatment failure, virological, immunological, clinical, ART, HAART, HIV, AIDS, children, children under-15 years, young population, associated factors, determinants, predictors, risk factors, causes, and Ethiopia with their appropriate medical searching heading terms (MeSH) were used to search eligible studies. In addition, Boolean operators “OR” and “AND” were used to combine these words. Finally, EndNote citation manager software (version X7; Thomson Reuters, New York, NY) was used to manage duplications. The search was conducted and completed on 2 January 2021.
Inclusion and exclusion criteria
This systematic review and meta-analysis included all observational studies (cross-sectional, case control, and cohort) which reported either prevalence of treatment failure, virological failure, immunological failure, and clinical failure and/or factors associated with treatment failure among children living with HIV; studies published in English language and conducted in Ethiopia. There was no restriction placed on study design, setting, study year, and publication year. Full texts of eligible studies were also examined. Articles which could not be accessed in their full format at the time of search process were excluded after contact was attempted with the principal investigator through email at least two times. Studies which did not report outcome of interest were excluded. In addition, studies deemed to be of poor quality as per settled criteria of reviewing the articles were excluded from the final analysis.
Data extraction procedure
Joanna Briggs Institute Reviewers’ Manual 2014 17 was used to develop the data extraction format on Excel spreadsheet. The prepared spreadsheet format includes author(s) name(s), publication year, study area, study design, sampling technique, mean age, sample size, and prevalence of overall treatment failure, virological failure, clinical and immunological failure among children living with HIV. In addition, cross tabulations were computed to evaluate the association between treatment failure and common factors listed in the included studies (such as age, sex, disclosure, parent status, weight for age, WHO status, CD4 count, OI, drug adherence, and drug substitution).
Quality appraisal
After duplicate studies were excluded using Endnote, two independent reviewers critically appraised studies using Newcastle–Ottawa Scale (NOS) quality assessment adapted for observational studies18,19 (freely accessed). Generally, NOS quality assessment tool have 10 scales. Only studies that scored NOS 6 and above were considered for final analysis. Differences or disagreement between reviewers were resolved by discussion and consensus. Where a consensus could not be reached, a third reviewer was engaged. Then, the average score of the two reviewers was applied for final inclusion. In addition to this, risk of bias in the studies was assessed and evaluated using the 10-item rating scale developed by Hoy et al. 20 Sampling, data collection, reliability and validity of study tools, case definition, and prevalence periods were included in the tool. For each article, responses from the rating scale were categorized as having low risk of bias (“yes” answers to domain questions) or high risk of bias (“no” answers to domain questions). Each study was assigned a score of 1 (yes) or 0 (no) for each domain, and these scores were summed to provide an overall study quality score. Scores of 8–10 were considered as having a “low risk of bias”; 6–7, a “moderate risk”; and 0–5, a “high risk.”
Outcomes measurement
The main aim of this meta-analysis was to pool the national-level burden of treatment failure of children living with HIV in Ethiopia either using overall treatment failure, or virological failure, or immunological failure or clinical failure. In addition to this, this meta-analysis was also aimed at evaluating the effect of common factors such as age, sex, disclosure, parent status, weight for age, WHO status, CD4 count, OIs, drug adherence, and drug substitution on treatment failure among children living with HIV.
Statistical analysis
STATA version-14 was used for further data analysis. Cochran’s Q statistic with inverse variance (I 2 ) was used to assess the existence of statistical heterogeneity and to quantify it. The Der Simonian Laird random-effects model was employed to estimate the overall prevalence. Low, moderate, and high heterogeneity were considered at 25%, 50%, and 75%, respectively. 21 In addition, a p value less than 0.05 was used to confirm the presence of heterogeneity across studies. Publication bias was assessed using Egger’s regression test 22 and funnel plot asymmetrical visualization. The estimated pooled burden of treatment failure and its associated factors among children living with HIV was presented using forest plot diagram with their corresponding 95% confidence interval (CI) and odds ratio (OR). In addition, subgroup analysis was also computed using study region, design, and mean age to explore those potential sources of heterogeneity across primary studies. The potential factors listed above were also analyzed.
Results
Explanation of original studies
The initial search included a total of 789 studies. Then, 712 articles were excluded because of duplication. Of the 77 studies screened, 65 were excluded due to irrelevancy. Finally, seven14,15,23– 27 complete studies were critically appraised using NOS for final analysis after five articles were removed due to their inconsistent outcomes with our objectives (Figure 1).

PRISMA flow diagram of studies included to estimate pooled burden of treatment failure among children living with HIV in Ethiopia.
Of the included studies, three were from Amhara regional state,14,26,27 two from Addis Ababa23,24 and the remaining were from Tigray region 15 and Oromo region. 25 All included studies have been published on internationally known journals from 2012 to 2020 and were conducted using retrospective cohort except one cross-sectional study. A total of 3628 under-15-years-old children living with HIV and on HAART were included in this meta-analysis (Table 1).
Descriptive characteristics of seven studies included in this meta-analysis of pooled prevalence of treatment failure among children living with HIV in Ethiopia.

AA: Addis Ababa; VF: virological failure; IF: immunological failure; CF: clinical failure; TF-treatment failure; Syrs: systematic random sampling; SR: simple random; NOS: Newcastle–Ottawa scale.
Meta-analysis
Treatment and immunological failure among children living with HIV in Ethiopia
A total of seven studies14,15,23– 27 were included to estimate the overall treatment failure among children living with HIV in Ethiopia. Accordingly, the pooled burden of treatment failure among children living with HIV was 16.6% (95% CI: 12.09–21.1). However, this meta-analysis showed a significant heterogeneity across the included studies as evidenced with I 2 = 80%, p < 0.001 (Figure 2). Whereas relatively symmetrical visualization of funnel plot (Supplemental Additional file-1) and non-significant Egger’s test (p = 0.102) exclude presence of publication bias. Furthermore, to pool the burden of immunological failure among children living with HIV in Ethiopia, a total of seven primary studies14,15,23– 27 were considered. The meta-analysis of these studies showed that, a total of 5.41% (95% CI: 3.2–7.6) children living with HIV were diagnosed with immunological failure in Ethiopia (Figure 2). This meta-analysis showed significant heterogeneity across included primary studies (I 2 = 74.6% and p = 0.001). The symmetric visualization of funnel plot (Supplemental Additional file-2) and non-significant Egger’s test (p = 0.307) confirmed the absence of publication bias.

Forest plot of the pooled prevalence of treatment and immunological failure among children living with HIV in Ethiopia.
Virological and clinical failure among children living with HIV in Ethiopia
In a similar manner, a total of five primary articles14,15,24– 26 were used to estimate the pooled burden of virological failure among children living with HIV in Ethiopia. The average pooled prevalence of these studies revealed that 4.49% (95% CI: 2.09, 6.89) of children living with HIV were confirmed cases of virological failure. The forest plot revealed the presence of heterogeneity across included studies (I 2 = 85.1%, p < 0.001) (Figure 3), whereas the symmetrical visualization of funnel plot (Supplemental Additional file-3) and non-significance Egger’s test (p = 0.120) confirmed the absence of publication bias.

Forest plot of the pooled prevalence of virological and clinical failure among children living with HIV in Ethiopia.
Furthermore, this meta-analysis also used five primary studies14,23,25,27 to estimate the pooled prevalence of clinical failure among children living with HIV in Ethiopia. Based on the analysis of these studies, 5.71% (95% CI: 3.24, 81.18) of children living with HIV were showed clinical failure (Figure 3). The forest plot showed the presence of moderate heterogeneity across included studies (I 2 = 65.9%, p = 0.02) while the symmetrical visualization of funnel plot (Supplemental Additional file-4) and non-significant Egger’s test (p = 0.388) evidenced the absence of publication bias.
Subgroup analysis
According to subgroup analysis, the regional prevalence of treatment failure was 23% in Tigray, around 18% in Addis Ababa and Oromo, and 12.7% in Amhara regional state. The pooled prevalence of treatment failure among cross-sectional studies was 18% and 16.4% according to the analysis of retrospective cohort studies. In addition to this, the pooled prevalence of treatment failure among children living with HIV younger than mean age of 7 was 11.3% while nearly 20% for children older than mean age of 7 (Table 2).
Subgroup analysis which describes pooled prevalence of treatment failure among children living with HIV in Ethiopia.

AA: Addis Ababa.
Factors associated with treatment failure among children living with HIV
In addition to estimating the pooled burden of treatment failure among children living with HIV in Ethiopia, this meta-analysis also explored the association between common factors such as age, sex, parent status, disclosure, weight for age, WHO stage, CD4 T-cell count, OI, drug adherence, and drug substitution with treatment failure. Only parent status, disclosure status, WHO stage, OIs, and drug substitution were found to be significantly associated with treatment failure.
In order to evaluate the effect of parent status on treatment failure of children living with HIV, three primary studies15,25,26 were included. In accordance, children living with HIV whose either parent is deceased were two times more likely to have treatment failure when compared to their counterparts (OR = 2.13, 95%, CI: 1.38–3.28) (Figure 4).

Forest plots which describe association between maternal age, parent status, weight for age, disclosure status, and WHO stage, and treatment failure children living with HIV in Ethiopia.
In addition, the odds of treatment failure among children living with HIV who had no disclosure on their status14,15,23– 25 was 1.64 times higher when compared to their counterparts (OR = 1.64, 95% CI: 1.07–2.53) (Figure 4). Furthermore, children living with HIV and diagnosed with WHO stage 3 and 4 15 , 23 – 26 were 4.9 times higher to have treatment failure than their counterparts (OR = 4.9, 95% CI: 1.67–10.55) (Figure 5). Moreover, the odds of treatment failure among children living with HIV who had OIs14,15,25 was 1.7 times higher than their counterparts (OR = 1.67, 95% CI: 1.12–2.49). Once more, children living with HIV who had drug substitution history14,15,23,25 were 2.02 times more likely to be diagnosed with treatment failure when compared to their counterparts (OR = 2.02, 95% CI: 1.520–2.69) (Figure 5).
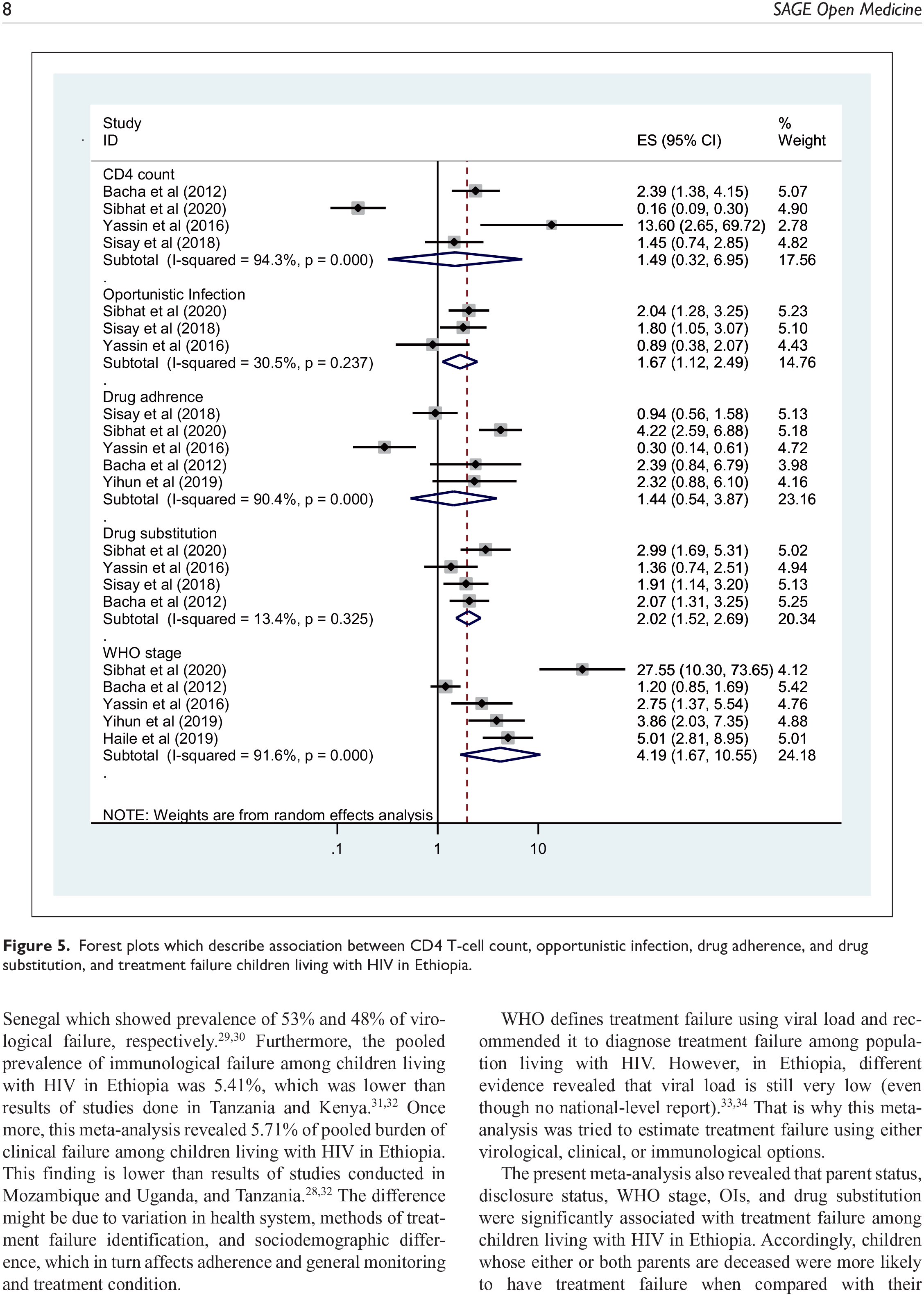
Forest plots which describe association between CD4 T-cell count, opportunistic infection, drug adherence, and drug substitution, and treatment failure children living with HIV in Ethiopia.
Discussion
This systematic review and meta-analysis was conducted to investigate the pooled burden of treatment failure and its associated factors among children taking HAART in Ethiopia, not yet investigated at national level. A total of 3628 children living with HIV and seven primary studies were included to explore the pooled prevalence of treatment failure among children living with HIV in Ethiopia. Accordingly, the overall pooled prevalence of treatment failure among children living with HIV in Ethiopia was 16.6%. This implicated that only encouraging children living with HIV is not enough, and giving attention to implementation of treatment failure prevention activities is important in Ethiopia. This finding is lower than an observational study done in Mozambique and Uganda, which reported 29% of prevalence of treatment failure. 28
In addition to this, the present review and meta-analysis also revealed a pooled burden of 4.49% virological failure among children living with HIV in Ethiopia. This figure is much lower than findings of studies done in Cameroon and Senegal which showed prevalence of 53% and 48% of virological failure, respectively.29,30 Furthermore, the pooled prevalence of immunological failure among children living with HIV in Ethiopia was 5.41%, which was lower than results of studies done in Tanzania and Kenya.31,32 Once more, this meta-analysis revealed 5.71% of pooled burden of clinical failure among children living with HIV in Ethiopia. This finding is lower than results of studies conducted in Mozambique and Uganda, and Tanzania.28,32 The difference might be due to variation in health system, methods of treatment failure identification, and sociodemographic difference, which in turn affects adherence and general monitoring and treatment condition.
WHO defines treatment failure using viral load and recommended it to diagnose treatment failure among population living with HIV. However, in Ethiopia, different evidence revealed that viral load is still very low (even though no national-level report).33,34 That is why this meta-analysis was tried to estimate treatment failure using either virological, clinical, or immunological options.
The present meta-analysis also revealed that parent status, disclosure status, WHO stage, OIs, and drug substitution were significantly associated with treatment failure among children living with HIV in Ethiopia. Accordingly, children whose either or both parents are deceased were more likely to have treatment failure when compared with their counterparts. Similar finding was reported in Cameroon. 30 This might be related to the fact that losing parents or appropriate caregiver may cause psychological depression or impairment, which may impact adherence. Those children might also vulnerable to malnutrition and late HAART initiation with more advanced immunodeficiency and exposed to loss to follow up in turn increased viral load and risk of OIs that further deteriorate the immunity.
Similarly, advanced WHO clinical stage (III/IV) was significantly associated with treatment failure, supported with results in Mozambique and Uganda, and Tanzania.28,35 This increased risk of disease progression could further impair the positive effects of the HAART on immune cells and may encounter burden of two diseases treatment; HIV/AIDS and the advanced stages, more likely to experience side effects. 11
Disclosure of status was another important determinant in this study. Children who did not know their HIV status were more likely to be failed from their treatment regimens when compared with children insured their status. This study is supported by similar finding reported in Tanzania. 36 Disclosure of status is positively associated with better social support, stronger family and relationship cohesion, and reductions in anxiety and depression. This leads to improvements in physical health, emotional support, and financial support which leads to HAART adherence. But, in the absence of disclosure, the inverse is true. 37
Children who had OIs were at higher risk of treatment failure than their counterparts. This might be due to when the immunity compromised due to OIs and the virus itself, the chance of the patient to control the virus in the body is too low and as a result, the first regimen of HAART cannot control the infections. 14 The patient is likely to give attention to those secondary infections, which in turn may cause interruption of drug taking and loss of follow-up. OIs bring a very conducive environment for the HIV virus. 28
Furthermore, children who had drug substitution history were more likely to be diagnosed with treatment failure when compared with their counterparts. Our finding of a higher risk of first-line treatment failure in children who had drug substitution is consistent with a study conducted in Malawi. 12 Administering a new drug to the patient is mostly associated with new side effects until usual adaptation and response happened, which in turn influence the adherence and treatment condition on HAART.
Limitation of the study
Regardless of the study’s strengths and the inevitable intrinsic limitations of using systematic review and meta-analysis, more limitations were noted. The use of clinical and/or immunological criteria to diagnose treatment failure in some primary studies due to the absence of viral load testing was a limitation. Most of the included studies were conducted using retrospective cohort, difficult to identify the cause and consequence (example in case of advanced WHO stage and OIs). In addition, this meta-analysis did not include all regions and administrative cities of the country. Therefore, further country-based and prospective studies to assess the effect of factors including other than patient-related factors such as health service factors, health policy factors, and health caregiver–related factors are recommended.
Conclusion
Generally, this meta-analysis revealed a high (but lower than most African countries reports) pooled prevalence of treatment failure among children living with HIV in Ethiopia. Having either or both parents deceased, on advanced WHO clinical stage, presence of OIs, non-disclosure of HIV status, and presence of drug substitutions were the contributing factors of HIV treatment failure. The findings of the present study will have great impact on the current health policy and therapeutic management decisions for HIV/AIDS clinical practice. In addition to this, this report of the burden of treatment failure will be used to monitor the national action plan progress of 90-90-90 strategies in Ethiopia.
Supplemental Material
sj-docx-1-smo-10.1177_20503121221081335 – Supplemental material for Treatment failure and its associated factors among children receiving highly active antiretroviral therapy in Ethiopia: A systematic review and meta-analysis
Supplemental material, sj-docx-1-smo-10.1177_20503121221081335 for Treatment failure and its associated factors among children receiving highly active antiretroviral therapy in Ethiopia: A systematic review and meta-analysis by Temesgen Getaneh, Ayenew Negesse, Getenet Dessie, Melaku Desta, Moges Agazhe Assemie, Agimasie Tigabu, Kihinetu Gelaye, Addisu Alehegn Alemu and Sarah Lebu in SAGE Open Medicine
Supplemental Material
sj-docx-2-smo-10.1177_20503121221081335 – Supplemental material for Treatment failure and its associated factors among children receiving highly active antiretroviral therapy in Ethiopia: A systematic review and meta-analysis
Supplemental material, sj-docx-2-smo-10.1177_20503121221081335 for Treatment failure and its associated factors among children receiving highly active antiretroviral therapy in Ethiopia: A systematic review and meta-analysis by Temesgen Getaneh, Ayenew Negesse, Getenet Dessie, Melaku Desta, Moges Agazhe Assemie, Agimasie Tigabu, Kihinetu Gelaye, Addisu Alehegn Alemu and Sarah Lebu in SAGE Open Medicine
Supplemental Material
sj-docx-3-smo-10.1177_20503121221081335 – Supplemental material for Treatment failure and its associated factors among children receiving highly active antiretroviral therapy in Ethiopia: A systematic review and meta-analysis
Supplemental material, sj-docx-3-smo-10.1177_20503121221081335 for Treatment failure and its associated factors among children receiving highly active antiretroviral therapy in Ethiopia: A systematic review and meta-analysis by Temesgen Getaneh, Ayenew Negesse, Getenet Dessie, Melaku Desta, Moges Agazhe Assemie, Agimasie Tigabu, Kihinetu Gelaye, Addisu Alehegn Alemu and Sarah Lebu in SAGE Open Medicine
Supplemental Material
sj-docx-4-smo-10.1177_20503121221081335 – Supplemental material for Treatment failure and its associated factors among children receiving highly active antiretroviral therapy in Ethiopia: A systematic review and meta-analysis
Supplemental material, sj-docx-4-smo-10.1177_20503121221081335 for Treatment failure and its associated factors among children receiving highly active antiretroviral therapy in Ethiopia: A systematic review and meta-analysis by Temesgen Getaneh, Ayenew Negesse, Getenet Dessie, Melaku Desta, Moges Agazhe Assemie, Agimasie Tigabu, Kihinetu Gelaye, Addisu Alehegn Alemu and Sarah Lebu in SAGE Open Medicine
Supplemental Material
sj-docx-5-smo-10.1177_20503121221081335 – Supplemental material for Treatment failure and its associated factors among children receiving highly active antiretroviral therapy in Ethiopia: A systematic review and meta-analysis
Supplemental material, sj-docx-5-smo-10.1177_20503121221081335 for Treatment failure and its associated factors among children receiving highly active antiretroviral therapy in Ethiopia: A systematic review and meta-analysis by Temesgen Getaneh, Ayenew Negesse, Getenet Dessie, Melaku Desta, Moges Agazhe Assemie, Agimasie Tigabu, Kihinetu Gelaye, Addisu Alehegn Alemu and Sarah Lebu in SAGE Open Medicine
Footnotes
Author contributions
T.G. developed the protocol and involved in the design, selection of study, data extraction, statistical analysis, and developing the initial drafts of the manuscript. A.N., M.D., and G.D. involved in quality assessment. T.G., A.N., G.D., M.D., A.T., M.A.A., K.G., and A.A.A. prepared and revised subsequent drafts as well as prepared the final draft of the manuscript. S.L. edited the overall language. All authors read and approved the final draft of the manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics approval and consent to participate
Not applicable.
Informed consent
Not applicable.
Consent for publication
Not applicable.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.