
Abstract
Although several scoring systems have been used to differentiate simple acute appendicitis from perforated appendicitis, no particular system has been widely accepted. Therefore, this study aimed to investigate preoperative factors associated with complicated appendicitis and to develop a scoring system that distinguishes complicated appendicitis in children aged <10 years. Patients aged <10 years who underwent surgical treatment for acute appendicitis between 2011 and 2019 were included in this study, after excluding those with insufficient medical records, with other diseases that affect the length of hospitalization, or without formal reports of abdominal computed tomography (CT) or ultrasonography (US). Complicated appendicitis was defined as hospitalization for ≥5 days postoperatively or readmission within 30 days postoperatively. Patient characteristics, symptoms, physical examination, laboratory data, and radiographic results were collected to determine predictors of complicated appendicitis. The mean age of 279 patients was 7.3 years. Among them, 57 patients had complicated appendicitis. A scoring system was developed based on the following 5 independent risk factors derived from multiple logistic regression analysis: body temperature, anorexia, diarrhea, C-reactive protein (CRP) level, and presence of periappendiceal free fluid on CT or US. The scoring system resulted in an area under the curve of .898 (P < .001). For patients aged <10 years, a new model that includes objective factors, such as body temperature, CRP levels, and radiography results, might help predict complicated appendicitis and determine treatment plans.
Introduction
The lifetime risk of appendicitis has been known to be 7% to 9%, with a peak incidence at 10 to 19 years age. 1 Acute appendicitis occurs less likely in younger patients, including preschoolers; however, its symptoms are often atypical with higher perforation and complication rates as compared to adults. 2 Following the trend of non-surgical management of acute uncomplicated appendicitis, several studies, including meta-analyses, have been conducted in pediatric patients.3,4 A recent guideline indicated that non-operative management for uncomplicated acute appendicitis in children was feasible, safe, and effective. 5 In order for non-operative treatment to be successful, un-complicated appendicitis should be distinguished from complicated appendicitis. Several studies have revealed risk factors for complicated appendicitis in pediatric patients.6-13 In addition, although some studies have suggested scoring systems to differentiate complicated and uncomplicated appendicitis,7,10,13 no scoring system has been widely accepted to date. Therefore, this study aimed to investigate preoperative factors associated with complicated appendicitis and to develop a scoring system that distinguishes complicated appendicitis in children aged <10 years.
Methods
Study Population
Patients aged <10 years who underwent surgical treatment for acute appendicitis between 2011 and 2019 at Inje University Sanggye Paik Hospital were included in this retrospective study. All patients underwent at least 1 of 2 radiographic studies: abdominal computed tomography (CT) or ultrasonography (US). Those without formal CT or US readings were excluded. Patients who underwent appendectomy >2 days after the imaging were excluded due to the possibility of mismatch between imaging test results and disease severity during surgery. Patients diagnosed with other diseases that prolonged hospital stay and with incomplete medical records were also excluded. Patients underwent laparoscopic or open appendectomy with intravenous antibiotic treatment during hospital stay. Patients were discharged when tolerating light diet, with normalized body temperature and white blood cell (WBC) counts.
Variables and Definitions
In order to classify patients with acute appendicitis into 2 groups according to disease severity, the length of postoperative hospital stay and readmission was used. Complicated appendicitis was defined as hospitalization for >5 days postoperatively or readmission within 30 days postoperatively. Perforated appendicitis was defined as a patient with documented perforation in the operation record.
Clinical features of the study population were collected through a medical record review. Data on age, sex, duration of symptoms, abdominal pain, anorexia, vomiting, diarrhea, body temperature, WBC counts, differential counts, prothrombin time, and C-reactive protein (CRP) level were selected and analyzed. Decreased oral intake was considered to be anorexia. The Alvarado Score, 14 Pediatric Appendicitis Score (PAS), 15 and Appendicitis Inflammatory Response (AIR) score 16 were calculated based on the collected data. The following radiological features were identified by reviewing formal CT or US reports: diameter of the appendix, presence and size of appendicolith, wall defects of the appendix, periappendiceal fluid collection, and extraluminal free air.
Statistical Analysis
Differences between categorical variables were analyzed using Pearson’s chi-square test, and continuous data were compared using Student’s t-test. Univariate analysis of each candidate for risk factors of complicated appendicitis was performed. The sensitivity, specificity, and area under curve (AUC) of the receiver operating characteristic (ROC) curve of each variable were calculated. For multivariate analysis, all variables with P-value of <.05 in univariate analysis were logged into logistic regression analysis with backward selection. The AUC of various scoring systems was compared using the ROC curve analysis.
Statistical significance was defined as P < .05. All statistical analyses were performed using Statistical Package for the Social Sciences 25.0 software (IBM, Chicago, IL, USA).
Ethical Approval and Informed Consent
The present study was approved by the Institutional Review Board Inje University Sanggye Paik Hospital (SGPAIK 2020-11-004), and the requirement for informed consent was waived.
Results
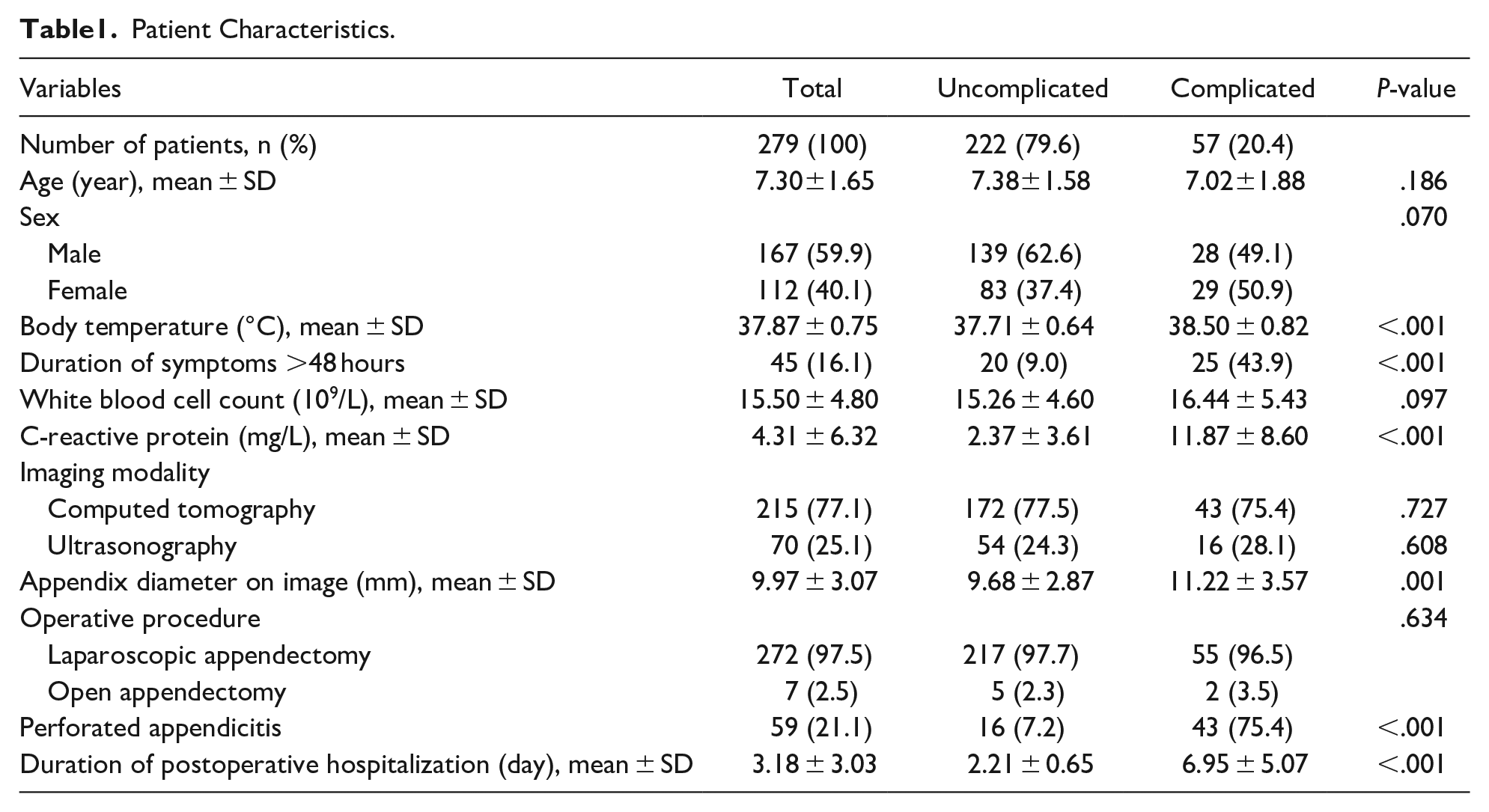
During the study period, 335 children aged <10 years underwent appendectomy for acute appendicitis. After excluding 56 patients according to the exclusion criteria, the remaining 279 patients were finally included in this study (Figure 1). Among them, 222 (79.6%) patients had uncomplicated appendicitis and 57 (20.4%) had complicated appendicitis. No significant differences were observed between the 2 groups according to the mean patient age, gender distribution, and surgical procedure (open vs laparoscopic appendectomy). Perforated appendicitis was more common in the complicated appendicitis group. A total of 10 patients in the complicated appendicitis group (17.54%) were readmitted; the causes of readmission were intra-abdominal abscesses (7 patients), ileus (2), and vomiting (1). Detailed characteristics of the study population are described in Table 1.

Flowchart of patient inclusion.
Patient Characteristics.
The association between various risk factors and complicated appendicitis was evaluated using univariate regression and ROC curve analyses. Table 2 shows the results of 12 predictors significantly associated with complex appendicitis, including odds ratio (OR), AUC, sensitivity, and specificity for each factor.
Univariate Analysis of Possible Risk Factors of Complicated Appendicitis.

Abbreviations: AUC, area under curve; CI, confidence interval.
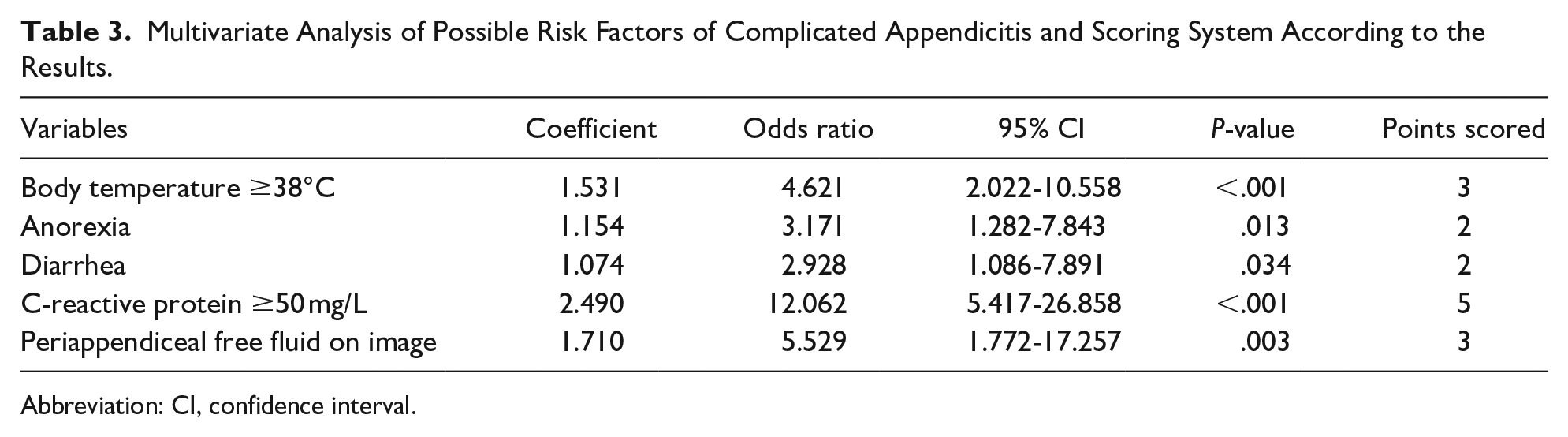
Multivariate logistic regression identified 5 variables associated with complicated appendicitis: body temperature of ≥38°C (OR = 4.621, P < .001), anorexia (OR = 3.171, P = .013), diarrhea (OR = 2.928, P = .034), CRP ≥ 50 mg/L (OR = 12.062, P < .001), and presence of periappendiceal fluid on radiography (OR = 5.529, P = .003). The AUC of this regression model was .896 (95% confidence interval [CI]: 0.852-0.941, P < .001). The integer closest to twice each coefficient was assigned as the weighted score for each variable. In this way, a new scoring system of up to 15 possible points was created to distinguish complicated from uncomplicated appendicitis (Table 3).
Multivariate Analysis of Possible Risk Factors of Complicated Appendicitis and Scoring System According to the Results.
Abbreviation: CI, confidence interval.
The total score of the new scoring system for the study population was calculated. Of 182 patients who scored ≤4 points, 9 patients (4.95%) had a false-negative result with complicated appendicitis, showing a negative predictive value (NPV) of 95.05%. For a cut-off value of 4 points, the scoring system showed 84.21% sensitivity, 77.93% specificity, 3.82 positive likelihood ratio, and 0.20 negative likelihood ratio. Table 4 shows the validity values of the scoring system according to each criterion, along with a 95% CI. The AUC for this new scoring system was .898 (95% CI: 0.856-0.931, P < .001) and was significantly higher than that of other known scoring systems (0.547 for Alvarado score, 0.571 for PAS, and 0.780 for AIR score) (all P < .05) (Figure 2).
Sensitivity and Specificity of the Scoring System with Various Criterion Values.

Abbreviations: CI, confidence interval; +LR, positive likelihood ratio; −LR, negative likelihood ratio.
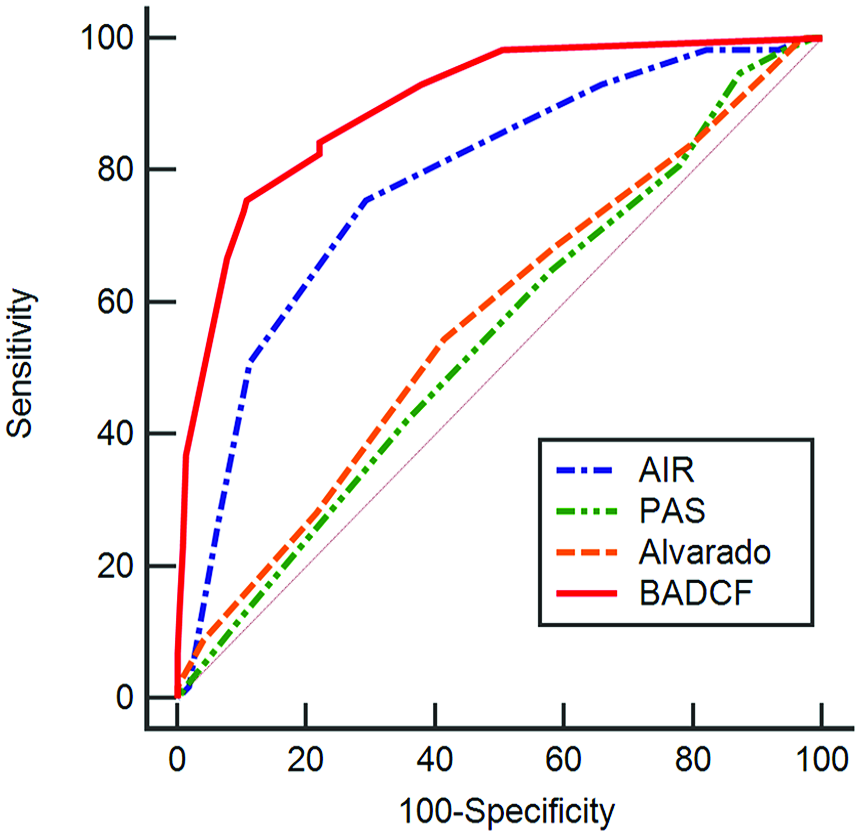
Comparison of the receiver operating characteristic curves for various scoring systems. Area under the curves: 0.780 for Appendicitis Inflammatory Response (AIR) score, 0.547 for Alvarado score, 0.571 for Pediatric Appendicitis Score (PAS), and 0.898 for the proposed scoring system (BADCF, named after the initial letters of 5 risk factors).
Discussion
Several studies have been conducted on the predictors of complicated or perforated appendicitis in children and adults.8-11,13,17-21 St Peter et al 22 defined perforated appendicitis as a hole in the appendix or fecalith in the abdomen according to a prospective randomized trial, which is the generally accepted definition. However, since this study was based on the incidence of postoperative intra-abdominal abscess after appendectomy and the definition did not include severe appendicitis without perforation, many studies defined ‘complicated appendicitis’ based on the surgical, pathological, or radiological findings to analyze predictors of advanced appendicitis that affected the prognosis and treatment plan of the disease. However, the definition of complicated appendicitis differed slightly for each study. Findings such as gangrenous appendicitis, phlegmon, purulent contamination in the abdominal cavity, or diffuse peritonitis were included or not included in the complicated appendicitis group in each study.6,9,11 However, these findings are relatively subjective factors that can be determined differently depending on the observer, and each factor has a wide spectrum of disease severity. In this study, 48.0% of patients (59 of 123) with turbid ascites or pus in the surgical record were discharged within 2 postoperative days without complications. Conversely, the length of hospital postoperatively and the occurrence of complications requiring readmission objective indicators that reflect disease severity. The mean duration of postoperative hospitalization of all patients was 3.18 days in this study. The number of patients discharged ≥5 days after appendectomy was 50, and the reasons for the extended hospital stay were reviewed. With multiple causes, persistent intraperitoneal drainage (16 patients) was the most common cause, followed by leukocytosis (15), delayed initiation of diet (15), fever (7), diarrhea (4), intra-abdominal abscess (3), wound infection (2), nausea or vomiting (2), EC fistula (1), and sepsis (1). Readmission, due to complications within 30 postoperative days, was observed in 10 patients: 7 due to intra-abdominal abscess, 2 due to mechanical ileus, and 1 due to vomiting.
This study aimed not to diagnose acute appendicitis in patients with acute abdominal pain, but to develop a new scoring system to help predict the prognosis and plan treatment for acute appendicitis diagnosed after a radiographic examination. The new scoring system consisted of 5 risk factors, including fever7,9,10,12,17,18 and CRP levels,12,17,19,20 found to be predictors of complicated appendicitis in many previous studies. CRP is generally recognized as a useful biomarker for predicting acute appendicitis in children. 5 Moreover, a higher CRP level was associated with severe acute appendicitis and a negative outcome in non-operative management in some studies.23-25
Physical findings, such as abdominal tenderness, rebound tenderness, and pain migration, were excluded from the current study. Tenderness and rebound tenderness might often be measured incorrectly in frightened or crying pediatric patients. In younger children, distinguishing and expressing symptoms, such as pain shifting, can be difficult. Conversely, diarrhea, vomiting, and decreased oral intake are indicators that can be easily observed.
Radiologic findings of the presence of periappendiceal free fluid were included in the scoring system. Van den Bogaard et al 12 and Atema et al 17 also reported that the presence of free fluid in images was significantly associated with complicated appendicitis in their multivariate analyses. Conversely, some studies revealed the presence of appendicolith in the image as a significant risk factor for complicated appendicitis.6,13,17 Appendicolith was significantly associated with complicated appendicitis in univariate analysis in this study but not in the multivariate analysis. Some studies have reported the presence of appendicolith as a risk factor for the failure of non-operative treatment for pediatric acute appendicitis.25,26 A recent guideline recommended non-operative management of children with uncomplicated acute appendicitis in the absence of appendicolith. 5 However, several studies on the usefulness of diagnosing complicated appendicitis using imaging tests in pediatric patients have found that US and CT have high specificity but relatively low sensitivity.27-29 Therefore, due to issues of misdiagnosis of complicated appendicitis based solely on radiographic findings, it was used in combination with other clinical values in the current study.
The AIR score showed a higher AUC than other widely used screening systems, such as Alvarado scores or PAS, in discriminating complicated appendicitis in this study. This seemed to result from the inclusion of CRP level and exclusion of symptoms that are difficult to distinguish in children, such as pain migration and nausea. 30 Williams et al 13 proposed a scoring system to diagnose ruptured appendicitis in children aged <18 years. However, in this study, the definition of ruptured appendicitis was not clearly described, and the CRP level was not analyzed. More recently, a scoring system, consisting of symptom duration, body temperature and absolute neutrophil count, for pediatric patients was reported by Bonadio et al 7 Although the authors defined perforated appendicitis based on CT findings, they excluded radiographic findings from their scoring system in order to use the scoring system as a screening test to determine whether to perform additional imaging tests and to differentiate complicated appendicitis. In addition, each risk factor was included in the scoring system without a weighted score according to different coefficients.
Considering the screening system for discriminating uncomplicated appendicitis to apply non-operative management, the cut-off value of 4 points had 77.93% specificity, indicating that 173 patients could be correctly identified as uncomplicated appendicitis among 222 uncomplicated appendicitis. The remaining 49 (22.07%) patients misclassified as complicated appendicitis could be surgically treated due to the exaggerated disease severity. However, compared to the burden of overtreatment including surgery for patients with uncomplicated appendicitis, the risk of missing the appropriate treatment timing is greater when patients with complicated appendicitis requiring surgical treatment are incorrectly identified as uncomplicated appendicitis. Therefore, in order to lower the risk of misclassifying complicated appendicitis as uncomplicated appendicitis using this scoring system and to maintain an NPV of >95%, 4 points were determined as the cut-off value. The optimal cut-off value calculated based on the Youden index was 6 points, and the specificity increased to 89.19%, whereas the NPV decreased to 93.4%. Based on this scoring system with a cut-off value of 4 points, appendectomy should be considered for patients with CRP of ≥50 mg/L (5 points) or patients with 2 or more risk factors.
In addition, the scoring system is associated with the length of hospital stay and complication rate after appendectomy. As a result of the partial correlation analysis, the correlation coefficient rho (r) with adjustment according to the type of surgery (laparoscopic or open appendectomy) was .561 (P < .001). Using this scoring system, patients with high preoperative scores can be predicted to have longer hospital stays after appendectomy. Readmission within 30 postoperative days after appendectomy showed a positive relationship with the score (r = .14, P = .015) and AUC of 0.721 (P = .004).
As a retrospective analysis, some limitations exist in this study. Emergency center and inpatient medical records were not standardized, and the data for some variables were missing. The intensity of rebound tenderness was not described in majority of emergency center records. As a result, the AIR score was derived by calculating the rebound tenderness as 1 point in all patients. In addition, since the formal CT or US readings were reported after appendectomy was performed in some patients, surgical findings might possibly influence the imaging interpretation. This study was based on data from a single center with the potential for selection bias, making it possible to maintain common surgical procedures and postoperative management protocols. The proposed scoring system did not include several factors identified as predictors of complicated appendicitis in many previous studies, such as the duration of symptoms6,8,10-13,17,18,20 and number of WBCs or neutrophils.8-10,12,13,17,19 These factors showed a significant association with complicated appendicitis in univariate analysis but not in multivariate analysis. In addition, proper external validation could not be performed for the scoring system. For the general application of the scoring system, appropriate external validation studies should be conducted. In spite of efforts to define of complicated appendicitis that reflects the disease severity and prognosis, limitations remained in the definition used in this study.
Nevertheless, the proposed scoring system has the advantage of being composed of 5 factors that can be objectively evaluated in children aged <10 years, who have difficulty expressing symptoms accurately or cooperating with physical examinations. In order to improve the accuracy of the scoring system, clinical information, such as symptoms and blood tests, and radiological test information were combined. Furthermore, the scoring system of the current study showed a high AUC of >0.85 within 95% CI, demonstrating a good capacity for distinguishing simple and complicated appendicitis.
In conclusion, objectively observable symptoms, such as nausea and diarrhea, and clinical factors, such as body temperature, CRP level, and presence of periappendiceal free fluid collection on radiologic examination, were significantly associated with complicated appendicitis in patients aged <10 years. A new model derived from these 5 factors might help predict the prognosis of children with appendicitis and determine treatment approach.
Footnotes
Author Contributions
Yujin Lee was primary author and contributed to study design, data analysis, data interpretation, and manuscript writing. Hyunjin Cho and Geumhee Gwak contributed to collection and interpretation of data. Byungnoe Bae contributed to study design, data collection, and manuscript revising. Keunho Yang was the primary editor and contributed to study design, data collection, data analysis, manuscript revision, and final approval as a corresponding author.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by a grant from research year of Inje University in 20140102.