
Abstract
In developing countries such as Ghana, ophthalmia neonatorum (ON) remains a public health concern. This is because of its unknown etiology patterns, the growing concerns of antibiotic resistance strains and the contribution of ON to childhood blindness. This study was therefore conducted to determine the causative agents, risk factors and the antibiotic sensitivity patterns of micro-organisms associated with ON. A clinic-based prospective study was conducted in the Maternal and Child Health units of six health care facilities in the Central region of Ghana over a period of 17 months. Conjunctival swabs were taken from all neonates with clinical signs of ON. Isolation and characterization of bacteria were done using standard microbiological methods. Additionally, data were collected and analyzed on neonate’s demographics and clinical features of ON. Microbial growth was recorded in 86 cases (52.4%) out of the 110 neonates assessed. Staphylococcus spp. (39.2% of all positive cultures) was the most common causative organism. No case of gonococcus was isolated. Delivery method, vaginal discharge, administration of prophylaxis and weight of neonate were the risk factors associated with the development of ON (P < .05). The level of resistance to Tetracycline was found to be 73%. Neonatal conjunctivitis is more likely to be acquired postnatal. Culture and sensitivity testing are required as an important guide for treatment. The commonest causative organism, Staphylococcus spp., were found to be resistant to Teteracyline which is currently being used as prophylaxis in the prevention of ON. There is therefore the need to consider alternative measures in the prevention and control of ON.
Keywords
Introduction
Ophthalmia neonatorum is one of the major causes of blindness as reported by the World Health Organization (WHO) Vision 2020 “The Right to Sight, Global Initiative for the Elimination of Avoidable Blindness” and the commonest infection during the neonatal period.1,2 Neonatal conjunctivitis can occur immediately after a baby is born at the hospital or some days later after leaving the hospital. The occurrence of the infection ranges between less than 2% to 23% in developing countries and is dependent mainly upon socioeconomic conditions, level of knowledge on general health, standard of maternal healthcare as well as the choice of prophylactic eye treatment.3,4
The infection can be septic or aseptic and pathogens predominantly isolated include Neisseria gonorrhea, Chlamydia trachomatis, Staphylococcus aureus, Streptococcus spp., Escherichia coli, Klebsiella pneumoniae, Serratia marcescens, Proteus, Enterobacter and Pseudomonas spp. 5 Due to the lack of diagnostic techniques with appropriate sensitivity and specificity, Chlamydial ON has been underdiagnosed, although in recent times, it has been found to be more prevalent than gonococcal ON. 6
In the late nineteenth century, Crede’ introduced an intervention of cleaning the eyes of newborns with a 1% silver nitrate to prevent ophthalmia neonatorum due to only gonococcal infections because it was the commonest cause of ON. 7 Recently, Chlamydia trachomatis has been reported to be more prevalent in both the developed countries and the developing world.8,9 However, the most frequent isolated microorganism in developing countries is Staphylococcus aureus.10,11,12
Clinical signs such as redness, tearing, purulent eye discharge, erythema and edema of the eyelids, a pseudo-membrane and corneal perforation are regularly presented by neonates with the infection. 5 Predisposing risk factors include premature rupture of membranes (PROM), the place of delivery, maternal infections of the lower genital tract, prolonged labour, low Apgar score, neonatal sepsis, low birth weight, premature labour, amniotic fluid stained with meconium, low socioeconomic status, unhygienic environment, absence of eye prophylaxis, unsterile handling of neonates by relatives and nutritional deficiency during pregnancy.1,8,13,14 Among the various causes of ophthalmia neonatorum, PROM has been found to be the most important.1,8,15 Treatment for neonatal conjunctivitis is based on clinical presentations and laboratory results. WHO guidelines for the management of sexually transmitted infections, recommends that all cases of ophthalmia neonatorum be treated for both N. gonorrhoea and C. trachomatis. 16 According to the Standard Treatment Guideline (2010) from the Ghana Health Service, 17 the cleaning of the neonate’s eyes immediately after birth and the application of 1% tetracycline ointment into the eyes is recommended as prophylaxis.
Silver nitrate prophylaxis (Crede’s 1% Silver nitrate prophylaxis) is no more popular due to its ineffectiveness in preventing chlamydial infection and the tendency to cause chemical conjunctivitis. 18 Tetracycline or erythromycin ointment has replaced Silver nitrate prophylaxis and this is because of the high efficacy they have against Chlamydia and gonorrheal pathogens. However, diagnosis based on only clinical signs and symptoms is not adequate for treatment of ON as has been the practice. 19
There have been declines in the incidence of ophthalmia neonatorum with the introduction of universal prophylaxis in recent years as well as the provision of clear guidelines for the treatment of Chlamydia trachomatis and Neisseria gonorrhea. However, it is not clear how to manage newborns with conjunctivitis secondary to other bacterial organisms. It is important to note that, routine prophylaxis carries the risk of antibiotic resistance, especially in patients with ON due to gonococcal infection. 20
Although, blindness from ON is rare nowadays, the risk can only be prevented by providing a well-organized medical care for mothers and neonates. Unfortunately, this is still a problem in rural areas of developing countries. Unknown etiology patterns of ON in Ghana, the growing concerns of antibiotic resistance strains and the contribution of ON to childhood blindness are of major public health concern. According to Schaller & Volker Klauss, there is the need for further research and monitoring of the prevalence of the various causative agents of ON in different parts of the world, so that prevention and treatment protocols can be adjusted. 20 Thus, the purposes of this study was to determine the causative agents, risk factors and the drug sensitivity patterns of micro-organisms associated with ophthalmia neonatorum in the Central region, Ghana.
Materials and Methods
The study was conducted at the neonatal wards of 6 hospitals in the Central region over a period of 17 months (January 2018-May 2019). Neonates born at the facilities without any major congenital malformations, presenting with clinical findings of conjunctivitis within a period of 28 days were enrolled in the study after informed consent has been sought from the mothers. A structured questionnaire was filled for each neonate by the midwives who also read out the questions (interview guide) and filled in the mother’s responses. Information not readily available from the mothers were obtained from the neonate’s records at the hospital and microbiological tests were then performed. Data obtained from the interview included details such as gestational age, weight, gender, mode of delivery, onset of neonatal conjunctivitis, signs and symptoms accompanying the infection (erythema, swelling of the eyelids, eye discharge, unilateral/bilateral involvement), maternal and neonatal risk factors and whether neonates had received prophylaxis or management for their infections.
Culture and Sensitivity
Neonates with clinical signs of conjunctivitis had swabs taken from their inferior conjunctival fornix with sterile swabs for culturing. Swabs were labelled and immediately transported to the laboratory (within 2 hours). Each swab was inoculated on blood, MacConkey, plate count, Thayer-Martin, and chocolate agars to ascertain microbial growth. Only sterile media were used in culturing. The Chocolate agar plates were incubated under anaerobic conditions using CO2 jar for Neisseria gonorrhoea whereas the other plates were incubated at 37 °C for a minimum of 24 hours. 14 The isolate bacteria were identified using standard microbiological procedures which included colonial morphology, gram staining and biochemical tests. The susceptibility patterns of bacterial isolates to antibiotics were determined using the disc-diffusion tests (Kirby-Bauer). Direct fluorescent anti-body test and Giemsa staining for Chlamydia trachomatis could not be done because of the unavailability of logistics.
Ethical Approval and Informed Consent
This study was approved by the Institutional Review Board of the University of Cape Coast (IRB No. UCCIRB/CHAS/2017/08). All mothers provided written informed consent prior to enrolment in the study.
Results
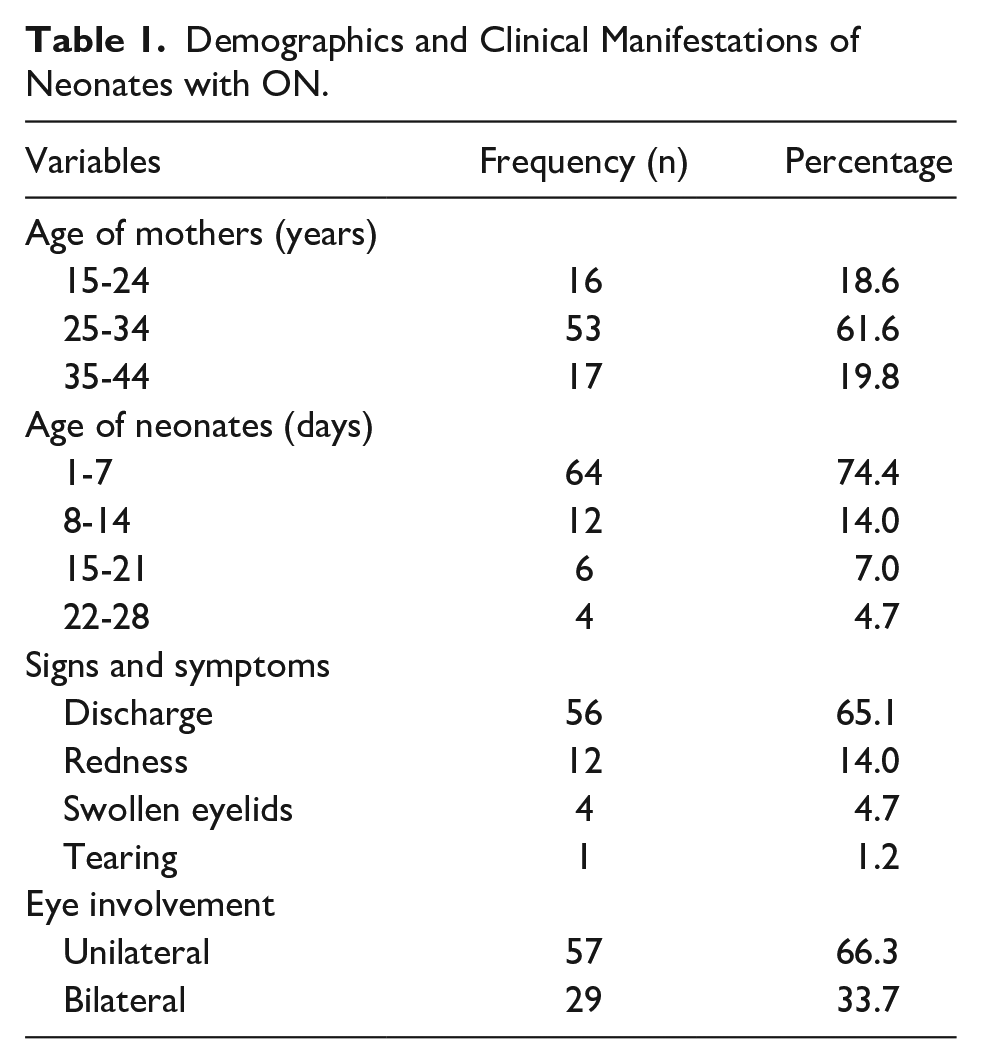
A microbiological study was performed on 110 neonates from the 6 facilities. Bacteria cultures were positive in 86 neonates (52.4%) and 24 (7.6%) were free from demonstrable pathogenic bacteria despite the presence of conjunctivitis. The 24 neonates were subsequently excluded from the study. Among positive cultures, 75 (87.2%) were found to be monobacterial cultures and 11 (12.8%) were two bacterial species. There was a significant male predominance among neonates with positive culture (60.5%). Babies delivered through caesarean section were 34.9%. Only 6 (7%) of these babies had low birth weight. Unilateral conjunctivitis was present in 57 (66.3%) of the neonates and the onset of conjunctivitis within the first week constituted 91.6%. The mean age at the time of conjunctivitis for the 86 cases was 5.6 days with the age range of 1-28 days. All cases were clinically diagnosed based on the signs of discharge, 56 (65.1%), redness, 12 (14.0%), swelling 4 (4.7%) and tearing 1(1.2%). There was a relation between the presence of discharge and the occurence of ophthalmia neonatorum (P < .001). Most of the mothers were between the ages of 25-34 years (61.6%) (Table 1).
Demographics and Clinical Manifestations of Neonates with ON.
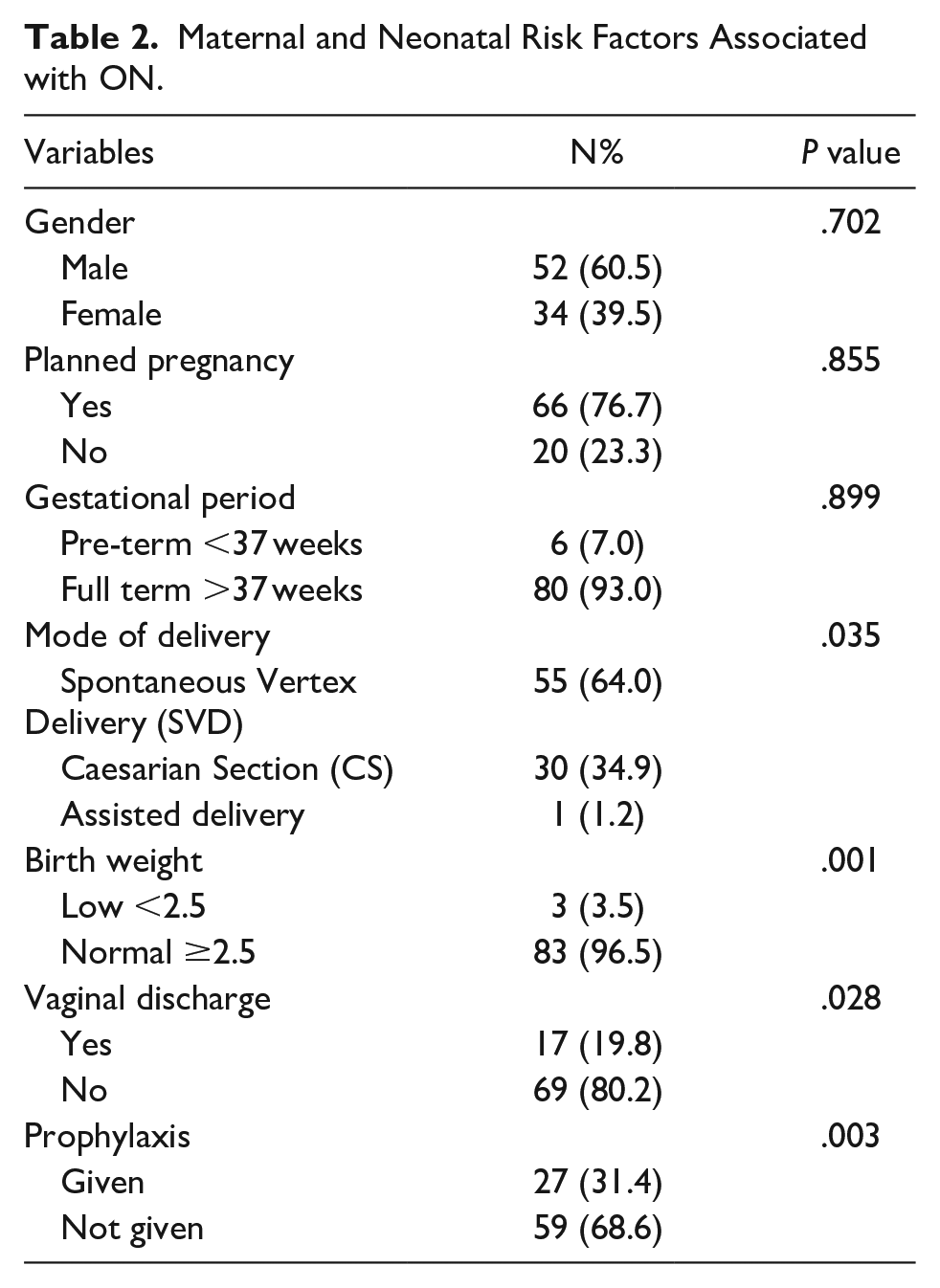
The risk factors for ON considered in this study were also analyzed but gender of neonates, planned pregnancy and gestational period were found not to be significant (Table 2).
Maternal and Neonatal Risk Factors Associated with ON.
Eleven (11) different strains of bacteria were identified. The most common isolate was Staphylococcus spp. which constituted 38 (39.2%) of all positive cultures followed by Bacillus spp. in 17 (17.5%) samples. Neisseria gonorrhea was not isolated from any case (Table 3).
Frequency of Microorganism Isolates.

Sensitivity as determined by the Kirby-Bauer method to antimicrobial agents commonly used in the treatment of conjunctivitis, which includes Ciprofloxacin, Gentamicin, Chloramphenicol, and Tetracycline indicated that Tetracycline 73 (75.3) had a high bacterial resistance (Table 4). Whereas Gentamycin 75 (77.3) and Ciprofloxacin 68 (70.1) were generally effective (Table 5).
Antimicrobial Susceptibility Testing Showing Bacteria that were Resistance to Commonly Used Antibiotics.
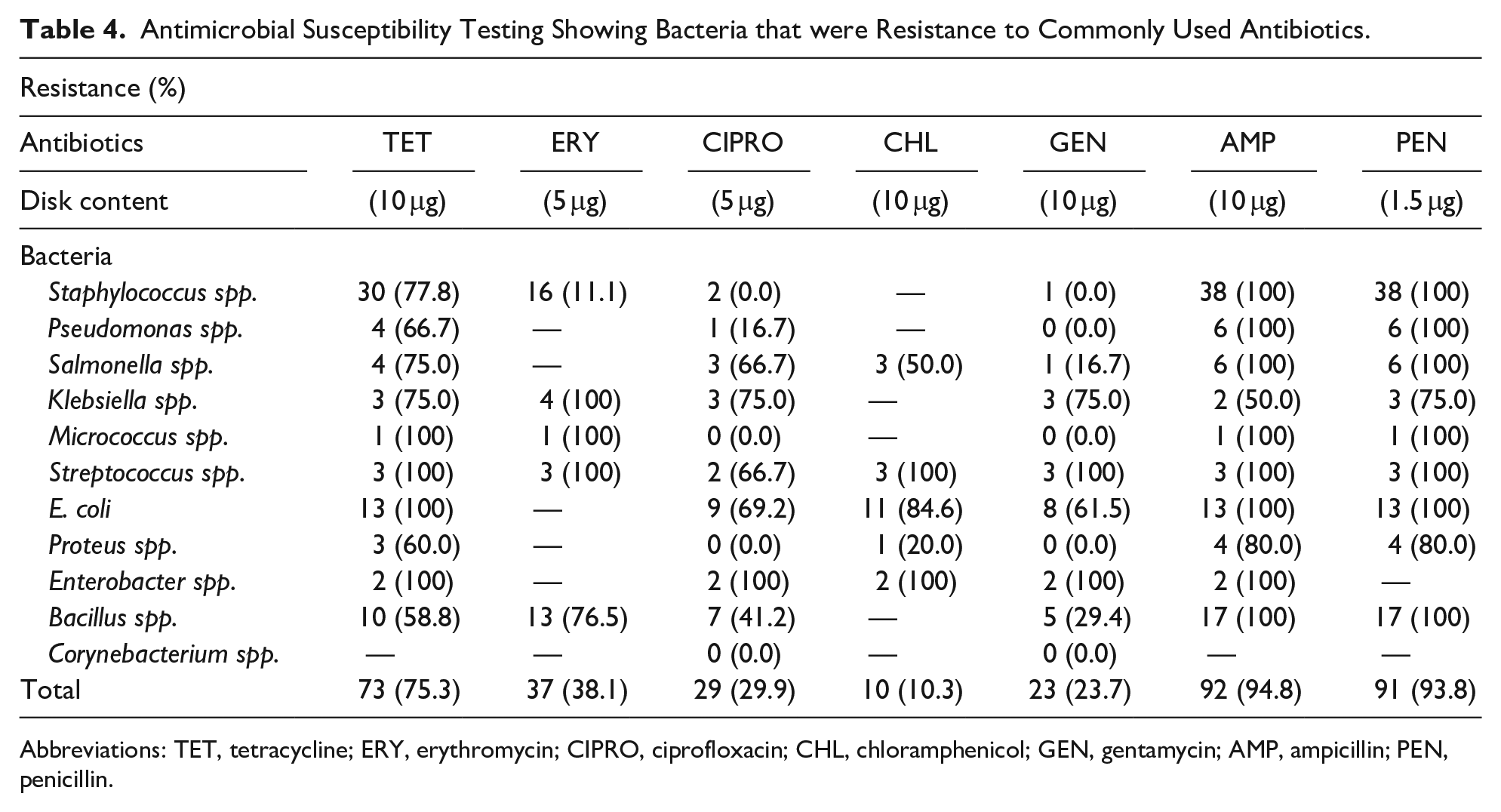
Abbreviations: TET, tetracycline; ERY, erythromycin; CIPRO, ciprofloxacin; CHL, chloramphenicol; GEN, gentamycin; AMP, ampicillin; PEN, penicillin.
Antimicrobial Susceptibility Testing Showing Bacteria that were Susceptible to Commonly Used Antibiotics.
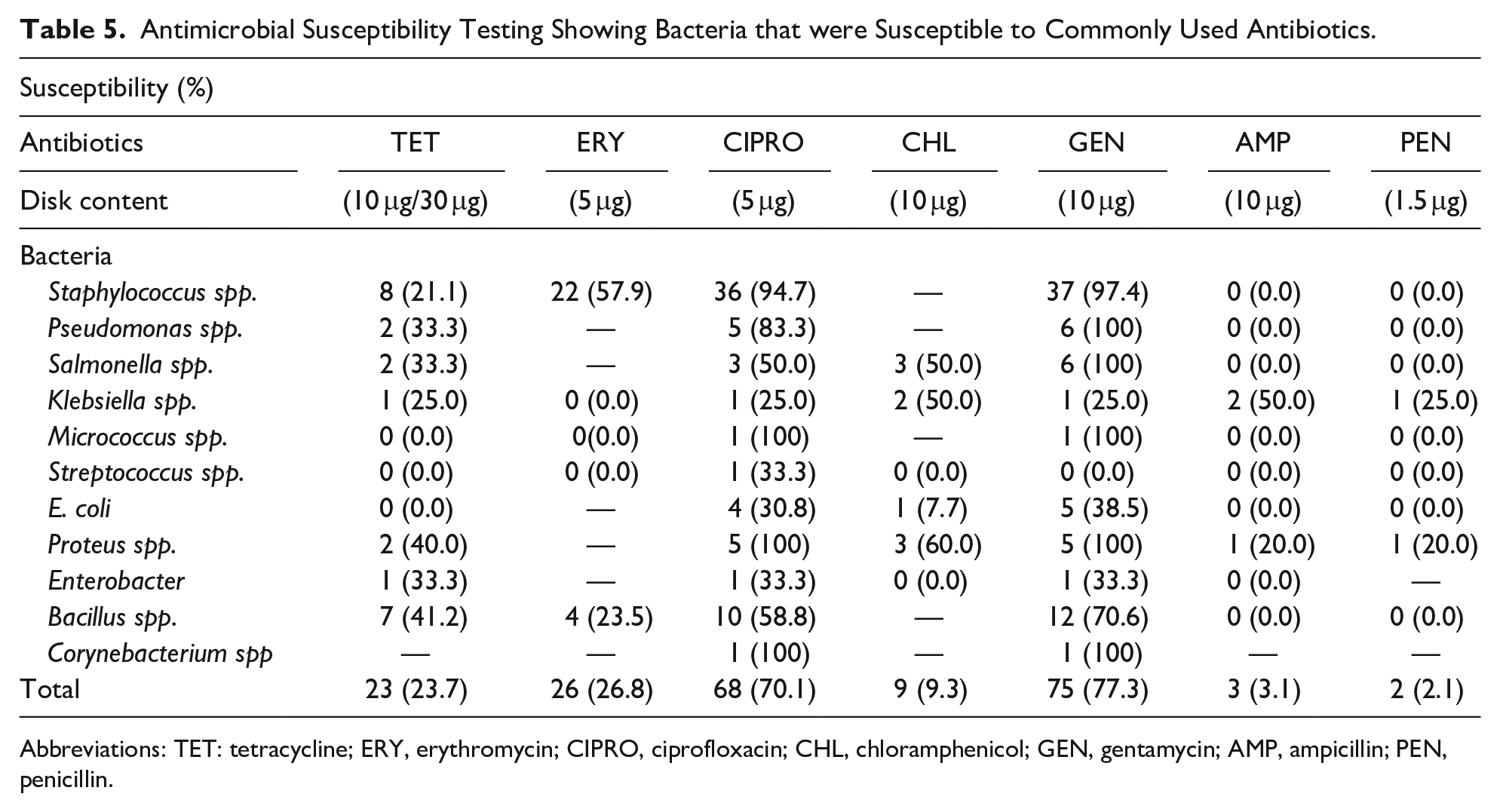
Abbreviations: TET: tetracycline; ERY, erythromycin; CIPRO, ciprofloxacin; CHL, chloramphenicol; GEN, gentamycin; AMP, ampicillin; PEN, penicillin.
Discussion
In this study, a total of 86 newborns (52.4%) with clinical conjunctivitis were enrolled. The male predominance (60.5% vs 39.5%) was consistent with studies from Iran (62% vs 38%), Norway (75% male neonates) and Saudi Arabia (63% males).14,21 Sex did not influence the development of ON, which is in agreement with other similar studies.11,14 There was a relationship between conjunctivitis and neonatal body weight (Table 2). However, close to 97% of neonates in this study had normal weight thus suggesting the risk for ON cannot be explained based on birth weight. The mean age (5.6 days) of the neonates indicates that ON is postnatally acquired. This period of onset suggests that other factors such as low maternal education on new born care practices, which results in poor mother and baby hygiene may inadvertently cause ON.
Unilateral conjunctivitis was more common [57 (66.3%)] in our study, similar to other reports by Yip et al 22 and Epling. 23 The earliest time at which conjunctivitis occurred was within the first week of birth, which was seen in more than half of the neonates (74.4%). This was in agreement with a study done by Verma et al 24 who reported that the onset of neonatal conjunctivitis is mostly within the first week of birth and only few babies develop eye discharge after 7 days.
A study from Ilorin found the pre-disposing factors to neonatal conjunctivitis to include antenatal maternal vaginal discharge, low social class and maternal age of less than 20 years. 25 As reported by Kolade, 25 vaginal discharge during pregnancy was associated with ON in this study. However, we did not find any correlation between age of mothers and the occurrence of ON. This could be due “to the” manupulative higher percentage of mothers who were outside the teen age in this study.
The current study did not record any mother having premature rupture of membranes, thus, no relationship could be established between it and ON. Similar studies which reported on mothers having premature rupture of membranes, indicated that there was no statistically significant relationship between development of neonatal conjunctivitis and rupture of membranes.8,14,15,26 Also, caesarean section was found to have a significant correlation with ON in the present study (Table 2). This could be due manipulative nature of the procedure and the possible contamination of the caesarean section.
The 7.6% of cases which could not be assigned to pathogenic bacteria could be attributed to other organisms like anaerobes, viruses, chemical conjunctivitis or nasolacrimal duct obstruction. 27
Staphylococcus spp. was resistant to tetracycline but sensitive to Ciprofloxacin and Gentamicin (Tables 4 and 5). Our finding is in agreement with a study by Ayebazibwe et al 28 who also found that Staphylococcus aureus were resistant to Tetracycline (91%), the routinely used drug for prophylaxis but sensitive to Ciprofloxacin (74%). Hence, Ciprofloxacin and Gentamicin could be useful in treating ON caused by resistant strains of bacterial.
The predominance of Staphylococcus spp. in this study may suggest that most of the cases of neonatal conjunctivitis are post-natally acquired probably due to poor hygiene rather than during passage through the birth canal as suggested by Krohn et al. 29 Moreover, the role of the bacteria as a causative agent of ON is uncertain as they can be found in both neonates with conjunctivitis and asymptomatic neonates.11,29 Micrococcus spp. isolated in this study are frequently found on the skin and conjunctiva of humans and have been reported as an opportunist in conjunctivitis. 30 Bacillus spp. are most likely part of the normal flora as well as the Corynebacterium spp. isolate.
E. coli as a causative agent can cause neonatal sepsis. 31 The best way of identifting E. coli and the various causative agents of ON is through laboratory analysis.31,32 Unfortunately, this practice is not common in our health facilities as diagnosis of ON is solely based on clinical impression. Incorporating laboratory analysis in the diagnosis regime of ON will not be a challenge because most mothers were receptive to the idea of laboratory diagnosis. Besides, the laboratory facilities are available in most health facilities where these mothers access health care.
There was a significant association between eye discharge and the occurence of ON (P < .001) in the current study. Most studies have reported the need for all neonates who present with eye discharge to undergo a thorough physical examination and full microbiological investigation that includes culture and microscopy for bacteria and C trachomatis.10,14 This is because most pathogens have drug resistance to antibiotics such as Ampicillin and Penicillin. 33 The challenge of increasing risk of drug resistant strains of Neisseria gonorrhea worldwide have also been highlighted in the literature. 34
Several microorganisms isolated from neonates with ON, show different antibiotic susceptibility patterns according to the geographical regions and whether the infection was community or hospital acquired. 35 In our study, some of the samples were acquired from neonates whose mothers were yet to be discharged from the hospitals and others from babies reporting back to the hospital with ON, hence, the difference in antibiotic susceptibility. In addition, there was a statistical significant difference between the presence of conjunctivitis and provision of prophylaxis (P < .003). The antibiotic that showed a high level of resistance apart from Ampicillin and Penicillin was Tetracycline (Table 4) which was consistent with studies elsewhere.3,4
In their study, Zuppa et al 36 reported that none of the used drug combinations proved effective enough to warrant their use on a large scale. In the current study, Tetracycline which is routinely used as prophylaxis was inffective against most of the causative agents on ON. There is therefore the need to consider the use of alternative antibiotics as prophylaxis in the prevention and control of ON.
Conclusion
Neonatal conjunctivitis mostly occurs during the first week after birth. That notwithstanding, culture and sensitivity testing are required as an important guide for treatment of the infection. Our study suggests the need to begin discussions in the consideration of alternative measures in the prevention and control of ON in developing countries.
Supplemental Material
sj-pdf-1-gph-10.1177_2333794X211019700 – Supplemental material for A study of Ophthalmia Neonatorum in the Central Reion of Ghana: Causative Agents and Antibiotic Susceptibility Patterns
Supplemental material, sj-pdf-1-gph-10.1177_2333794X211019700 for A study of Ophthalmia Neonatorum in the Central Reion of Ghana: Causative Agents and Antibiotic Susceptibility Patterns by Samuel Bert Boadi-Kusi, Samuel Kyei, Selina Holdbrook, Emmanuel Kwasi Abu, Jonathan Ntow and Abena Mantebea Ateko in Global Pediatric Health
Footnotes
Acknowledgements
The authors are grateful to the Directors of the various health facilities in the Central Region for granting permission to conduct the study and to the health workers for their assistance. We are also grateful to all the postnatal mothers who participated in this study.
Author Contributions
SBBK: Conceived the study; contributed to the acquisition, analysis and interpretation of data, drafted and critically revised the manuscript and gave final approval.
SK & SH: Contributed to the study design, analysis and interpretation of data; contributed to the writing of the manuscript; critically revised the manuscript and gave final approval.
EKA: Contributed to the analysis and interpretation of data; critically revised the manuscript and gave final approval.
JN: Contributed to the acquisition, analysis and interpretation of data, drafted; critically revised the manuscript and gave final approval.
AMA: Contributed to the acquisition, analysis and interpretation of data; gave final approval of the manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available upon request.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.