
Abstract
Background:
Early enteral feeding initiation for preterm neonates is a vital part of neonatal intervention for overall outcomes. There are few dates. We aimed to assess the time to enteral feeding initiation and its associated factor among preterm newborns admitted to the University of Gondar.
Method:
An institutional-based retrospective follow-up study was conducted from August 8, 2024, to December 30, 2024.
Result:
A total of 144 preterm newborns were followed for about 6452 person-hours of observation. The follow-up period ranged from 1 to 240 hours. Out of 144 preterm newborns, 51 (35.42%) initiated enteral feeding early within the first 24 hours. Variable that affects trophic feeding initiation were gestational age, small for gestational age, and presence of jaundice were significant and independent predictors of early initiation.
Conclusion:
The rate of early trophic feeding initiation was low in our institution.
Introduction
Preterm birth is defined as delivery before 37 weeks of gestation. It remains a significant global public health challenge, contributing substantially to neonatal morbidity and mortality.1,2 According to the World Health Organization (WHO), preterm birth complications are the leading cause of death among children under 5 years, accounting for approximately 1 million deaths annually. 2 In sub-Saharan Africa, the burden of preterm birth is particularly pronounced, where resource limitations exacerbate neonatal care challenges.3,4
Adequate nutrition is vital for the growth, development, and survival of preterm infants; however, feeding these infants poses a significant challenge due to their immature gastrointestinal systems and increased vulnerability to complications such as necrotizing enterocolitis (NEC).5 -7 Trophic feeding, also known as minimal enteral feeding, is a strategy used to stimulate gut maturation and improve feeding tolerance by administering small volumes of enteral feeds during the early postnatal period. 8 This approach not only primes the gastrointestinal tract but also reduces the risk of feeding-associated complications, thereby promoting better outcomes for preterm infants. 9
The timing of initiating trophic feeding is a critical decision in neonatal care, and there are different views on when to start this feeding.10,11 Evidence suggests that early initiation of trophic feeding, within the first 48 hours of life, may be beneficial in improving feeding outcomes and reducing hospital stay. 12 However, the decision is influenced by various clinical factors, including gestational age, birth weight, hemodynamic stability, and the presence of other comorbidities such as sepsis or respiratory distress syndrome. 13 In resource-limited settings, additional factors such as the availability of skilled healthcare providers and access to breast milk or donor milk also play a significant role.14,15
Despite the recognized importance of trophic feeding, there is limited research on its implementation and predictors in low-resource settings such as Ethiopia. The University of Gondar Comprehensive Specialized Hospital, a tertiary referral center, provides care to a substantial number of preterm infants annually. However, the timing and determinants of initiating trophic feeding in this setting remain poorly understood. Understanding these factors is crucial for optimizing feeding practices and improving neonatal outcomes.
This study aims to investigate the time to initiate trophic feeding and its predictors among preterm infants admitted to the University of Gondar Comprehensive Specialized Hospital. By identifying the determinants of early feeding initiation, this research seeks to contribute to evidence-based neonatal care protocols tailored to resource-constrained settings. Furthermore, it addresses a critical gap in the literature by providing context-specific insights that can inform policy and practice in Ethiopia and similar settings.
The findings of this study have the potential to enhance the quality of neonatal care by promoting timely and appropriate feeding practices. This, in turn, can reduce the risk of feeding-related complications and support better growth and developmental outcomes for preterm infants.
Methods and Materials
Study Setting, and Period
The study was conducted at the University of Gondar Comprehensive Specialized Hospital (UOGCSH) neonatal intensive care unit (NICU) from August 8, 2024, to December 30, 2024, for 5 months. UOGCSH is the oldest tertiary teaching hospital, which is in northwest Ethiopia, located in Gondar town, 725 km northwest of the capital city of the country, Addis Ababa. The hospital gives comprehensive pediatrics care, among which neonatal intensive care is the one that is organized into different service areas, including term, preterm, kangaroo mother care (KMC), and maternal waiting rooms. The major services are general neonatal care, blood and exchange transfusion, phototherapy, and ventilation support such as continuous positive airway pressure (CPAP). These services are provided by senior pediatricians, residents, general practitioners, and neonatal nurses.
Study Design
This is an institution-based retrospective follow up study.
Population
Source Population
All preterm infants admitted to the neonatal intensive care unit preterm compartment at UOGCSH in northwest Ethiopia.
Study Population
All preterm infants were admitted to the neonatal intensive care unit preterm compartment during the data collection period at the UOGCSH in northwest Ethiopia.
Sample Size and Sampling Procedure
The sample size was calculated by using RStudio (version 2024.09.1-394) considering statistical assumptions: significant level (α) 0.05, power 80%, Za/2 = Z value at 95% confidence interval = 1.96, probability of feeding initiation = 29%, Hazard Ratio (HR) = .5, survival probability = .5, and the proportion of withdrawal = .10. Though the calculated sample size was 137, we collected 144 preterm neonates to increase the power of the study. We use consecutive sampling methods within the data collection period. Those who had already started feeding before the time of admission, either at home or referred to facilities, and those with congenital anomalies with obstructions, like gastroschisis and omphalocele, were excluded from this study.
Variables of Study
Outcome Variable
Time to initiate trophic feeding was the outcome variable of this study.
Independent Variables
Socio-demographic characteristics (gestational age, birth weight, age of the mother, residence, and educational status) and neonatal-related factors (first-minute APGAR score, fifth-minute APGAR score, hemodynamic instabilities, congenital abnormality, respiratory distress syndrome, blood transfusion, and phototherapy) maternal-related factors (sero-status of the mother, hypertensive disorder of pregnancy, mode of delivery, birth type, place of delivery, parity, and diabetes mellitus).
Operational Definitions
Early feeding: neonates initiated trophic feeding within 24 hours of birth.16,17
Survival time: the length of time in hours from birth to the first trophic feeding.
Event: the neonates who had started their first trophic feeding within the follow-up period.
Censored: neonates who died left against medical advice, were transferred, or were referred before starting trophic feeding, or not started at end of follow-up.
Follow up time: time from birth to the first 10 days of life.
Trophic feeding: the university hospital follows national guidelines that are based on the patients’ gestational age and birth weight, but we define trophic feeding as first minimal enteral feeding to prime the gut regardless of method or volume.
Data Collection Tools and Procedure
A structured data extraction form with English language was prepared and used to extract information from patient charts. The data extraction checklist and questionnaire were adapted from different related literature, books, and guidelines. Data was collected by a trained general practitioner. The principal investigator checked the completeness and consistency of the data daily.
Data Analysis and Interpretation
Data were checked for completeness, coded manually, and entered into an Excel spreadsheet, then exported to STATA version 17 for analysis. Both descriptive and analytical statistical procedures were utilized. Descriptive statistics like percentage, mean, median, standard deviation, and IQR were used for the presentation of characteristics of patients. Tables and graphs were used for data presentation. Factors associated with delayed feeding initiation were identified using survival analysis. Specifically, univariate and multivariate Cox regression models were fitted. From univariate regression, a variable with a P-value less than .2 was exported into multivariable COX regression analysis. The results of the regression analysis were reported as a hazard ratio with a 95% confidence interval. Finally, variables with P-values < .05 in the multivariate COX regression model were taken as statistically significant.
Result
Socio-Demographic Characteristics
A total of 144 preterm neonates were included in the analysis with a 100% response rate. The mean gestational age of the preterm neonates was 32.34 weeks (SD ± 1.9) with a range of 28 to 36 weeks. More than half (60.4%) of the neonates were male. Except for one preterm neonate, others were low birth weight with a median weight of 1385 grams and an IQR of 1270 to 1450 g. From the total preterm deliveries, 39 (27.1%) were cesarean deliveries (Table 1).
Socio Demographic and Clinical-Related Characteristics of the Study Participants.

Abbreviations: AGA, appropriate for gestational age; APGAR, appearance, puls, grimace, activity and respiration; HAS, hospital acquired sepsis; NEC: necrotizing enterocolitis; RDS, respiratory distress syndrome; SGA, small for gestational age.
Sociodemographic and Obstetrics Related Characteristics of the Mother
More than two-thirds (67.36%) of the mothers were from urban areas, and 60% were found in the age group of 20 to 35 years old. Of the total 7 mothers, 4 (4.86%) were HIV positive. The median income of the family was 8250, with the interquartile range of 5000 to 12 000 Ethiopian birr (Supplemental File).
Survival Status of Neonates on Time to Initiate Trophic Feeding and Incidence of Feeding Initiation
More than 35% of the preterm neonates initiated Trophic Feeding (TF) within the first 24 hours, and the median time to initiate TF was 36 hours with an IQR of 23.5 to 70 hours. A total of 6452 person-hours of risk time were followed for 144 preterm newborns. The follow-up period ranged from 1 to 240 hours. Out of 144 preterm newborns, 51 (35.42%, 95% CI: (27.5%-43.3%)) were starting trophic feeding, and the remaining 93 (64.58%) were censored. The overall incidence of initiating trophic feeding (TF) was 7.9 per 1000-person hours of observation. The cumulative probability of initiating trophic feeding at 72 hours was 79.8%.
The risk of necrotizing enterocolitis was higher among preterm neonates who started late compared with those who started early that accounts for 74.07% among who developed necrotizing enterocolitis (Supplemental File).
Differences in all variables at baseline between strata were determined using the log-rank (χ2) test, and the equality of hazard was assessed for the different explanatory variables. A Kaplan-Meier failure curve was plotted for gestational age (P value = .0001), and weight for gestational age (P value = .0001) shows a significant difference (Figures 1 and 2).

Kaplan-Meier failure (trophic feeding initiation) estimates curves by gestational age.

Kaplan-Meier failure (trophic feeding initiation) estimates curves by weight for gestational age.
Predictors of Early Trophic Feeding Initiation at University of Gondar Comprehensive Specialized Hospital
The Cox proportional hazards model was fitted to identify predictors of mortality. From the multivariate analysis, gestational age ≥ 34 weeks, small weight for age, and presence of jaundice were predictors of early trophic feeding initiation. The hazard of early trophic feeding initiation was 2.70 times higher for preterm neonates with a gestational age ≥ 34 weeks (AHR = 2.70, 95% CI: 1.33-5.49) when compared with preterm neonates with a gestational age < 34 weeks and 4.17 times higher in preterm neonates who were small for gestational age (AHR = 4.17, 95% CI: 2.04-8.54) compared with preterm neonates having an appropriate weight for gestational age. Similarly, the hazard of early trophic feeding initiation was 1.96 times higher for preterm neonates who developed jaundice (AHR = 1.96, 95% CI: 1.11-3.45) compared with those who didn’t develop jaundice (Table 2).
Predictors of Time to Initiate TF Among Preterm Neonates Who Were Admitted to NICU at University of Gondar Comprehensive Specialized Hospital, Northwest Ethiopia (n = 144).
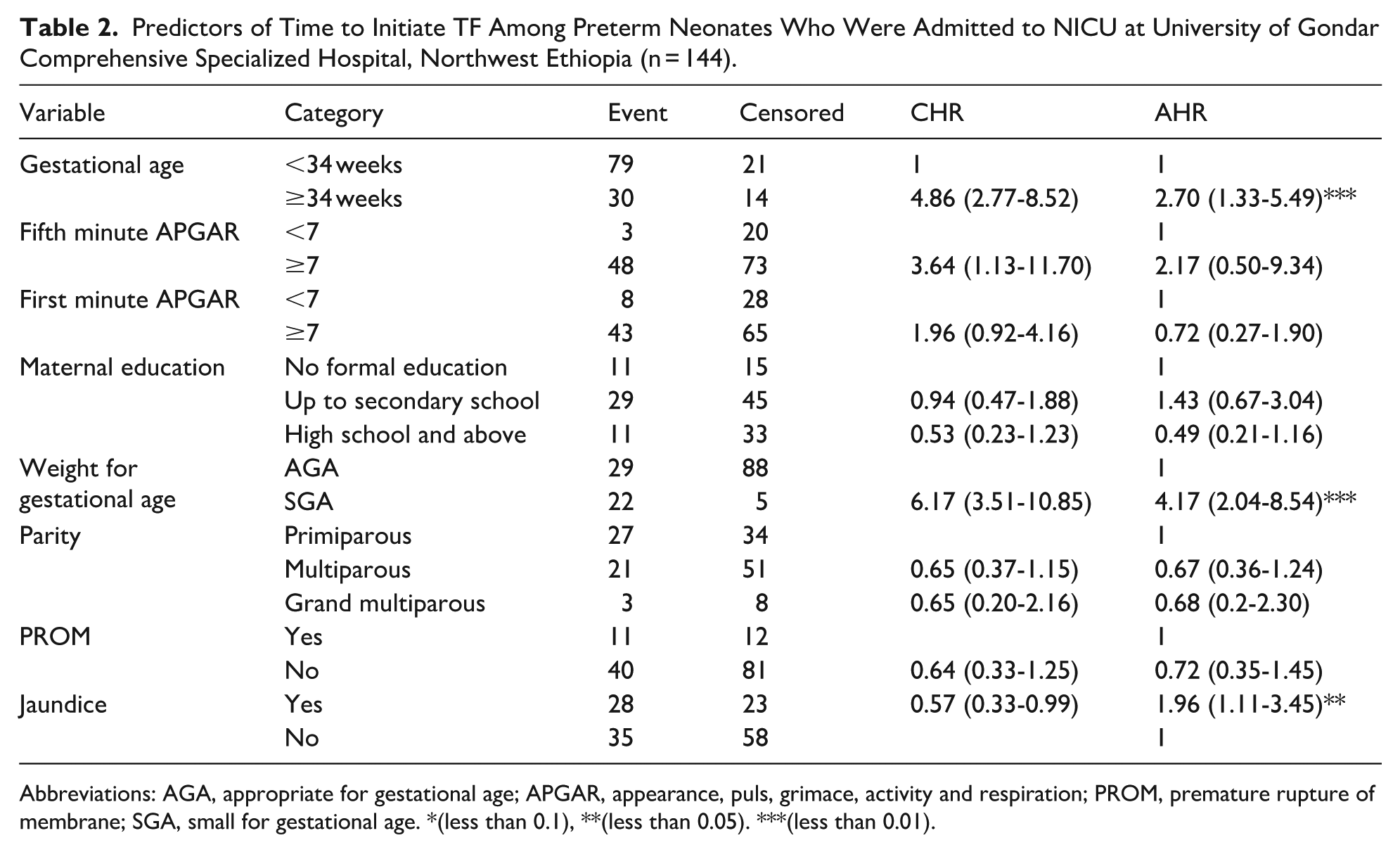
Abbreviations: AGA, appropriate for gestational age; APGAR, appearance, puls, grimace, activity and respiration; PROM, premature rupture of membrane; SGA, small for gestational age. *(less than 0.1), **(less than 0.05). ***(less than 0.01).
Discussion
This study found that over 35% of preterm neonates initiated trophic feeding (TF) within the first 24 hours of life. This finding contrasts with earlier systematic reviews and meta-analyses, which recommended initiating TF within a 72-hour window8,18 or within 48 hours. 19 However, our result aligns with more recent recommendations that support initiation within 24 hours.20,21 This study aimed to evaluate local practices against these evolving evidence-based guidelines.
The proportion of early TF initiation in this study was 35.42%, with an incidence rate of 7.9 per 1000 person-hours of observation. This is consistent with a study from northwest Ethiopia, 20 a similarity potentially attributable to comparable populations, clinical settings, and levels of expertise within Ethiopia. This finding is further supported by a study conducted at Chris Hani Baragwanath Academic Hospital. 22
Conversely, our result is lower than the rate of 59.5% reported in a national multicenter cohort study in China 5 and another study from Iran. 12 This discrepancy may be due to the larger sample sizes, greater availability of expert neonatologists, and more advanced infrastructure for early complication detection in those settings.
However, when compared to larger, multicenter data analyses, the rate of early trophic feeding initiation in this study was higher. Specifically, one multicenter study reported a rate of 24%, and another study conducted in Addis Ababa reported 22.1%, indicating that the performance in the present study was considerably better21,23
The hazard of initiating early trophic feeding was 2.70 times higher for preterm neonates with a gestational age ≥34 weeks. This is likely attributable to the greater physiological maturity of the gastrointestinal system in more mature infants. In contrast, neonates of lower gestational ages are more susceptible to necrotizing enterocolitis and feeding intolerance, which often necessitates a delay in feeding initiation. This finding is supported by international research confirming that a gestational age <34 weeks decreases the likelihood of early feeding initiation.20,21,24
Conversely, the hazard of early trophic feeding initiation was 4.17 times higher in small for gestational age (SGA) preterm neonates compared to those with an appropriate weight for gestational age (AGA). This finding contradicts studies from northwest Ethiopia and Greece.20,25 The discrepancy may be explained by the fact that SGA infants often experience cumulative nutrient deficits due to intrauterine malnutrition, prematurity, and other morbidities, which typically lead to feeding intolerance and delayed feeding initiation. In contrast, another study from Ethiopia found that SGA status itself did not significantly affect the time to initiation of trophic feeding; rather, birth weight was the more influential factor. 21
Preterm neonates who developed jaundice exhibited a 1.96 times higher hazard of early trophic feeding initiation compared to those who did not. This finding is challenging to explain pathophysiologically. Jaundice often results from conditions such as sepsis or immune-mediated hemolysis, which are typically associated with a delay in feeding initiation. Furthermore, the treatment for jaundice (eg, phototherapy) can itself interrupt feeding and delay the time to reach full enteral feeds.26,27
However, it is also established that delayed or insufficient feeding can increase the risk of neonatal jaundice, particularly breastfeeding failure jaundice. Conversely, early, frequent, and effective feeding is thought to help prevent and treat hyperbilirubinemia by promoting bowel movements and reducing enterohepatic circulation of bilirubin.28,29
In this study, respiratory distress syndrome, perinatal asphyxia, and sepsis were not statistically significant predictors of feeding initiation timing. Although not statistically significant, the incidence of necrotizing enterocolitis (NEC) was lower among neonates who started early feeding. This observation is supported by a previous systematic review 8
Limitation of the Study
This study has several limitations. Its single-center design and relatively small sample size may limit the generalizability of the findings and reduce the statistical power to detect significant associations. As a result, the true effect size in the broader population may not be fully captured, and the significance of some covariates may change in a larger study. Future research should involve a larger, multi-center randomized controlled trial to validate these findings.
Conclusion
In conclusion, though the risk of developing complications like necrotizing enterocolitis was low among neonates who started early trophic feeding, the initiation of early trophic feeding within 24 hours was suboptimal in our cohort of preterm neonates. We identified gestational age ≥ 34 weeks, small for gestational age status, and the presence of jaundice as independent facilitators of earlier feeding. While the first 2 factors are clinically intuitive, the association with jaundice is counterintuitive and warrants rigorous examination. To address this, we strongly advocate for large-scale multicentered studies to confirm this association and explore its underlying causes whether physiological or driven by specific unit protocols. Clarifying this relationship is critical for developing evidence-based feeding practices for all preterm infants.
Supplemental Material
sj-docx-1-gph-10.1177_30502225251401655 – Supplemental material for Time to Initiate Trophic Feeding and Its Predictors Among Preterm Infants at University of Gondar Comprehensive Specialized Hospital, Northwest Ethiopia
Supplemental material, sj-docx-1-gph-10.1177_30502225251401655 for Time to Initiate Trophic Feeding and Its Predictors Among Preterm Infants at University of Gondar Comprehensive Specialized Hospital, Northwest Ethiopia by Geta Bayu Genet, Yohannis Derbew Molla, Miteku Andualem Limenih and Destaye Shiferaw Alemu in Sage Open Pediatrics
Footnotes
Acknowledgements
We are thankful to the study participants and hospital administrators of the University of Gondar comprehensive specialized hospital. We also would like to acknowledge the department of pediatrics and child health.
Abbreviations
AGA Appropriate for gestational age
AHR Adjusted hazard ratio
ANC Antenatal care
APGAR Appearance, Puls, Grimace, Activity and Respiration
CHR Crude hazard ratio
CI Confidence interval
CPAP Continuous positive airway pressure
HAS Hospital acquired sepsis
HIV Human immunodeficiency viruses
IQR Interquartile range
KMC Kangaroo mother care
NEC Necrotizing enterocolitis
NICU Neonatal intensive care unit
PROM Premature rupture of membrane
RDS Respiratory distress syndrome
SD Standard deviation
SGA Small for gestational age
SVD Spontaneous vaginal delivery
TF Trophic feeding
UOG University of Gondar
UOGCSH University of Gondar comprehensive specialized hospital
WHO World health organization
Ethical Considerations
Ethical clearance was obtained from the University of Gondar, college of medicine and health science, school of medicine ethical review committee with reference no, SOM/246/2024.
Consent to Participate
Informed verbal consent was obtained from the caretakers. During the data collection the mother was clearly communicated with Amharic language (mother tongue of the region) that they can ask any question at any time during the data collection, or they can withdraw from the study at any time. The name or any other identifying information was not recorded on the data collection form, and all information taken from the chart was kept strictly confidential and in a safe place.
Author Contributions
GBG: Conceptualization, data collection, manuscript writing.
YDM: Data collection, entry.
MTA: Data analysis, draft writing.
HTA: Draft writing and revision.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Data is available from the corresponding author upon reasonable request.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.