
Abstract
Despite dramatic declines in the incidence of ophthalmia neonatorum with universal prophylaxis, it remains a clinically important cause of eye disease in newborns. While clear guidelines exist for the treatment of the historically primary agents of ophthalmia neonatorum (Chlamydia trachomatis and Neisseria gonorrhoeae), it is less clear how to manage newborns with conjunctivitis secondary to other bacterial organisms, particularly those also frequently implicated in neonatal sepsis. We present the case of a 3-day-old well-appearing term infant with unilateral purulent conjunctivitis. The eye culture grew Escherichia coli, an unusual cause of ophthalmia neonatorum. After a limited sepsis evaluation proved negative, the infant was switched to moxifloxacin ophthalmic drops and made a full recovery. This case highlights the challenge of managing a rare presentation with minimal guideline support, as well as the need to consider other bacterial causes of neonatal conjunctivitis which are emerging in the era of routine prophylaxis in the United States.
Keywords
Introduction
The incidence of infectious ophthalmia neonatorum (also called neonatal conjunctivitis) in the United States has declined dramatically with the advent of universal prophylaxis, yet still occurs after 1%–2% of births.1,2 The majority of cases in term infants are caused by organisms acquired during the passage through the birth canal, with Chlamydia trachomatis and Neisseria gonorrhoeae being the leading etiologic agents traditionally reported. However, with the advent of routine ophthalmic prophylaxis in the immediate newborn period in the United States, other bacterial causes of ophthalmia neonatorum have started to become more prevalent without clear management guidelines available. 3
Case presentation
A female infant born at 39 weeks gestation via normal spontaneous vaginal delivery presented at 3 days of age to the emergency room with a right-sided purulent eye discharge progressing over the past day. The infant had received erythromycin ointment prophylaxis on the first day of life and had an uneventful nursery course and was discharged home at 48 h of age.
The mother was Group B streptococcus positive via polymerase chain reaction (PCR) screening late in the third trimester and was appropriately treated with clindamycin prior to delivery as she was allergic to penicillins. 4 The remainder of the mother’s serologies was unremarkable, although she was not tested for N. gonorrhoeae or C. trachomatis.
In the emergency room, the infant was noted to have a copious purulent discharge from the right eye, with significant conjunctival injection and prominent palpebral soft-tissue swelling. She was clinically well otherwise, afebrile, with normal vital signs and did not meet the pediatric Systemic Inflammatory Response Syndrome criteria for potential sepsis. 5 The decision was made to perform only a limited evaluation including complete blood count, basic metabolic profile, peripheral blood culture, and an eye culture along with N. gonorrhoeae and C. trachomatis PCR from the right eye drainage. The white blood cell count was 13.5 × 109 L−1, hematocrit was 46.5%, and platelet count was 297 × 109 L−1. The electrolytes were normal. The Gram stain of the discharge revealed Gram-negative rods. She was started empirically on ceftriaxone 50 mg/kg/day for gonococcal coverage as well as oral erythromycin 50 mg/kg/day for chlamydial coverage per guidelines, 3 with a diagnosis of ophthalmia neonatorum pending the final results of the cultures and admitted to the inpatient unit given her age and the higher risk of disseminated infection.
The N. gonorrhoeae and C. trachomatis PCRs came back negative within 24 h of admission and the erythromycin was therefore discontinued. While a single dose of a third-generation cephalosporin is an appropriate treatment for presumed gonococcal conjunctivitis, 3 the baby was continued on cefotaxime pending the eye and blood culture results given the Gram-negative rods in the ocular discharge Gram stain. The final eye culture came back at 72 h with moderate growth of Escherichia coli which was pan-sensitive except for ampicillin. Blood cultures remained negative. There was a significant clinical improvement in the conjunctivitis within 48 h of therapy initiation without involvement of the contralateral eye. The baby continued to breastfeed well and remained vigorous and afebrile with stable vital signs.
In consultation with the infectious diseases and ophthalmology specialists, we decided to start moxifloxacin ophthalmic drops 0.5%, 1 drop to each eye three times daily on day 4 of hospitalization which the baby tolerated well for 24 h. 6 The cefotaxime was discontinued and the infant was discharged home on day 5 to complete a 7-day course of the topical moxifloxacin. On follow-up 5 days after discharge, there was complete resolution of the conjunctivitis and no subsequent complications.
Discussion
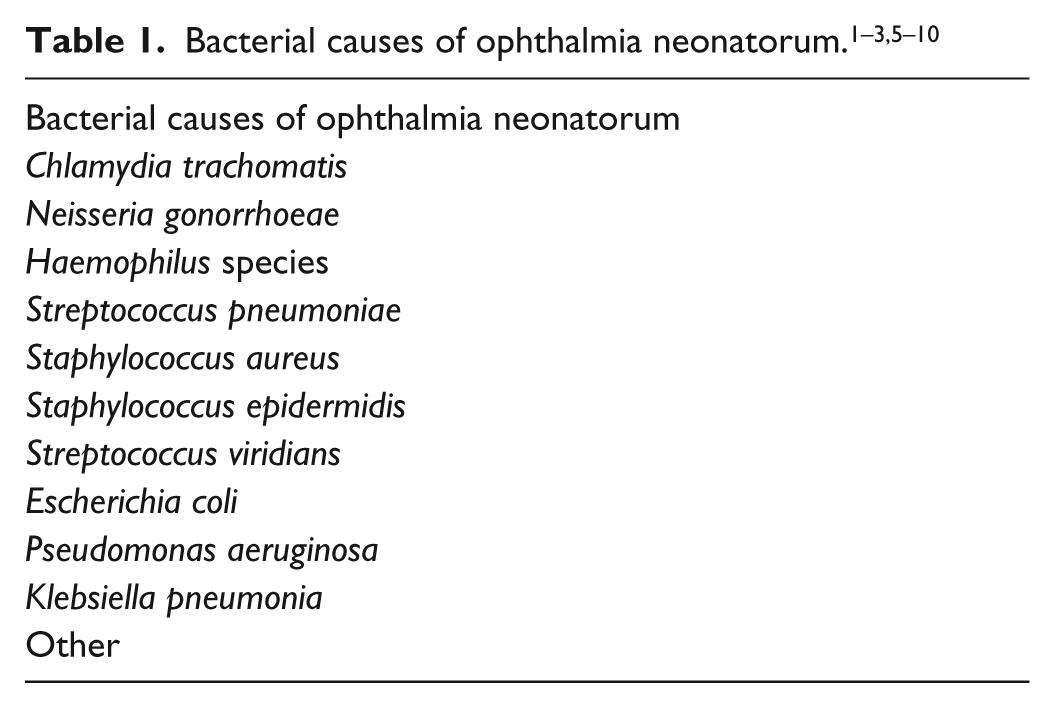
Ophthalmia neonatorum remains a problem among neonates in the United States, with an overall incidence of 1%–2%.1,2 With the implementation of routine erythromycin prophylaxis in the United States, the proportion of cases of neonatal conjunctivitis caused by N. gonorrhoeae is now less than 1%, while for C. trachomatis it is as low as 2%. Other bacterial pathogens constitute 30%–50% of the cases 3 (Table 1). While E. coli has been reported as a causative bacteria of ophthalmia neonatorum in neonatal intensive care unit settings,7,8 it is rarely reported in term infants, with only a single case report found in the literature. 6
This infant’s presentation of unilateral purulent eye discharge and inflamed conjunctiva was consistent with ophthalmia neonatorum and merited empiric treatment for the predominant causes which include N. gonorrhoeae and C. trachomatis. In afebrile, otherwise well-appearing infants with a suspicion of isolated gonococcal conjunctivitis, there is no current recommendation for a full sepsis workup unless clinically warranted, and a limited evaluation including blood and eye cultures should be adequate. 3 However, the presence of Gram-negative rods on the Gram stain of the discharge gave us cause for concern given that non-gonococcal and non-chlamydial ophthalmia neonatorum has been linked to potentially severe orbital complications including orbital abscesses and corneal perforation,9,11 which we felt warranted a more aggressive initial empiric management. With E. coli being one of the major causative agents of neonatal sepsis, 10 we were concerned that E. coli conjunctivitis could potentially represent a source of sepsis in the affected newborn. On further review, we found that while sepsis has been reported in neonates who presented with ophthalmia neonatorum, the causative organism was either not identified or was different from the organism in the eye.12,13
In the lone published case report we could find on E. coli ophthalmia neonatorum, the infant was also clinically well otherwise and afebrile. 6 That neonate underwent a full sepsis workup including a spinal tap, which was unremarkable, and all cultures remained negative. The initial empiric antibiotic management was similar to our own case in order to provide adequate coverage for N. gonorrhoeae and C. trachomatis, and in both instances, the infant was discharged home on moxifloxacin alone once the eye cultures confirmed the presence of E. coli and there was a definite clinical improvement of the conjunctivitis.
Given the currently available data, it may be reasonable to consider only a limited evaluation of the well-appearing afebrile neonate with an isolated case of conjunctivitis even when the Gram stain reveals a bacteria while still providing initial systemic broad coverage with a third-generation cephalosporin and erythromycin as a precautionary measure against disseminated disease pending final culture results. Once a causative organism for the ophthalmia neonatorum has been identified, then it may be reasonable to consider switching over to a topical broad-spectrum ophthalmic antibiotic such as moxifloxacin to complete the treatment course.14,15 E. coli, while rarely listed among the causative agents in term infants, should be considered in the differential especially with the presence of Gram-negative rods on the Gram stain. Moreover, as different bacteria emerge in ophthalmia neonatorum due to the effective reductions in N. gonorrhoeae and C. trachomatis with routine eye prophylaxis at birth, further study is needed to determine whether topical therapy alone may prove to be adequate in the clinically well-appearing infant. Furthermore, it may be worth evaluating the replacement of the traditional routine erythromycin ophthalmic prophylaxis with a broader spectrum antibiotic given the significant rise in the non-gonococcal and non-chlamydial etiologies of ophthalmia neonatorum, along with the cost to benefit ratio of such an approach. Updating guidelines to address the possible value of empiric management of such cases has the potential of reducing unnecessary evaluations and length of stay along with the associated benefits of potential cost reductions in care.
Footnotes
Acknowledgements
The authors wish to thank Dr Hope Pogemiller for her co-management of the case.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
Our institution does not require ethical approval for reporting individual cases or case series.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed consent
Written informed consent was obtained from a legally authorized representative(s) for anonymized patient information to be published in this article.