
Abstract
Necrotizing enterocolitis (NEC) remains to be the most critical and frequent gastrointestinal disorder understood in neonatal intensive care units (NICU). The presented study was intended to assess the prevalence of NEC and associated factors among enteral Fed preterm and low birth weight neonates. Institution based retrospective cross-sectional study was conducted on 350 enteral Fed preterm and low birth weight neonates who were admitted at selected public hospitals of Addis Ababa from March 25/2020 to May 10/2020. The data were collected through neonates’ medical record chart review. A total of 350 participants were enrolled in to the study with the response rate of 99.43%. One hundred eighty-four (52.6%) of them were male. The majority 123 (35.1%) of them were (32 + 1 to 34) weeks gestational age. The prevalence of NEC was (25.4%) (n = 89, [95% CI; 21.1, 30.0]). Being ≤28 weeks gestational age (AOR = 3.94, 95% CI [2.67, 9.97]), being (28 + 1 to 32 weeks) gestational age (AOR = 3.65, 95% CI [2.21, 8.31]), birth weight of 1000 to 1499 g (AOR = 2.29, 95% CI [1.22, 4.33]), APGAR score ≤3 (AOR = 2.34, 95% CI [1.32, 4.16]), prolonged labor (AOR = 2.21, 95% CI [1.35, 6.38]), maternal chronic disease particularly hypertension (AOR = 3.2, 95% CI [1.70, 5.90]), chorioamnionitis (AOR = 4.8, 95% CI [3.9, 13]), failure to breath/resuscitated (AOR = 2.1, 95% CI [1.7, 4.4]), CPAP ventilation (AOR = 3.7, 95% CI [1.50, 12.70]), mixed milk (AOR = 3.58, 95% CI [2.16, 9.32]) were factors significantly associated with NEC. Finally, the prevalence of NEC in the study area was high. So that, initiating the programs that could minimize this problem is required to avoid the substantial morbidity and mortality associated with NEC.
Background
NEC is the most common emergency of the gastrointestinal tract happening in the neonatal period. 1 NEC is a global issue that has arisen in the past 25 years as the most common gastrointestinal emergency in neonatal NICU. 2 NEC is stated as the most common critical gastrointestinal disorder affecting very preterm or very low birth weight (VLBW) infants. 3 NEC is the most known life-threatening, acquired gastrointestinal disorder in the newborn infant. 4 NEC is a common and overwhelming gastrointestinal emergency that mainly affects premature infants.5-7
NEC is the most recognized lethal gastrointestinal emergency encountered in the NICU.8,9 The incidence of NEC is 6% to 10% in infants with birth weight less than 1500 g. 5 The evidence revealed that 7 in 100 of all VLBW infants in NICU are probable to develop NEC. 10 The proportion of NEC among neonates with congenital heart disease was 3.7%. 11 NEC is a leading cause of morbidity and mortality, particularly in extremely LBW infants. 12 The mortality due to NEC has not reduced considerably despite advances in neonatal care and better knowledge of clinical and basic sciences. 5
In spite of advances in neonatal care, NEC remains a leading cause of morbidity and mortality among premature infants in ICU. 8 NEC is a common cause of morbidity and mortality in VLBW infants. 13 The mortality rate of neonates with NEC leftovers high and is significantly associated with a birth weight category. 14 NEC is related to a substantially worst neurodevelopmental consequence than prematurity alone. The presence of advanced NEC and requirement for surgery rise the risk of neurological impairment. 15 Also, NEC is a costly disease which is responsible for about 20% of NICU costs annually. 9
The risk factors for NEC are multifactorial. 16 The risk of NEC is found to be inversely proportional to gestational age and weight at birth while fetal growth restriction and compromise may be further specific risk factors. 3 Enteral feeding is advanced slowly in preterm neonates considering the risk of NEC. Whereas, prolonged intravenous alimentation in these neonates, however, may rise the risk of morbidity and mortality associated with sepsis, principally in low resource settings. 17 Because of this feeding preterm infants with artificial formula is related to the faster rates of growth, but with a closely doubling of the risk of developing NEC. 18 Breast milk feeding has been related with lower risk of NEC. But, mothers of VLBW infants often get inadequate milk production, this leads to mixed feedings of breast milk and formula. 13
Formula feeding and prolonged duration of parenteral feeding were related to the augmented risk of NEC. 19 Meconium aspiration syndrome, sepsis, and postnatal asphyxia factors were significantly associated with NEC in preterm infants. 20 The early enteral feeding of VLBW preterm babies does not rise the risk of NEC. 21 Enteral feeding and composition play a major role in the inhibition and treatment of NEC. Giving mother’s own breast milk and standardization of feeding regimens reduced a risk for NEC. There is growing evidence on the providing of specific human milk components and its consequence on the incidence of NEC. 22 Early feeding of babies with their own mother’s milk and prevention of bovine-origin products might decrease the risk of NEC, but the absolute decrease is small. 23 Prolonging small feeding volumes early in life declines the incidence of NEC in VLBW infants. 24
As explained above, the burden of NEC is growing worldwide. However, there is a lack of studies that have addressed the prevalence of NEC and associated factors among enteral fed preterm and LBW neonates in the study area and even in our country Ethiopia. Therefore, the aim of the present study was to determine the prevalence of NEC and associated factors among enteral fed preterm and LBW neonates. The findings of the present study would aware the hospitals, healthcare professionals, government, stakeholders, and the researchers.
Objectives
General Objective
To assess prevalence and associated factors of necrotizing enterocolitis among enteral fed preterm and low birth weight neonates admitted in selected public hospitals neonatal intensive care unit in Addis Ababa, Ethiopia.
Specific Objectives
To assess the prevalence of necrotizing enterocolitis among enteral fed preterm and low birth weight neonates admitted in selected public hospitals intensive care unit in Addis Ababa, Ethiopia.
To identify factors associated with necrotizing enterocolitis among enteral fed preterm and low birth weight neonates admitted in selected public hospitals intensive care unit in Addis Ababa, Ethiopia.
Methods
Study Area and Period
The study conducted in governmental hospitals that found in Addis Ababa capital city of Ethiopia. Recently, the city has thirteen public hospitals. Out of these, 9 of them are delivering neonatal intensive care services. From these 9 hospitals the study was done on only 3 of them selecting it with lottery method. Namely, they were Tikur Anbesa specialized hospital, Gandhi memorial hospital, and Yekatit 12 hospital medical college. The total number of preterm, very preterm, and very low birth weight infant’s average annual admission in Gandhi memorial hospital (GMH), Yekatit 12 hospital medical college (Y12HMC) and Tikur Anbesa specialized hospital (TASH) were 425, 650, and 820 respectively, at the current time. These made a total of 1895 preterm admission per year within these 3 hospitals only. The study was conducted from March 25/2020 to May 10/2020.
Study Design
An institution based retrospective cross-sectional study with document review method was used among preterm, very preterm, low birth weight, and VLBW infants who were admitted to the NICU of selected public hospitals.
Source of Population
The source of population included all neonates’ card who were admitted and treated in the NICUs of selected hospitals.
Study Population
The study population included all preterm, very preterm, low birth weight and VLBW infants’ cards who were admitted to the NICU from January 2019 to January 2020 and who fulfilled the inclusion criteria.
Eligibility Criteria
Inclusion criteria
All preterm neonates’ cards <37 completed weeks of gestation and birth weight below 2500 g neonate’s card were admitted in neonatal intensive care unit. All very preterm and VLBW infants’ card between the ages of birth to discharge who were admitted to the selected hospitals NICU from January 2019 to January 2020 for whom, gestational age and weight parameters were available and stayed for more than 72 hours were included in the study.
Exclusion criteria
Preterm neonates’ cards who died or were discharged before 72 hours of age, and neonates’ cards for whom the gestational age and weight measurements and/or other relevant clinical data were not documented or were incomplete were excluded from the study.
Sample Size Determination
The sample size was calculated by using a single population proportion formula. Due to absence of studies done in Ethiopia, the prevalence was considered to be 50% to calculate the sample size. The single proportion formula is stated as:
Sampling Technique and Procedures
A simple random sampling technique was used to select the hospitals and study participants’ medical record chart for document review. There were a total of 13 public hospitals in Addis Ababa city, of which 9 public hospitals were giving NICU service while the rest were not. Out of those 9 public hospitals, 3 public hospitals were selected by using simple random sampling (lottery) method. The total number of preterm, very preterm, and very low birth weight infant’s average annual admission were GMH (425), Y12HMC (650), and TASH (820). The calculated sample size was proportionally allocated for each hospital (Figure 1).
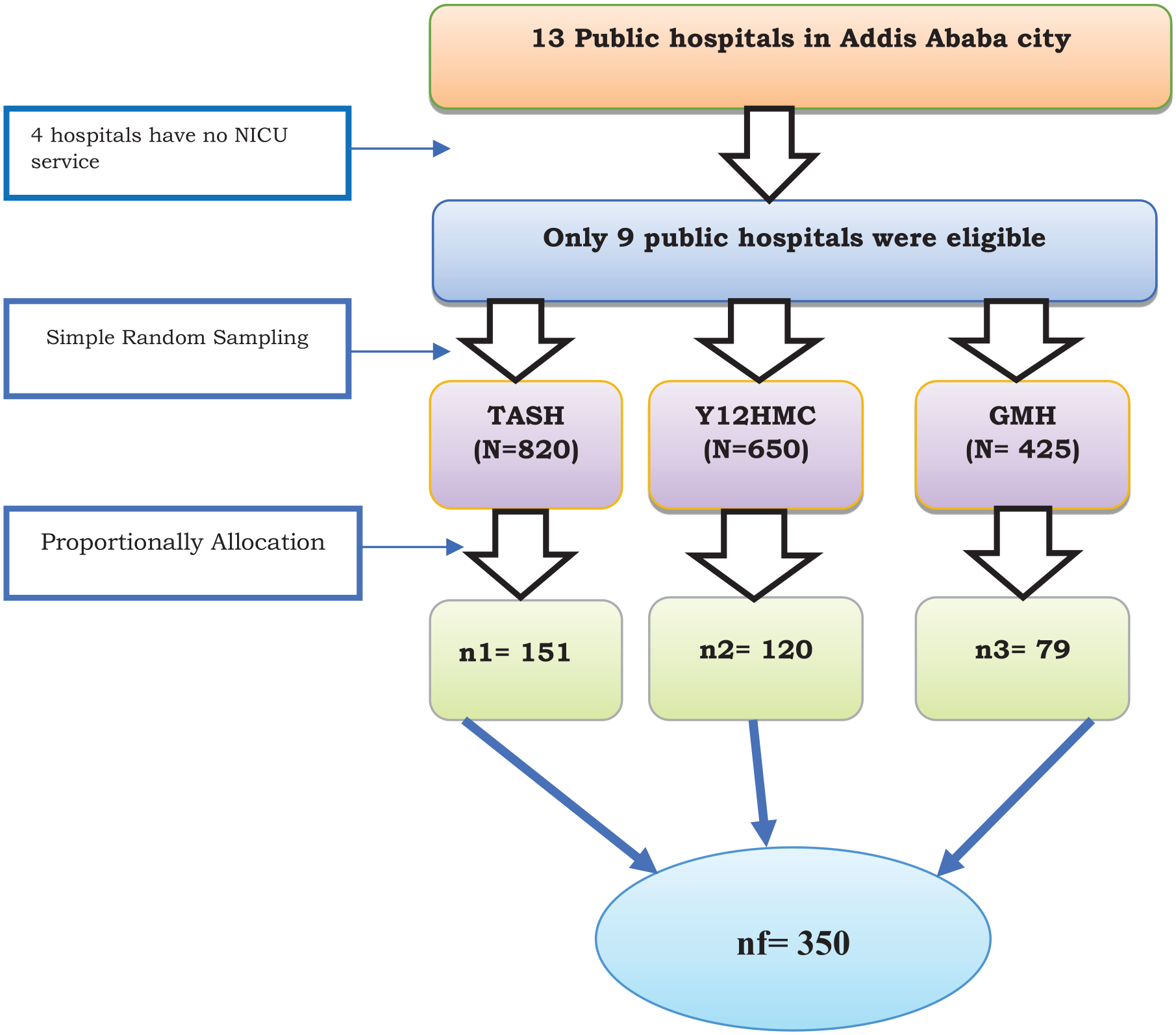
Schematic presentation of sampling procedure from each selected hospitals Addis Ababa, Ethiopia, 2020 (n = 350).
Study variables
Dependent variable
Prevalence of Necrotizing enterocolitis
Independent variables
Operational Definition
Data Collection Instrument
Structured document review questionnaire was used to collect the data. The questionnaires were adapted after an intense review of the related literatures25-30 and being modified to the local context and to the research objective. It was prepared in English language.
Data Collection Procedure
Data were collected by trained 3 BSc nurses and supervised by 2 MSc nurses. Chart numbers of infants’ card admitted to the NICU of selected public hospitals from January 1, 2019 to January 30, 2020 were retrieved from the NICU HMIS and medical record storeroom. Selection was made according to inclusion and exclusion criteria.
Data Quality Control
The quality of data was assured by using pre-test of the questionnaire on 5% of the calculated sample size in Zewditu memorial hospital to check for their accuracy and consistency prior to data collection period. Then the necessary modifications were made accordingly. Data collectors and supervisors were trained for 1 day on the data collection instrument and data collection procedure. The reliability of the questionnaire was checked by the reliability analysis and a cronbach’s alpha value was 0.89 which shows a reliable tool. Moreover, the supervisors and principal investigator were offered a feedback on daily basis for the data collectors. Finally, the collected data were checked carefully on a regular basis.
Data Processing and Analysis
The collected data were entered into Epi-data version 4.6.0.5 and then it was exported to Statistical Package for the Social Sciences (SPSS) version 25.0 (IBM Corporation, North Castle Drive, Armonk, NY, USA) for statistical analysis for further analysis. Descriptive statics such as frequency, percentage, means, and standard deviation was used to describe the data.
Bivariable and multivariable logistic regression analysis was done to find associated between dependent and independent variables. All independent variables with P-value of <.25 in bivariable logistic regression analysis were entered into multivariable logistic regression model to identify variables associated with NEC. Both crude odds ratio (COR) and adjusted odds ratio (AOR) with the corresponding 95% confidence interval (CI) were calculated to display the strength of the association. Model fitness was checked by Hosmer-Lemeshow’s goodness-of-fit test for NEC while the result was P-value = .543. Finally, P < .05 were considered statistically significant.
Result
Characteristics of the Neonates Admitted to NICU
A total of 350 participants were enrolled in to the study resulting in the response rate of 99.43%. More than half 184 (52.6%) of them were male. The majority 290 (82.9%) of them were born in the hospitals of a study area. About 46 (13.1%) of them were faced IUGR. The majority 123 (35.1%) of them were (32 + 1 to 34) weeks gestational age (Table 1).
Characteristics of Neonates Admitted to NICU in Selected Public Hospitals in Addis Ababa, Ethiopia, 2020 (n = 350).

Prenatal and Intrapartum Factors
The majority of 199 (56.9%) of them were delivered through cesarean section.
About199 (56.9%) of neonates were born from primipara mother. Among 350 study subject of neonate’s mother, 67 (19.1%) of them had a prolonged labor and 65 (18.6%) of neonate’s mothers had a maternal chronic disease during pregnancy (Table 2).
Prenatal and Intrapartum Factors in Selected Public Hospitals in Addis Ababa, Ethiopia, 2020 (n = 350).

Description of Neonates’ Characteristics by Enteral Milk Feed Initiation
The majority 326 (93.1%) of them were received trophic feeding. Most 287 (82%) of them were fed breast milk. The higher proportions 276 (78.9%) of admitted premature neonates to neonatal ICU has been fed by NGT. About 271 (77.4%) of the baby established full enteral milk feeds. Concerning to the enteral feed volume before onset of NEC; 179 (51.1%) of them done trophic feeding (Table 3).
Description of Neonates’ Characteristics by Enteral Milk Feed Initiation in Selected Public Hospitals in Addis Ababa, Ethiopia, 2020 (n = 350).

Description of Clinical Factors to the Diagnosis of NEC
From the study neonates admitted to NICU, 14 (4.0%) of them had congenital anomalies. Eighty-three (24.9%) of them had developed failure to breath or resuscitated after birth. Two hundred fifty-seven (73.4%) of them had a respiratory distress. Three hundred twenty-one (91.7%) of them had diagnosed with early/late onset neonatal sepsis. About 31(8.9%) of them had blood/exchange transfusion in the 48 hours prior to NEC diagnosis (Table 4).
Description of Clinical Factors to the Diagnosis of NEC on Premature and Low Birth Weight Infants in Selected Public Hospitals in Addis Ababa, Ethiopia, 2020 (n = 350).

Prevalence of Necrotizing Enterocolitis
The prevalence of NEC among enteral fed preterm and low birth weight neonates admitted in selected public hospitals intensive care unit was (25.4%) (n = 89, 95% CI, [21.1, 30.0]) (Figure 2).
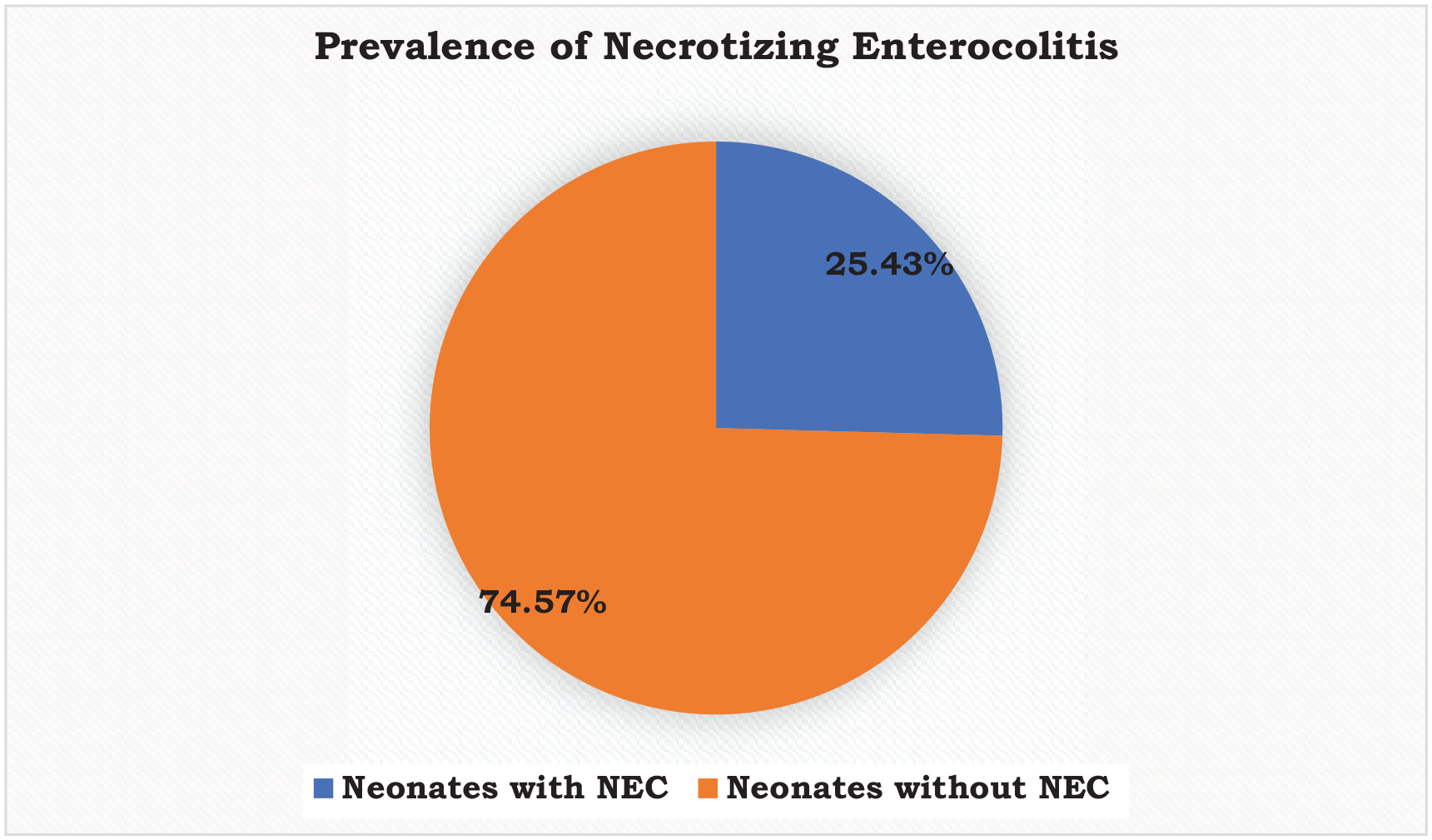
The prevalence of necrotizing enterocolitis among enteral fed preterm and low birth weight neonates admitted in selected public hospitals intensive care unit in Addis Ababa, Ethiopia, 2020 (n = 350).
Factors Associated with Necrotizing Enterocolitis
Bivariable logistic regression analysis was done to find variables associated with NEC. All independent variables with P-value of <.25 in bivariable logistic regression analysis were entered into multivariable logistic regression model to identify variables associated with NEC.
Gestational age, birth weight, gender, APGAR score, IUGR, prolonged labor, maternal chronic disease /Hypertension, maternal infection, chorioamnionitis, mother took drug, steroid drug, failure to breath/resuscitated, respiratory distress syndrome, use of CPAP ventilation, received trophic feed, age of milk fed started, type of milk fed used by neonates were entered into multivariable logistic regression model. Gestational age, birth weight, APGAR score, prolonged labor, maternal chronic disease /hypertension, chorioamnionitis, failure to breath/resuscitated, use of CPAP ventilation, and type of milk fed used by neonates were factors significantly associated with NEC.
The odds of having a NEC among neonates who aged ≤28 weeks gestational age and (28 + 1 to 32 weeks) were 3.94 times (AOR = 3.94, 95% CI [2.67, 9.97]) and 3.65 times (AOR = 3.65, 95% CI [2.21, 8.31]) higher than neonates aged (34 + 1 to 36 + 6 weeks) of gestational age, respectively. The likelihood of having a NEC among neonates who had birth weight of (1000-1499 g) were 2.29 times (AOR = 2.29, 95% CI [1.22, 4.33]) folds more as compared with neonates who had birth weight of (1500-2499) g.
Likewise, neonates who had APGAR score ≤3 were 2.34 times (AOR = 2.34, 95% CI [1.32, 4.16]) more likely to have a NEC when compared to neonates who had APGAR score ≥7. The odds of having a NEC among neonates who were born from mothers who had prolonged labor were 2.21 times (AOR = 2.21, 95% CI [1.35, 6.38]) higher than neonates who were not born from mothers who had prolonged labor.
Besides, the likelihood of having a NEC among neonates who were born from mothers who were with maternal chronic disease particularly hypertension was 3.2 times (AOR = 3.2, 95% CI [1.70, 5.90]) higher than their contraries. Neonates who were born from mothers who were with Chorioamnionitis were 4.8 times (AOR = 4.8, 95% CI [3.9, 13]) more likely to have a NEC when compared to their contraries. The odds of having a NEC among neonates who were faced failure to breath/resuscitated were 2.1times (AOR = 2.1, 95% CI [1.7, 4.4]) higher than neonates who were not faced failure to breath/resuscitated.
Furthermore, the likelihood of having a NEC among neonates who had CPAP ventilation were 3.7 times (AOR = 3.7, 95% CI [1.50, 12.70]) higher than neonates who had not CPAP ventilation. The odds of having a NEC among neonates who fed mixed milk were 3.58 times (AOR = 3.58, 95% CI [2.16, 9.32]) more likely than neonates who fed breast/human milk (Table 5).
Bivariate and Multivariate Analysis of Factors Associated with Necrotizing Enterocolitis Among Enteral Fed Preterm and Low Birth Weight Neonates Admitted in NICU of Public Hospitals in Addis Ababa, Ethiopia, 2020 (n = 350).

Number in bold indicates statistically significant (P < .05), number 1 represents the reference category.
Abbreviations: COR, crude odds ratio; AOR, adjusted odds ratio; CI, confidence interval; CPAP, continuous positive airway pressure; APGAR, appearance, pulse, grimace, activity, and respiration; IUGR, intrauterine growth restriction.
Discussions
The present study was done to determine the prevalence of NEC and associated factors among enteral fed preterm and low birth weight neonates. This is because, knowing the prevalence of NEC and associated factors is a cornerstone for NEC management in order to control the burden of NEC because of its associated morbidity and mortality is growing substantially across the worldwide. The present study revealed that the prevalence of NEC among enteral fed preterm and low birth weight neonates was 25.4% (n = 89, 95% CI [21.1, 30.0]).
The present study finding was higher than a prospective cross-sectional survey conducted in the United Kingdom which reported the prevalence of NEC as 1.8% for winter period and 2.1% for summer period. 25 The variation might be due to the difference in study design which was prospective cross-sectional survey for the study of United Kingdom but retrospective cross-sectional document review for the present study. Besides, the difference could also be due to the difference in the level of economic growth, the United Kingdom is economically developed country whereas, unfortunately Ethiopia is economically developing country. In fact, this could have huge effect on the quality of healthcare service.
The present study finding was also higher than the study done in United States which has been reported the prevalence of NEC as 7%. 26 The difference might be due to that the differences in population segment, while the study of United States includes only the very low birth weight infants. Furthermore, there could be healthcare disparities which would have the great impacts since United States is economically developed countries.
The present study finding was also higher than a retrospective cohort study conducted in Duke intensive care nursery which was reported the incidence of NEC as 10.7%. 28 The possible explanation could be due to that the difference in population segment while the study of Duke intensive care nursery was included only very-low-birth-weight infants. The present study finding was also higher than the study done in Soroka University Medical Center results which reported the prevalence of NEC 8.0%. 30 The variation might be due to that the difference in population segment while the study of Soroka University Medical Center was included only very-low-birth-weight infants.
The present study finding was higher than the study conducted in National Institute of Child Health and Human Development (NICHD) Neonatal Research Network which reported the prevalence of proven NEC 10.1%. 29 The variation might be due to that the difference in population segment while the study of National Institute of Child Health and Human Development (NICHD) Neonatal Research Network was included only very-low-birth-weight infants. The present study finding was higher than the study done in China which reported the prevalence of NEC 4.87%. 31 The possible justification could be that due to the healthcare disparities whereas the China has highly improved with their economic development when compared with that of Ethiopia, the poor country.
The odds of having a NEC among neonates who aged ≤28 weeks gestational age and (28 + 1 to 32 weeks) were 3.94 times (AOR = 3.94, 95% CI [2.67, 9.97]) and 3.65 times (AOR = 3.65, 95% CI [2.21, 8.31]) higher than neonates aged (34 + 1 to 36 + 6 weeks) of gestational age, respectively. This finding was supported by a systematic review which reported that low gestational age was a significant prognostic factors for NEC. 32 This finding was also supported by the study conducted in Swedish which reported that different patterns of associations were seen in the subgroups of different gestational age and NEC. 33 This might be due to that the smaller the gestational age of the neonates, the immature their immunity system. In fact, as the gestational age of the neonate increases, their immunity system get matures and would have the potential to protect them from different problems.
The likelihood of having a NEC among neonates who had birth weight of (1000-1499 g) were 2.29 times (AOR = 2.29, 95% CI [1.22, 4.33]) folds more as compared with neonates who had birth weight of (1500-2499) g. This finding was supported by the study done in National Institute of Child Health and Human Development (NICHD) Neonatal Research Network which reported birth weight as significant risk factors for NEC. 28 This finding was also supported by a systematic review which reported that a low birth weight was a significant prognostic factors for NEC. 32 This finding was also supported by the study conducted in Swedish which reported that birth weight has an association with NEC. 33 This finding was also supported by study done on predictors of NEC in preterm growth-restricted neonates showed that birth weight remains the predominant risk factor for NEC. 34 This finding was also supported by a research done in Polish which has been reported that a high risk of developing NEC is closely associated with VLBW. 35 This might be due to that the low birth weight could indicate the problem associated with nutrition. Whereas, the nutrition has a great effect on the maturity of the immunity system of the neonates.
Neonates who had APGAR score ≤3 were 2.34 times (AOR = 2.34, 95% CI [1.32, 4.16]) more likely to have a NEC when compared to neonates who had APGAR score ≥7. This finding was supported by a retrospective case-control study which has been found that NEC infants had a significantly higher frequency of APGAR score <7 at 1 and 5 minutes when compared with the control group. 36 This finding was also supported by a prospective multicenter investigation conducted in United States which has been reported that APGAR score deterioration were a determinants factor for NEC. 37
The odds of having a NEC among neonates who were born from mothers who had a prolonged labor were 2.21 times (AOR = 2.21, 95% CI [1.35, 6.38]) higher than neonates who were not born from mothers who had prolonged labor. This finding was supported by a research done in Polish which has been reported that a high risk of developing NEC is closely associated with inflammation of the amnion during labor. 35 This finding was also supported by a retrospective case-control study which has been found that NEC infants had a significantly higher frequency of prolonged rupture of membranes when compared with the control group. 36 So that, considering these findings as a contribution if a prolonged labor is occurred it will further facilitate the spread of infection while this could have the large contribution for the risk of NEC development. Furthermore, this might be described as maternal infection and prolonged labor increase the potential of neonatal infection which results in increased determinant factors of NEC.
The likelihood of having a NEC among neonates who were born from mothers who were with maternal chronic disease particularly hypertension was 3.2 times (AOR = 3.2, 95% CI [1.70, 5.90]) higher than contraries. This finding was supported by the study done in Soroka University Medical Center which reported that maternal hypertension was an independent risk factor for the development of NEC in preterm neonates of very-low-birth-weight. 30 This finding was also supported by the study conducted in Swedish which reported that preeclampsia has an association with NEC. 33 In fact, maternal vascular disorders may play a significant role in the development of NEC.
Neonates who were born from mothers who were with chorioamnionitis were 4.8 times (AOR = 4.8, 95% CI [3.9, 13]) more likely to have a NEC when compared to their contraries. This finding was supported by the study conducted in Morristown Memorial Hospital, New Jersey showed that histological chorioamnionitis substantially rises the risk of earlier delivery and neonatal mortality and vascular and coagulation placental findings rise the risk of NEC. 38 This finding was also supported by the systematic review and meta-analysis which indicated that chorioamnionitis was a risk factor for NEC. 39 This finding was also supported by a retrospective case-control study which has been found that NEC infants had a significantly higher frequency of chorioamnionitis when compared with the control group. 36
The odds of having a NEC among neonates who were faced failure to breath/resuscitated were 2.1 times (AOR = 2.1, 95% CI [1.7, 4.4]) higher than neonates who were not faced failure to breath/resuscitated. This finding was supported by a retrospective case-control study which has been found that NEC infants had a significantly higher frequency of respiratory problems when compared with the control group. 36
The likelihood of having a NEC among neonates who had CPAP ventilation were 3.7 times (AOR = 3.7, 95% CI [1.50, 12.70]) higher than neonates who had not CPAP ventilation. This finding was supported by a systematic review which reported that assisted ventilation was a significant prognostic factors for NEC. 32
The odds of having a NEC among neonates who fed mixed milk were 3.58 times (AOR = 3.58, 95% CI [2.16, 9.32]) more likely than neonates who fed breast/human milk. This finding was supported by a study conducted in Intermountain Healthcare which reported that the prevalence of NEC during the first week could be decreased by feeding them human milk exclusively. 27 This finding was also supported by a retrospective analysis which reported human milk should always be the diet of choice in preterm infants. The use of human milk is associated with a lower rates of NEC. 40 This finding was also supported by a systematic review which reported human milk should be used when possible to decrease the incidence of NEC. 41 The possible justification could be that human milk has very important protective factors for various problems including the intestinal mucosal layer of the neonates.
Conclusion
The present study revealed that the prevalence of NEC among infants was high. The multivariable logistic regression analysis revealed; Gestational age, birth weight, APGAR score, prolonged labor, maternal chronic disease/hypertension, chorioamnionitis, failure to breath/resuscitated, use of CPAP ventilation, and type of milk fed used by neonates were factors significantly associated with NEC.
The present study finding gives an important evidence to aid the public health and preventive program to the societies. It also would support healthcare providers for the management of NEC. Besides, it also would encourage them to emphasis on and design the strategies to address this problem. Finally, we recommend that there is a need to initiate programs that could minimize this critical problem. All the concerned bodies should actively involve on this public issue to prevent or minimize the morbidity and mortality associated with NEC.
Limitation of the Study
The limitation of this study was the study design we have used, which as Institution based retrospective cross-sectional study.
Footnotes
Acknowledgements
We are grateful to Addis Ababa University, College of Health Sciences, School of Nursing and Midwifery for their compulsory assistance. Next, we would like to thank the supervisor, data collectors and hospitals.
Authors’ Contributions
Sitotaw Molla Mekonnen, Daniel Mengistu Bekele, Fikrtemariam Abebe Fenta, and Addisu Dabi Wake contributed to the conception of the study, data analysis, drafting or revising the article. Finally, all the authors gave final approval of the version to be published, and agrees to be accountable for all aspects of the work.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The present study was funded by Addis Ababa University.
Ethics Approval
The study was approved by the Institutional Review Board (IRB) of the Addis Ababa University. Then, the letter of permission was gained from the hospital director of Tikur Anbesa specialized hospital, Gandhi memorial hospital, and Yekatit 12 hospital medical college. Finally, Since the data was collected by neonates’ medical record chart review, confidentiality of the information obtained from the neonates’ chart were maintained.
Availability of Data and Materials
The data used to support the findings of this study are on the hands of the corresponding author.