
Abstract
Objectives:
This study aimed to develop and validate a nomogram prediction model for identifying the risk of early perforation (within 24 h) in patients with acute appendicitis, using objective clinical and imaging indicators.
Methods:
A retrospective study was performed on 880 patients with acute appendicitis who underwent laparoscopic appendectomy within 24 h of symptom onset at the General Surgery Department of the Central Theater Command General Hospital between January 2011 and December 2022. Patients admitted from 2011 to 2020 were assigned to the modeling group (n = 616), and those from 2021 to 2022 to the validation group (n = 264). Based on postoperative pathology, patients were classified as having early or non-early perforated appendicitis. Independent risk factors for early perforation were identified using LASSO and multivariate logistic regression and were used to develop a predictive nomogram. Model performance was assessed by the area under the receiver operating characteristic (ROC) curve (AUC) for discrimination and the Hosmer–Lemeshow test for calibration.
Results:
Appendiceal diameter, body temperature, white blood cell count, fibrinogen level, appendiceal fecalith, age, and diabetes mellitus were identified as independent predictors of early perforation in acute appendicitis within 24 h (p < 0.05). ROC analysis indicated that diameter (AUC = 0.673), temperature (AUC = 0.705), white blood cell (AUC = 0.713), fibrinogen (AUC = 0.742), and age (AUC = 0.759) had moderate predictive power. Incorporating fecalith and diabetes significantly enhanced model performance, yielding an AUC of 0.891.
Conclusion:
The nomogram prediction model incorporating appendiceal diameter, body temperature, white blood cell count, fibrinogen level, appendiceal fecalith, age, and diabetes mellitus demonstrates clinical utility in estimating the probability of perforation within 24 h in patients with acute appendicitis.
Introduction
Acute appendicitis is one of the most common causes of acute abdomen, with a lifetime risk of ~7%–8% globally. 1 Epidemiological data indicate that its annual incidence ranges from 91 to 110 cases/100,000 population, 2 and its specific etiology has not been elucidated. 3 The conventional pathophysiological understanding of acute appendicitis is based on the concept of time-related disease progression, 4 and treatment strategies are generally categorized into surgical and conservative approaches. While acute appendicitis carries a low mortality rate, complications such as perforation, abscess formation, and peritonitis remain frequent in cases of complicated appendicitis. 3 Recent studies suggest that non-operative management may be appropriate for patients with uncomplicated acute appendicitis, characterized by the absence of abscess or perforation, 5 evidence suggests that delaying surgery for up to 24 h or using antibiotic therapy does not increase the risk of complications or perforation in selected patients.6,7 However, based on clinical practice, we observed that a proportion of patients with uncomplicated acute appendicitis who underwent surgery within 24 h of symptom onset already had appendiceal perforation at the time of operation. These findings suggest that such patients would benefit from prompt surgical intervention, rather than delayed management or antibiotic therapy alone. One possible explanation for this distinct type of early appendiceal perforation is that it may represent a disease entity separate from non-perforated appendicitis. 8 Therefore, early clinical identification of such patients is crucial. Although symptom-based scoring systems may assist in predicting early perforation in acute appendicitis, they lack objectivity due to the inclusion of subjective components. Based on objective clinical variables, this study defined perforation occurring within 24 h of acute appendicitis onset as the primary endpoint. This study investigated the risk factors and potential predictors of appendiceal perforation occurring within 24 h of acute appendicitis onset, clinical indicators were employed after admission to differentiate patients with acute appendicitis and facilitate appropriate clinical management.
Methods
Study subjects
Patients diagnosed with acute appendicitis who were admitted to the Central Theater Command General Hospital between January 2011 and December 2022 were retrospectively enrolled. Patients admitted between January 2011 and December 2020 were assigned to the modeling group, while those admitted between January 2021 and December 2022 were assigned to the validation group.
Patients with a confirmed diagnosis of acute appendicitis who presented within 24 h of symptom onset and underwent emergency laparoscopic appendectomy were included. Based on postoperative pathological examination of appendiceal specimens, patients were categorized into two groups: the early perforated appendicitis (ePA) group and the early non-perforated appendicitis (eNPA) group.
Inclusion and exclusion criteria
Inclusion criteria: (1) Patients who underwent laparoscopic appendectomy after admission; (2) a diagnosis of acute appendicitis confirmed by postoperative pathological examination; (3) time from symptom onset to surgery <24 h.
Exclusion criteria: (1) Age <18 years; (2) presence of severe comorbidities involving other organ systems; (3) pregnancy; (4) patients who underwent other abdominal surgeries concurrently; (5) appendiceal tumor confirmed by postoperative pathology; (6) incomplete clinical data (see Figure 1).
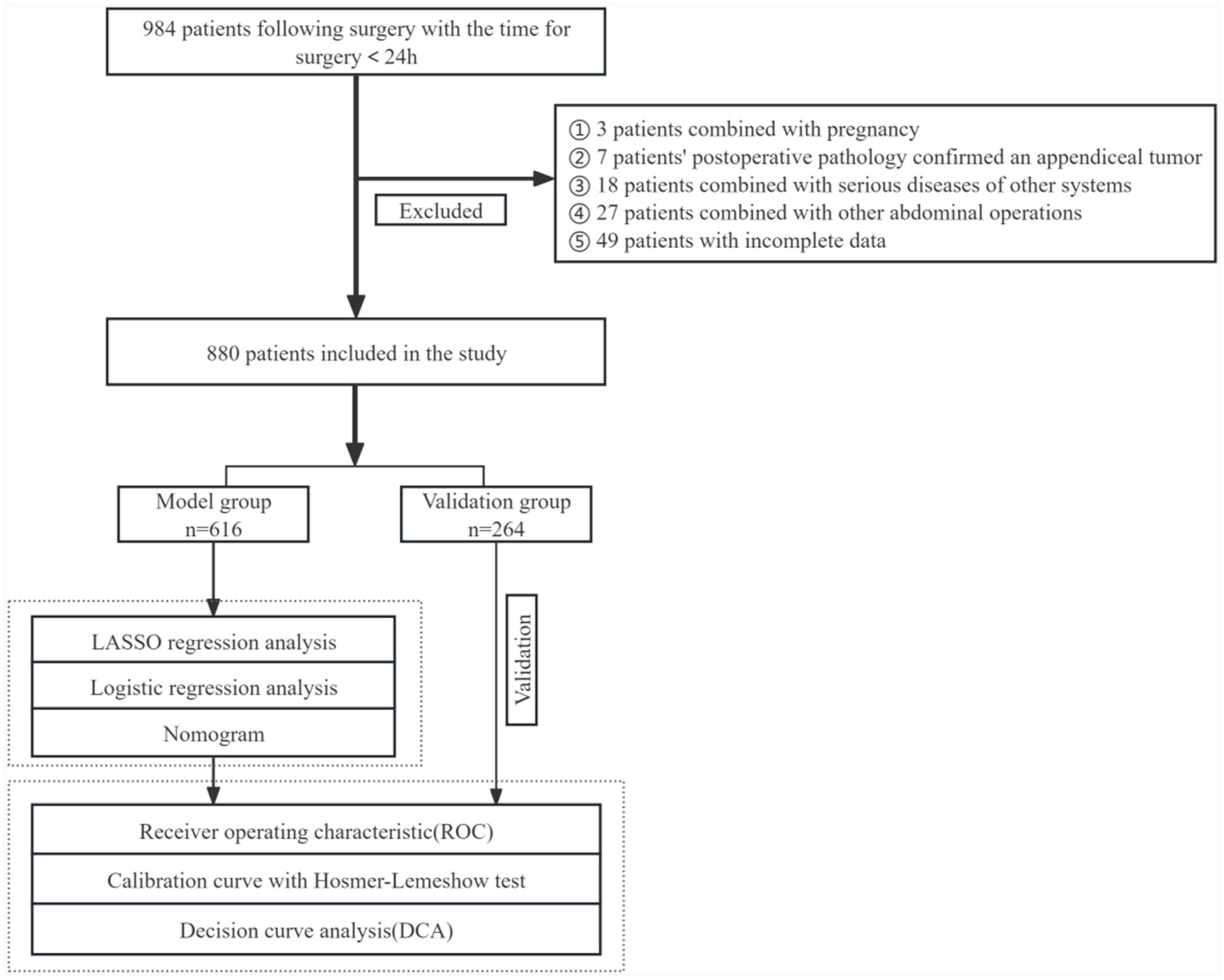
Flowchart of this study.
Clinical data collection and test methods
General information included gender, age, height, weight, body mass index, body temperature (Temperature), pulse rate (Pulse), duration time of symptoms (Time), and antimicrobial therapy prior to admission (Antimicrobial). Past medical history included previous episodes of acute appendicitis (Episodes) and prior abdominal surgery (Surgery). Laboratory tests included routine blood tests, coagulation profiles, and liver and kidney function tests. Imaging assessments included the presence of appendiceal fecalith (Fecalith), abdominal or pelvic effusion on preoperative CT (Fluid), and appendiceal diameter (Diameter), and pericecal fat stranding observed on preoperative CT (Fat). Pathological assessments were based on postoperative pathology reports. Imaging interpretations and pathological diagnoses were independently conducted by two physicians.
Statistical analysis
Statistical analysis was performed using R software (version 4.4.1; R Foundation for Statistical Computing, Vienna, Austria). Categorical variables were presented as counts and percentages (n (%)) and compared using the χ2 test. Continuous variables with a normal distribution were expressed as mean ± standard deviation (x̄ ± s) and compared using the t-test. Non-normally distributed data were expressed as median and interquartile range (M (P25, P75)) and compared using the Mann–Whitney U test (rank-sum test). Multivariate analysis was performed using stepwise backward logistic regression. The rms package in R was used to construct the regression model and generate the nomogram. Patient data from 2021 to 2022 were used for internal validation. The calibration and discrimination of the nomogram were assessed using the Hosmer–Lemeshow goodness-of-fit test and the area under the ROC curve, respectively. A two-sided significance level of α = 0.05 was applied, and p < 0.05 was considered statistically significant.
Results
General clinical characteristics of the study population
A total of 880 eligible patients were included in this study. The entire cohort was divided by admission year into a modeling group (n = 616) and a validation group (n = 264). There were no significant differences in baseline clinical characteristics, including demographic and biochemical parameters, between the two groups (p > 0.05; Table 1), indicating good comparability.
Comparison of clinical data between the modeling group and validation group.

Alb: albumin; ALT: alanine aminotransferase; APTT: activated partial thromboplastin time; AST: aspartate aminotransferase; BMI: body mass index; Cre: creatinine; FIB: fibrinogen; K: potassium ion; Lym: lymphocyte count; LymRatio: lymphocyte percentage; Na: sodium ion; Neu: neutrophil count; NeuRatio: neutrophil percentage; NLR: neutrophil-to-lymphocyte ratio; PLR: platelet-to-lymphocyte ratio; PT: prothrombin time; TB: total bilirubin; Ure: urea; WBC: white blood cell.
Appendiceal diameter.
Presence of fecalith.
Pericecal fat stranding observed on preoperative CT.
Abdominal/pelvic effusion.
Duration time of symptoms.
Antimicrobial therapy prior to admission.
Past medical history included previous episodes of acute appendicitis.
Past medical history included previous abdominal surgery.
Body temperature.
Pulse rate.
In the modeling cohort, 79 patients were classified into the ePA group and 537 into the eNPA group. Significant differences were observed between the two groups in white blood cell (WBC) count, neutrophil-to-lymphocyte ratio (NLR), neutrophil count, neutrophil percentage (NeuRatio), lymphocyte percentage, fibrinogen (FIB), total bilirubin, body temperature, appendiceal diameter, presence of fecalith, abdominal/pelvic effusion (Fluid), age, and diabetes (p < 0.05; Table 2).
Baseline characteristics of participants in NPA and PA set.

Alb: albumin; ALT: alanine aminotransferase; APTT: activated partial thromboplastin time; AST: aspartate aminotransferase; BMI: body mass index; Cre: creatinine; eNPA: early non-perforated appendicitis; ePA: early perforated appendicitis; FIB: fibrinogen; K: potassium ion; Lym: lymphocyte count; LymRatio: lymphocyte percentage; Na: sodium ion; Neu: neutrophil count; NeuRatio: neutrophil percentage; NLR: neutrophil-to-lymphocyte ratio; PLR: platelet-to-lymphocyte ratio; PT: prothrombin time; TB: total bilirubin; Ure: urea; WBC: white blood cell.
LASSO regression and multivariate logistic regression analysis
In the modeling population, a total of 12 predictors with non-zero coefficients were identified using LASSO regression analysis. These included fecalith, fluid, antimicrobial, WBC, NeuRatio, NLR, FIB, diameter, age, temperature, and diabetes. These variables were subsequently evaluated using multivariate logistic regression analysis. The results showed that fecalith, WBC, FIB, diameter, age, temperature, and diabetes were independent risk factors for perforation in patients with acute appendicitis within 24 h (Table 3 and Figure S1).
Multivariate logistic regression analysis of early perforation in acute appendicitis.

FIB: fibrinogen; OR: odds ratio; SE: standard error; WBC: white blood cell.
Establishment of nomogram prediction model
For the identified independent risk factors, optimal cut-off values for continuous variables were determined using ROC curve analysis and subsequently converted into categorical variables (Table 4). Based on these variables, an individualized nomogram prediction model was developed to estimate the risk of early perforation in patients with acute appendicitis (Figure 2). According to the cumulative scores of each factor in the nomogram, a higher total score corresponds to a greater risk of early perforation.
The optimal cut-off value of independent risk factors for predicting perforation in early acute appendicitis was determined.

FIB: fibrinogen; SE: standard error; WBC: white blood cell.
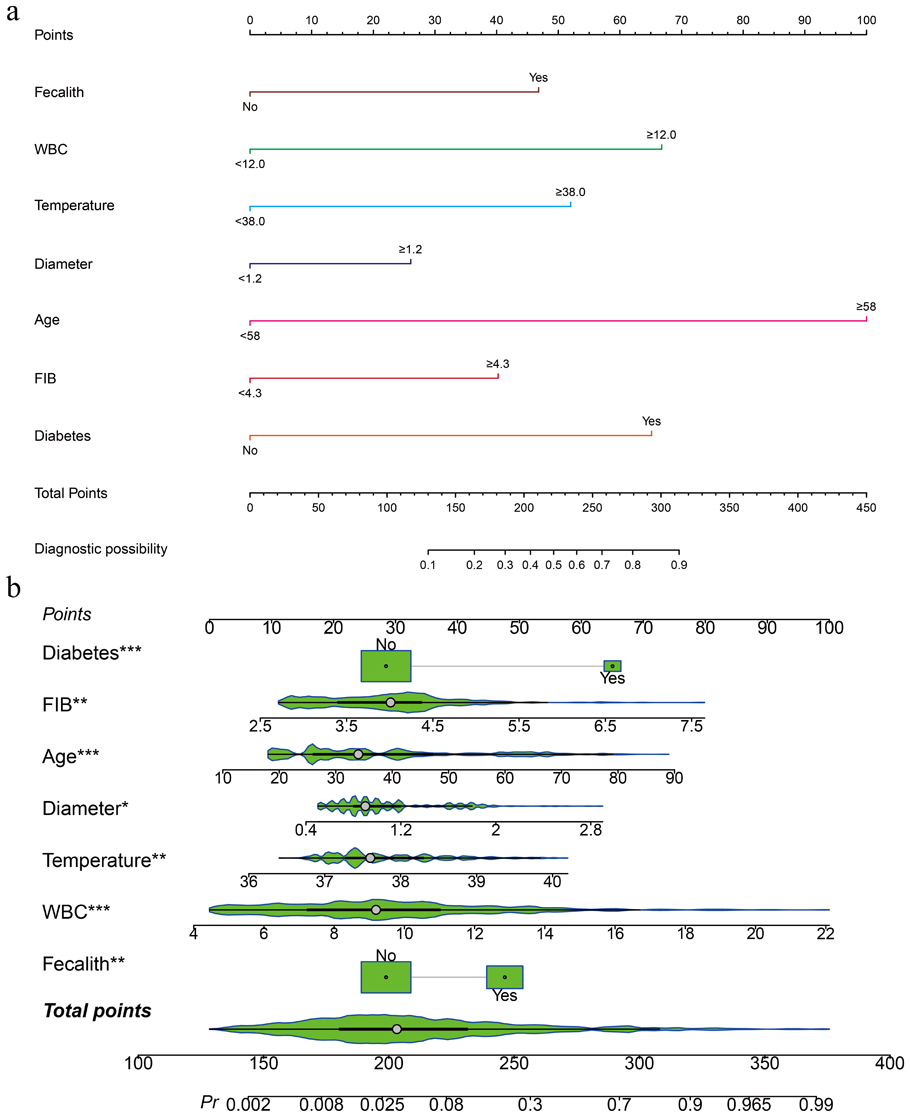
(a) The nomogram of each independent risk factor predicts the probability of early perforation in acute appendicitis. (b) The dynamic nomogram can obtain the prediction results in real time by inputting different variable values.
A nomogram to predict the probability of perforation in the early 24 h of acute appendicitis. Assign a value to each factor, obtain the corresponding value on the horizontal axis, and sum up the values for all factors. Mark the total points on the total axis. The values on the bottom line evaluate the probability of perforation.
Internal and external validation of the nomogram prediction model
Discrimination
ROC curves were plotted for both the modeling and validation cohorts. The AUCs were 0.891 (95% CI: 0.8494–0.9317) and 0.873 (95% CI: 0.8050–0.9401), respectively. Both AUC values exceeded 0.8, indicating that the prediction model demonstrated good discriminative ability (Figure 3).

ROC of the prediction model in the modeling and validation groups. (a) Modeling group and (b) validation group.
Calibration
Curve results showed that the mean absolute error of the training set and the validation set were 0.045 and 0.034, respectively, and the mean square error of the training set and the validation set were 0.00425 and 0.00269, respectively. The p values of Hosmer–Lemeshow goodness-of-fit test were 0.2855 and 0.4416, respectively, which were both >0.05, indicating that there was no significant difference between the predicted probability of the model and the true incidence, indicating that the prediction model had good prediction accuracy. The calibration chart showed that the predicted results of the model were highly consistent with the actual clinical observations (Figure 4).

Calibration curve of the prediction model in the modeling and validation groups. The x-axis represents the predicted perforation, while the y-axis represents the actual probability. The diagonal line represents a perfect prediction. The solid line indicates the performance of the nomogram. The closer the solid line fit to the diagonal line represents, the better the prediction model. (a) Modeling group and (b) validation group.
Clinical practicability
Based on the decision curves of both the modeling and validation cohorts, the use of the nomogram to predict the risk of perforation in patients with acute appendicitis within 24 h yielded a high net benefit, indicating that the model possesses good clinical applicability (Figure 5).

Decision curve of the prediction model in the modeling and validation groups. The thin solid gray line represents the assumption that all patients with acute appendicitis are perforated within 24 h. The solid black line represents the assumption that all patients with acute appendicitis do not develop perforation within 24 h. (a) Modeling group and (b) validation group.
Discussion
For cases of uncomplicated acute appendicitis, surgical intervention remains the recommended and widely accepted standard approach. 8 Nevertheless, recent evidence suggests that nonoperative management can achieve comparable rates of treatment success and major complications to surgery, although it is associated with longer hospital stays and higher recurrence rates. 9 In this context, antibiotic therapy may be considered in patients who are willing to accept the risk of recurrence. 10 On the one hand, antibiotic therapy preserves the potential physiological function of the appendix; on the other hand, it avoids unnecessary removal of normal appendiceal tissue and reduces the risk of surgical complications. 6 In addition, Fitz 11 and McBurney 12 believe that some cases of appendicitis can be cured without intervention, However Drake et al. 4 emphasized that the primary urgency in the management of acute appendicitis is to perform early surgical intervention in order to prevent progression to perforation, particularly this distinct form of acute appendicitis in which perforation occurs within the first 24 h of symptom onset. Accurate and quick identification and prompt surgical treatment are the key points. In many regions, ultrasound is widely used for the diagnosis of acute appendicitis due to its rapid and non-invasive nature. However, as demonstrated in the study by Bom et al., ultrasound has limited value in distinguishing between acute appendicitis with and without serious complications, and it cannot reliably rule out cases that require emergency surgical intervention. 13 Meanwhile, abdominal CT and MRI can be used as the optimal imaging diagnostic methods for the diagnosis of acute appendicitis, 10 their ability to accurately predict appendiceal perforation can vary depending on specific imaging features. In particular, the presence of an appendicolith and an increased appendiceal diameter on CT have been associated with a higher risk of early perforation, suggesting that these findings may serve as important predictors when integrated with clinical parameters. Therefore, we developed a clinical prediction model aimed at identifying the early occurrence of perforation in acute appendicitis. Previous studies have also attempted to construct predictive models, including the work by Liang et al., 14 which focused on gangrenous or perforated appendicitis in adults. In contrast, our model is specifically designed to detect perforation at an earlier stage, which may offer advantages for timely diagnosis and clinical decision-making. Our results indicate that the presence of a fecalith, elevated WBC count, increased FIB levels, higher temperature and age, enlarged appendiceal diameter on CT, and the presence of diabetes mellitus are key factors associated with early perforation in patients with acute appendicitis. A predictive model was constructed based on these seven factors, demonstrating strong discriminatory ability, good calibration, and favorable clinical utility. These findings highlight the potential value of the model in identifying early-stage perforation in acute appendicitis, thereby assisting clinicians in making timely interventions to reduce or prevent perforation.
As the first coagulation factor to be identified, FIB typically has a plasma concentration of 2–4 g/L and a half-life of ~4 days under normal physiological conditions. 15 The concentration of FIB increases significantly under pathological conditions such as infection, post-injury inflammation, or diseases associated with vascular rupture. Therefore, FIB is commonly regarded as an acute-phase protein, and its elevated levels in the blood are considered markers of systemic inflammatory response. In this study, a FIB cut-off value of 4.3 g/L was identified for predicting appendiceal perforation. The results demonstrated a significant difference in FIB levels between the perforation and non-perforation groups. Related in vitro studies have shown that FIB can significantly influence the function of WBCs, promoting cell migration, phagocytosis, the production of chemokines and cytokines, and other inflammation-related processes, 16 these findings underscore the important role of FIB in the inflammatory response. Shafagh et al. 17 and Wu et al. 18 have suggested that elevated FIB levels are associated with a higher incidence of appendicitis-related complications, such as perforation. However, the diagnostic value of FIB may overlap with that of other inflammatory markers, limiting its utility in the early stage of appendicitis. 19 Therefore, we believe that FIB should not be regarded as a diagnostic marker for acute appendicitis. Rather, it serves as an auxiliary indicator for distinguishing the presence or absence of appendiceal perforation. FIB has predictive value for perforation only when acute appendicitis has been confirmed.
Owing to its low time and cost requirements, WBC is the most commonly used clinical inflammatory marker. 20 As a routine laboratory test, it is widely utilized in the diagnosis of various inflammatory conditions. As an inflammatory marker, the WBC serves as a sensitive indicator for diagnosing infection-related diseases in clinical practice, and fluctuations in its levels can reflect the severity of the inflammatory response. 21 A previous study on gangrenous perforation of appendicitis in children demonstrated a significant correlation between WBC levels and clinical outcomes, 22 this finding suggests that WBC has certain advantages in risk assessment and prognostic prediction. However, because WBC elevation may result from systemic inflammatory responses triggered by acute appendicitis or other inflammatory conditions, 23 its predictive value as a standalone indicator is relatively limited 20 and should be interpreted in conjunction with other clinical factors.
Fever is a common accompanying symptom of acute appendicitis and has been reported in some studies as an indicator of disease severity.24–26 In this study, fever was identified as a statistically significant risk factor for predicting early perforation in acute appendicitis. The fever associated with appendicitis is primarily attributed to mixed infections involving anaerobic bacteria and Escherichia coli. As the infection progresses over time, body temperature tends to rise, thereby increasing the risk of sepsis and septic shock. Certain unique microbial characteristics 27 or host immune response28–30 may contribute to the development of appendiceal perforation by the time clinical symptoms become apparent. Body temperature serves as a valuable predictive marker and contributes to a more comprehensive clinical assessment.
Based on several classical articles published in the late 19th and early 20th centuries, surgeons have long believed that the development of appendicitis is closely associated with obstruction of the appendiceal lumen,4,11,12 among these factors, the presence of an appendicolith is considered the primary cause of appendiceal lumen obstruction. Following obstruction of the appendiceal lumen, the mucosa continues to secrete mucus, leading to increased intraluminal pressure. This progressive pressure elevation may result in ischemia, necrosis, and eventual perforation, forming a periappendiceal abscess and localized peritonitis, thus causing systemic peritonitis or appendiceal mass or abscess. 31 In this study, both appendiceal diameter and the presence of appendicolith differed significantly between the ePA group and the eNPA group. This is consistent with the findings of Tanrikulu. 32 These findings suggest that the presence of a fecalith and an increased appendiceal diameter significantly contribute to the risk of early appendiceal perforation.
Analysis of age and comorbidities revealed that the risk of early appendiceal perforation was significantly higher in patients over 58 years of age and in those with diabetes. According to relevant studies, the incidence of perforation in acute appendicitis ranges from 20% to 30%, but increases to 32%–72% in elderly patients.33–42 Some researchers suggest that age-related physiological changes in elderly patients—such as reduced lymphoid tissue and diminished blood supply—may accelerate the progression of acute appendicitis to perforation. 43 In elderly patients, diminished immune function and impaired ability to contain inflammation may facilitate the spread of infection and increase the risk of progression to perforation. Moreover, elderly patients often exhibit atypical symptoms of appendicitis, such as mild or absent abdominal pain, which can delay early diagnosis and treatment, thereby extending the disease course to some extent. In addition, the presence of complex comorbidities or delays in diagnosis among elderly patients may prolong preoperative preparation and surgical time, thereby further increasing the risk of early perforation in acute appendicitis. The risk of early perforation in acute appendicitis is also elevated in patients with diabetes mellitus. Previous studies have demonstrated that both cellular and humoral immune responses are significantly impaired in individuals with diabetes.44,45 As a result, the body’s ability to respond to infection is diminished, increasing the likelihood of inflammation spreading. Additionally, a hyperglycemic environment impairs tissue repair capacity and inhibits the healing process. Because a hyperglycemic environment reduces collagen deposition and impairs wound elasticity during the process of inflammatory wound healing, moreover, a hyperglycemic environment inhibits leukocyte phagocytosis, making injury to the appendiceal wall more likely to worsen, thereby increasing the risk of perforation. 46 Furthermore, Huerta et al. 47 demonstrated a strong association between diabetes mellitus and acute mesenteric ischemia, while Longstreth and Yao 48 found that acute colonic ischemia was independently associated with diabetes mellitus. Since early perforation in acute appendicitis may result from compromised blood flow to the appendiceal wall, pre-existing vascular conditions could increase the risk of early perforation. 49 In conclusion, prompt intervention and surgical management are particularly important for elderly patients and those with diabetes who present with acute appendicitis, in order to reduce the risk of perforation and associated complications.
Although pediatric patients and pregnant women were excluded from the present study, the nomogram developed may be of particular value in these populations, given the need to minimize radiation exposure from computed tomography (CT) imaging. Future studies focusing on these groups may help extend the applicability of the model.
Collectively, these findings support the utility of the nomogram model in providing a visual and quantitative evaluation of early perforation risk in acute appendicitis, thereby aiding clinicians in timely risk stratification.
In addition, this study has several limitations. First, due to the retrospective nature of the research, clinical data were collected from existing medical records, which may introduce selection bias. Second, some potential factors associated with perforation—such as C-reactive protein—were not included because of incomplete data, underscoring the need for future prospective studies to further validate their relevance. Finally, both model development and validation were performed internally using data from a single institution. While this approach allowed for model optimization in a relatively controlled setting, it may limit the generalizability of the findings to other clinical environments. External validation is recognized as a more rigorous method for assessing model robustness, however, noise or bias in external datasets may obscure the true performance of the model as observed in internal validation.50,51 Moreover, no formal sample size calculation was performed prior to the study, as the sample size was determined by the number of eligible patients available in the retrospective dataset. This may limit the statistical power, particularly in detecting smaller effect sizes. In addition, some predictors included in the nomogram—such as advanced age, presence of appendicolith, elevated inflammatory markers, and fever—are also factors that may influence the choice of surgical versus conservative treatment. This dual role introduces a potential methodological circularity, which should be taken into account when interpreting the model’s clinical implications. Finally, this study was a single-center study with a single sample source; therefore, multi-center and prospective cohort studies are necessary for further exploration.
Conclusion
This study retrospectively analyzed patients with acute appendicitis who developed perforation within the first 24 h of symptom onset. Multivariate analysis identified advanced age, elevated WBC count, increased FIB levels, enlarged appendiceal diameter on CT, and comorbid diabetes as independent risk factors for early perforation. Based on these variables, a predictive nomogram was established to estimate the individual risk of early perforation. This model offers potential utility in supporting timely clinical decision-making and optimizing management strategies for patients with acute appendicitis.
Supplemental Material
sj-docx-1-smo-10.1177_20503121251391271 – Supplemental material for Development and validation of a nomogram for predicting perforation in the early 24 h of acute appendicitis
Supplemental material, sj-docx-1-smo-10.1177_20503121251391271 for Development and validation of a nomogram for predicting perforation in the early 24 h of acute appendicitis by Yong Mei, Zhuo Huang, Zhi-Yuan Huang, Yan-Bing Shen, Zhang-Hao Liu, Qiao-Nuo Wei, Zhen Lan, Qin-Quan Zhang, Wen-Fei He, Wuerkaixi Abulaiti, Nuo Xu, Lian-Chun Mao and Wei-Dong Jin in SAGE Open Medicine
Footnotes
Ethical considerations
This study was reviewed and approved by the Research Ethics Committee of the People’s Liberation Army General Hospital of the Central Theater Command (approval no. (2025)128-01).
Consent to participate
Given the retrospective nature of the study, the committee granted a waiver of written informed consent.
Author contributions
Yong Mei: conceptualization, data curation, formal analysis, investigation, methodology, software, validation, visualization, writing—original draft, writing—review and editing. Zhuo Huang: investigation, software. Zhi-Yuan Huang: investigation, validation. Yan-Bing Shen: investigation, validation. Zhang-Hao Liu: data curation, formal analysis. Qiao-Nuo Wei: investigation, validation. Zhen Lan: data curation, investigation. Qin-Quan Zhang: data curation, software. Wen-Fei He: investigation, validation. Wuerkaixi Abulaiti: investigation, validation. Nuo Xu: investigation, validation. Lian-Chun Mao: data curation, validation. Wei-Dong Jin: conceptualization, funding acquisition, writing—review and editing.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Natural Science Foundation of Hubei Province of China (General Program, grant no. 2021CFB500).
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
The data and materials of this article could be available by contacting the corresponding author.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.