
Abstract
Introduction:
Low birth weight (LBW) is a major contributor to neonatal mortality globally. In Uganda, a surge in LBW deliveries has been noted.
Methods:
This retrospective study assessed LBW prevalence, associated factors, and outcomes at Kayunga Regional Referral Hospital from February 2023 to February 2024. Of 1,177 neonatal admissions, 37.4% were LBW, with detailed analysis of 204 LBW weighing <2.0 kg requiring inpatient care. Data analyzed using STATA v15, logistic regression done for multivariate analysis. Ethical approval was obtained.
Results:
Lower gestational age (AOR = 333.04; 95% CI: 57.84-1917.53; P < .001), respiratory distress syndrome (AOR = 0.02; 95% CI: 0.01-0.29; P < .001) and apnea of prematurity (AOR = 0.08; 95% CI: 0.02-0.35; P < .001) were associated with LBW.
Conclusion:
Mortality was highest among very LBW (44.4%). The study highlights a high burden of LBW with poorer outcomes among very and extreme LBW neonates, underscoring the need to strengthen antenatal care and neonatal care services.
Introduction
Low birth weight (LBW) is a major global public health concern contributing to neonatal mortality and long term morbidity. An estimated 15 million preterm births occur annually worldwide, with the highest burden been observed in Sub-Saharan Africa (SSA) where prevalence rates sour up to 15%. 1 Complications related to prematurity are the leading cause of mortality among children under 5, accounting for approximately 1 million deaths in 2015. 2
In Uganda, the risk of preterm birth is estimated at 13% to 15%, and prematurity contributes to 28% to 31% of all neonatal deaths.2,3 The increased morbidity and mortality among preterm neonates result from their physiological and metabolic immaturity, which predisposes them to apnea of prematurity, hypothermia, infections, and prolonged hospitalization.4,5
A number of factors contribute to LBW, including maternal characteristics (eg, age, parity), socio-economic factors (eg, education level, employment status), biological or medical conditions such as multiparity, hypertension, malaria, urinary tract infections, and human immune deficiency (HIV). A study at Mulago Hospital reported the prevalence of LBW among teenage women (below 20 years) to be 25.5%. 6 Analysis of the demographic health survey data from 35 Sub Saharan Africa countries found that women with limited decision-making autonomy, marital instability (divorced/ separated women), and multiple pregnancies were associated with higher LBW rates. 7
Infectious diseases such as HIV, Malaria, and syphilis along with poor maternal nutritional status remain key contributors to LBW. Malaria parasites (particularly Plasmodium falciparum) can sequester in the placenta, obstructing blood flow and impairing fetal nutrition. 8 Similarly, food insecurity and maternal undernutrition, common in many parts of Uganda, have been consistently linked to LBW.9,10
Recent studies in Uganda report high prevalence of prematurity and its associated mortality.2,3 However, there is paucity of data about the prevalence of prematurity, it’s associated factors, and it’s outcomes especially in rural settings like Kayunga. This study therefore sought to determine the prevalence, associated factors, and outcomes of low-birth-weight neonates admitted to a tertiary referral hospital in Kayunga, Uganda. Understanding the prevalence, risk factors, and outcomes of LBW is essential to inform targeted interventions aimed at preventing and reducing both the preterm and neonatal morbidity and mortality.
Methods
Study Design and Period
An analytical retrospective cross-sectional study was carried out where patient medical records/files from February 1, 2023 to February 29, 2024 of neonates admitted at the Neonatal Care Unit (NCU) and the Special Care Unit (SCU) in the general pediatric ward of Kayunga Regional referral hospital.
Study Setting
The study was carried out at the SCU and NCU of Kayunga regional referral Hospital (KRRH), which is a regional referral and teaching hospital located in Kayunga district. The NCU at KRRH is level 2+ neonatal care unit. Kayunga Hospital has a capacity of about 200-bed and serves the districts of Buikwe, Buvuma, Jinja, Kamuli, Kayunga, Luwero, Mukono and Nakasongola (Figure 1). The labor suite conducts about 1000 to 1500 deliveries a month with an average of about 10 neonates having a low birth weight daily. The majority of the Low-birth-weight neonates are transferred in from the labor suite and other health facilities within the catchment area of KRRH. The NCU and pediatric general wards at the hospital have bed capacities of 25 and 70 respectively.

Map of Uganda showing the districts Kayunga regional referral hospital serves in Central Uganda during the study period, from February 2023 to February 2024.
Study Population
All patient files of neonates within the time period (February 1, 2023 to February 29, 2024) were screened for low birth weight (<2.5 kg) for overall prevalence of low birth weight in the facility. Neonates with birth weight >2.0 kg were eliminated from the analysis due to national guidelines for admission and the remaining neonates with low birth weight, <2.0 kg who met our eligibility criteria were recruited for analysis.
Inclusion and Exclusion Criteria
Sampling Technique
A total of 204 medical records (files) were sampled using the non-probability method of consecutive sampling. This was achieved in a 1 month data collection period.
Sample Size
Our sample size was calculated based on the Kish and Leslie formula (n = (Z^(2) pq)/e^2) where p is the prevalence of low-birth-weight neonates in Uganda. 11
Where;
n is the estimated sample size, Z is the statistic corresponding to the level of confidence which is 95%, in this case 1.96
P is the prevalence of low-birth-weight neonates, assuming a national prevalence of low birth weight being 14%. 12
e is the precision at 5%
A sample size of 185 was estimated
With 10% of estimated sample added on 19 to account for errors, missing and inaccurate data
Therefore, the final sample size was 204.
Data concerning age, education status, antenatal care, maternal infections, Co-morbidities and information on the baby were collected using a pre-tested structured data extraction tool.
Variables
The dependent variable in the study were low birth weight categories that is, low birth weight-LBW (<2500 and >1500 g), VLBW- Very low birth weight (<1500 and >999 g) and ELBW- Extremely low birth weight (<1000 g). The independent variables were sociodemographic factors, past obstetric and medical history of the mother, and neonatal factors (diagnosis, management instituted, and outcomes).
Patient Management
All patients admitted were managed using the Uganda clinical protocols for managing small and sick newborns 2023, Basic Pediatric Protocols 2023, and Uganda Clinical guidelines 2023. They were managed either in the NCU and/or SCU following 2 protocols. First, all sick neonates born in the hospital and less than 72 hours were admitted in the NCU. Second, those referred in or older than 72 hours were managed in the SCU. Utilizing the Uganda clinical protocols for managing small and sick newborns 2023 and the Basic Pediatric Protocols 2023, management involved utilizing medications like oxygen therapy, Continuous Positive Airway Pressure(CPAP), ampicillin, gentamycin, cefotaxime, metronidazole, amikacin, phenobarbitone, phenytoin, atropine, adrenaline, aminophylline, caffeine citrate, calcium gluconate, sildenafil, hydrocortisone, omeprazole, vitamin k, tranexamic acid, tetracycline eye ointment, nevirapine syrup, Dextrose 5%, dextrose 10%, crystalloids(lactated ringers and 0.9% sodium chloride) and salbutamol nebuls.
First line antibiotics were ampicillin and gentamycin and second line were cefotaxime and gentamycin which were used for the first and second protocols respectively.
All diagnoses were taken as final diagnosis basing on the diagnosis in the patient file records.
There was no surfactant therapy administration or assisted mechanical ventilation for the low-birth-weight neonates.
Nasogastric tubes were passed for feeding on day 1 and fluid management was instituted following the Uganda clinical protocols for managing small and sick newborns 2023.
Referrals were made where appropriate, specifically for surfactant administration, cardiac echocardiogram or mechanical ventilation.
Temperature control was done using exposure when febrile, and the neonates were put in an incubator and when stable, Kangaroo mother care was instituted.
Data Quality Control and Measurements
A standardized data extraction tool was designed to capture maternal and neonatal characteristics and outcomes. In this retrospective study, maternal sociodemographic and obstetric characteristics were abstracted from patient review cards, admission records, and maternity files that had been completed during routine clinical care. Variables such as maternal age, marital status, educational level, parity, antenatal care attendance, and medical or obstetric history were therefore obtained from documented hospital records rather than direct interviews with mothers. The neonatal characteristics, were abstracted from patient review cards, and hospital admission records made during their stay in the hospital. Thus, the neonatal variables such as birth weight, diagnoses and management details including prescribed medicines during admission, hospital admission days, use of surfactant and the outcomes were directly obtained from documented hospital records. In addition, Gestational age was obtained mainly from estimation of the last normal menstrual period of the mother, or ultrasound scan estimation findings of gestation age and if none was availed a modified Ballard was done for the neonate at the earliest possible time. This was also obtained from the patient records. Therefore, during data abstraction, responses were coded according to predefined categories developed from the variables available in the data source records.
Data Analysis
Extracted data from patient files was entered in a csv file, cleaned in pandas and exported to STATA v15 software for the analysis. Frequencies of LBW categories were calculated by expressing the number of LBW neonate category out of the total number of files included in the study as a percentage. On univariate analysis, categorical data (ie, age groups, sex, level of education, marital status and parity) was analyzed using descriptive statistics that is, frequencies, proportions and percentages. Continuous data was analyzed using mean, range, median and standard deviation. Medical records with missing data were excluded from the study if they did not have any information about the neonate.
Bivariate logistic regression analysis was used to identify the maternal and neonatal factors associated with low birth weight using estimated crude odds ratios with confidence intervals and corresponding P-values serving as the measures of association. Factors found with significant associations were selected for multivariate analysis.
At multivariate analysis, Ordinal logistic regression models were fitted to examine significant associations between maternal and neonatal factors with birthweight classification. The proportional odds assumption was evaluated using the Brant test. Model goodness-of-fit was assessed using likelihood ratio tests and pseudo R2 statistics. Multicollinearity among predictors was examined using variance inflation factors (VIF), with values greater than 5 considered indicative of problematic multicollinearity. Adjusted Odds ratios (AOR) were obtained to identify the significant associations. Associations were considered statistically significant at 95% confidence intervals, with P-values of less than .05.
Ethical Consideration
Before data collection, ethical approval was obtained from both the Mildmay Uganda Research & Ethics Committee (MUREC) and the Uganda National Council of Science and Technology (UNCST) under the number
Results
Out of a total of 1177 admissions during the period of review, 37.4% had low birth weight (<2.5 kg) where by 82.5% were classified as LBW, 14.5% as VLBW and 3.0% as ELBW.
Utilizing the Uganda clinical protocols for managing small and sick newborns 2023, 53.6% of the LBWs who weighed >2.0 and <2.5 kg were observed for 24 hours and allowed home on Kangaroo mother care while the 46.4% of the LBWs who weighed <2.0 kg were analyzed for the study. Among these, 62.2% were classified as LBW, 31.4% as VLBW, and 6.4% as ELBW (Figure 2).

Study flow chart of recruitment process for enrollment into the retrospective low birth weight study in Kayunga, from February 2023 to February 2024.
Regarding maternal age, nearly half of participants were aged 15 to 24 years (49.0%), followed by 25 to 34 years (27.0%) and 35 to 44 years (7.8%), while 16.2% had age recorded as unknown. Across all age groups, the majority of neonates were in the LBW category, with the highest proportion of LBW observed among mothers aged 35 to 44 years (81.2%; Table 1).
Sociodemographic Characteristics and Birth Weight Classification of Study Participants in Kayunga, from February 2023 to February 2024.
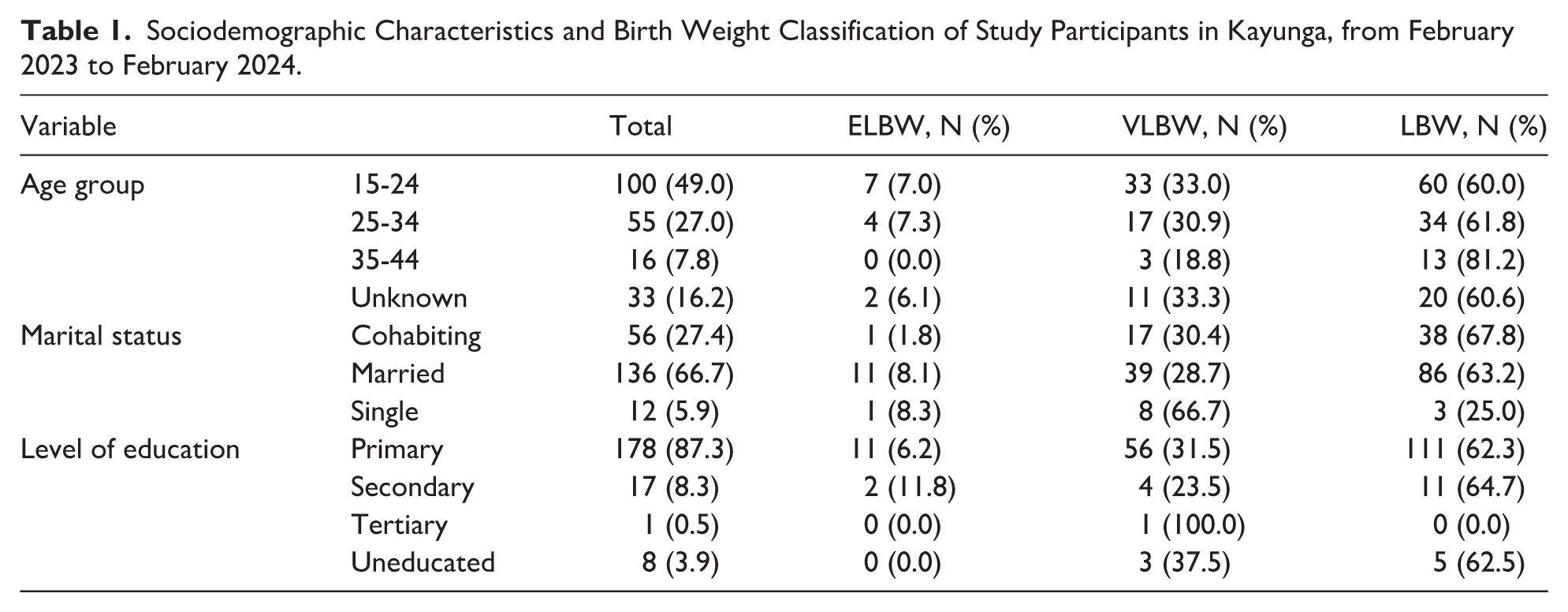
In relation to marital status, most mothers were married (66.7%), while 27.5% were cohabiting and 5.9% were single. Notably, a relatively high proportion of VLBW was observed among single mothers (66.7%), compared with married (28.7%) and cohabiting mothers (30.4%).
Most participants, (87.3%), had attained primary education while 8.3% had secondary education, 3.9% were uneducated, and only 0.5% had tertiary education. Across education levels, LBW remained the dominant category among the LBW classification (Table 1).
More than half of mothers had parity of 2 or more (55.9%), while 33.8% had parity of 1 with 10.3% unknown. LBW was common across all parity groups; however, mothers with parity 1 had a slightly higher proportion of VLBW (39.1%) compared with those with parity ≥2 (26.3%; Table 2).
Maternal History and Birth Weight Classification of Study Participants in Kayunga, from February 2023 to February 2024.

Antenatal care.
A history of obstetric complications was rare: 99.5% mothers reported no past obstetric complications, and only 0.5% reported a complication. Similarly, most mothers had no chronic medical illness (93.6%), while 6.4% reported chronic illness which was noted as HIV.
Most mothers attended antenatal care (ANC; 68.1%), while 31.9% did not attend. The majority had fewer than 4 ANC visits (83.8%), with only 16.2% reporting 4 or more visits (Table 2).
Almost all pregnancies were recorded as not carried to term (98.0%), with only 2.0% marked as carried to term. Most pregnancies were multiple gestations (76.0%), while 24.0% were singleton pregnancies (Table 2).
Of the 12 mothers that reported an illness during pregnancy, 41.7% reported being managed for Urinary tract infection (Figure 3). All mothers that were documented to having had an illness during pregnancy period received treatment.

Chart showing the maternal illness diagnosed during pregnancy of study participants in Kayunga, from February 2023 to February 2024.
In the Multivariate analysis, marital status was significantly associated with birth weight classification. Compared to cohabiting mothers, being single was associated with lower odds of having a low-birth-weight neonate (AOR = 0.22; 95% CI: 0.06-0.80; P = .022; Table 3).
Multivariate Analysis of Maternal Factors Associated with Low Birth Weight Among Study Participants in Kayunga, from February 2023 to February 2024.

Antenatal care.
Maternal age group showed no statistically significant association with birth weight category. Compared to mothers aged 15 to 24 years, those aged 25 to 34 years had similar odds (AOR = 1.03; 95% CI: 0.45-2.36; P = .948) and those aged 35 to 44 years had higher odds, though not significant (AOR = 2.90; 95% CI: 0.66-12.73; P = .159).
Education level, parity, ANC attendance (number of visits), Fansidar use, chronic medical illness status, illness during pregnancy, and plurality (singleton vs multiple gestation) were not significantly associated with birth weight classification (Table 3). The majority of babies born with low birth weight (<2.5 kg) and very low birth weight (<1.5 kgs) were of mothers with low parity. However, it is important to note that also majority of the mothers in the study were of low parity (Table 2).
Mothers who reported malaria during pregnancy, gave birth to children with very low birth weight (<1.5 kg; Figure 4). Mothers with pre-eclampsia and eclampsia gave birth to babies with low birth weight (<2.5 kg) however no significant association was found between mother’s past obstetric complications and low birth weight (Table 3).

Chart showing the frequency of maternal illnesses and associated categories of low birth weight among study participants in Kayunga, from February 2023 to February 2024.
The most made diagnoses were Respiratory distress syndrome 97.1%, neonatal sepsis 63.9%, presumed sepsis 35.6%, Neonatal jaundice 23.9%, Necrotizing enterocolitis 14.6%, Persistent Pulmonary Hypertension 3.4%, and Apnea of prematurity 3.4% (Figure 5).
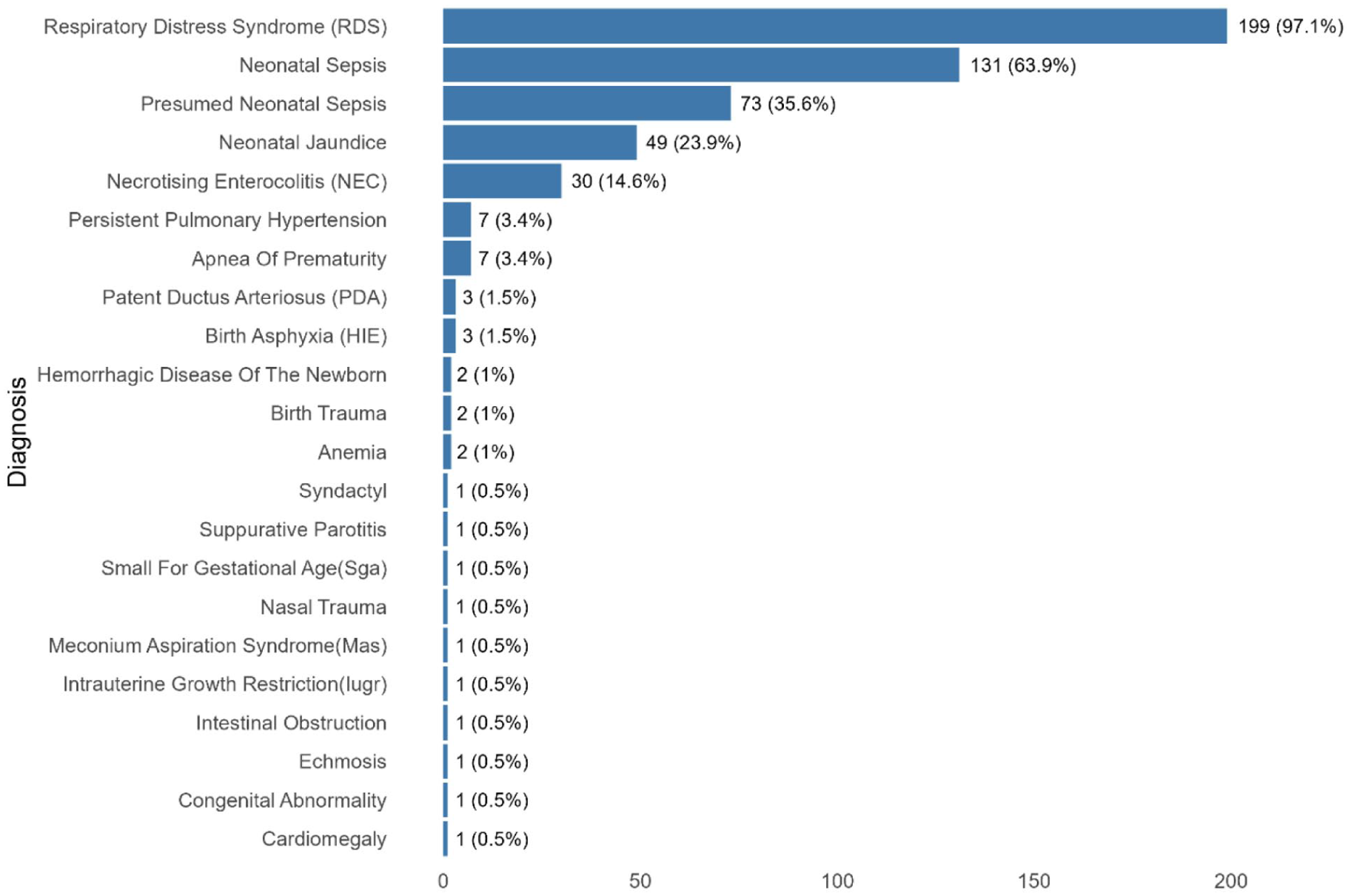
Chart showing the prevalence of neonatal diagnoses among the study participants in Kayunga, from February 2023 to February 2024.
The most encountered combined diagnoses were respiratory distress with either sepsis or presumed sepsis, necrotizing enterocolitis and jaundice (Figure 6).

Combination/ co-occurrences of the neonatal diagnoses among the low-birth-weight study participants in Kayunga, from February 2023 to February 2024.
Overall, nearly half of neonates (49.5%) had gestational age between 32 and 34 weeks with the lowest being ≤28 weeks at 8.3%. Gestational age showed a strong statistically significant association with birth weight category. Compared to neonates born at ≤28 weeks (reference), those born at 29 to 31 weeks had substantially higher odds of being in a higher birth weight category (AOR = 78.41; 95% CI: 14.00-439.23; P < .001), and those born at 32 to 34 weeks had even higher odds (AOR = 333.04; 95% CI: 57.84-1917.53; P < .001), suggesting that lower gestational age was strongly associated with low birth weight (Table 4).
Table Showing Neonatal Factors Associated with Low Birth Weight Among the Study Participants in Kayunga, from February 2023 to February 2024.

Regarding neonatal diagnoses, respiratory distress syndrome (RDS) was highly prevalent, reported in 97.5% neonates. A statistically significant association between RDS and birth weight classification (AOR = 0.02; 95% CI: 0.01-0.29; P < .001; Table 4).
In addition, apnea of prematurity, though uncommon (3.4%), showed a statistically significant association with birth weight category; neonates with apnea of prematurity had lower odds of being in a higher birth weight category (AOR = 0.08; 95% CI: 0.02-0.35; P < .001).
Neonatal sepsis was recorded in 62.7% neonates, while presumed neonatal sepsis occurred in 35.3%. However, neither neonatal sepsis (AOR = 0.70; 95% CI: 0.39-1.27; P = .243) nor presumed neonatal sepsis (AOR = 1.25; 95% CI: 0.69-2.26; P = .465) were significantly associated with birth weight classification. Similarly, neonatal jaundice, necrotizing enterocolitis (NEC), and persistent pulmonary hypertension these conditions did not show statistically significant associations with birth weight category (Table 4).
When disaggregated by birth weight category, mortality was highest among neonates in the VLBW group 44.4%; followed by LBW 33.3% and ELBW 22.2%. Discharge following improvement was most common among LBW neonates 68.8%; followed by VLBW 27.2%; and ELBW 4.0% (Table 5).
Neonatal Clinical Outcomes Per Birth Weight Classification of Study Participants in Kayunga, from February 2023 to February 2024.
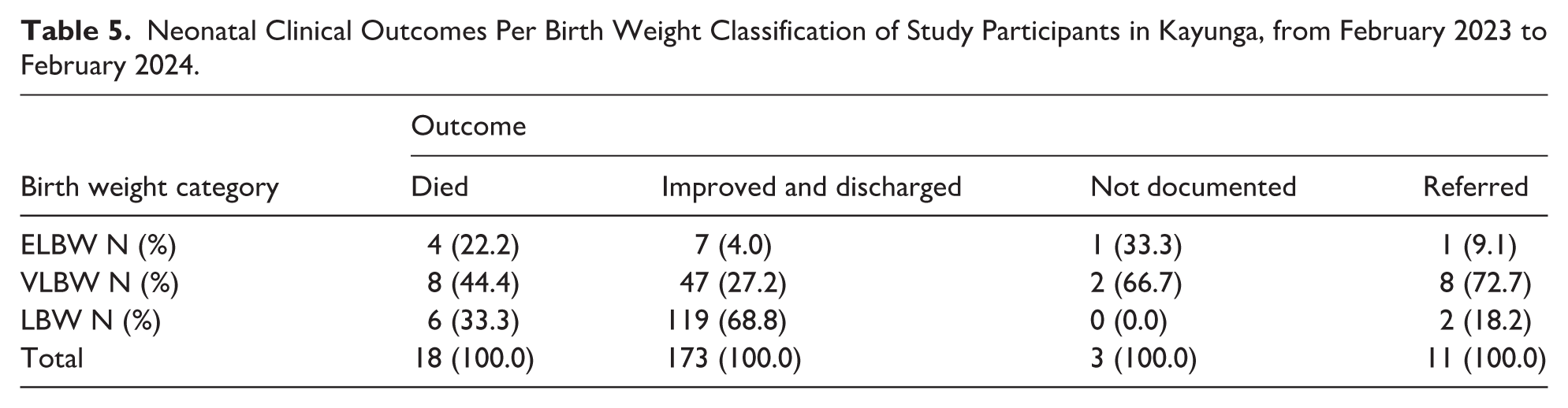
Table 5 summarizes neonatal clinical outcomes disaggregated by birth weight classification.
Low birth weight neonates with combination of diagnoses were sicker and had higher mortality (Figure 7). Those with a combination of Apnea of prematurity, presumed sepsis and RDS had a higher case fatality compared to necrotizing enterocolitis, neonatal jaundice, neonatal sepsis and RDS. None of the admitted neonates were managed with a surfactant.

Mortality rate by neonatal diagnosis combination of study participants in Kayunga, from February 2023 to February 2024.
Discussion
The aim of our study was to determine the prevalence of low birth weight and its associated factors among neonates born at a regional referral hospital in Uganda. This study found a high prevalence of low birth weight (37.4%) among neonates admitted to Kayunga Regional Referral Hospital, which is considerably above the national average of 14%.3,5,12,13 Of these, 46.4% preterm babies were noted as less than 2.0 kgs comprising a high number which necessitated admission for assessment, monitoring and/or management. This high prevalence of LBW is similar with the findings from a study done at a tertiary hospital in Central Uganda that showed LBW rates of up to 25.5% and 24.6% form another study done in Soroti Regional Referral hospital (SRRH).4,14 Similarly in Tanzania, high prevalence of LBW was noted in Muhimbili in 2 different studies, one at 21% and another at 26.4%.15,16 In Ghana, Chiadi et al reported a high prevalence of LBW at 26.5% higher than the global prevalence however lower than that reported in the study. 17 This is similar to estimates by Blencowe et al who reported a high prevalence of preterm births in in sub-Saharan Africa being greater than 15%. 12 However some studies reported lower prevalence rates of LBW. Tessema et al noted a 9.76% prevalence of LBW in SSA way much lower than in the study and rates by Blencowe et al above.6,12 Outside SSA, a 33 years analysis of VLBW in Brazil gave the average prevalence rate at 1.4%. 18 A study by Fortes et al found the prevalence rates of ELBW at 25% in Brazil which actually higher than that from our study. 19 Compared to other settings, these rates are high. This disparity may be attributed to differences in study settings, maternal health-seeking behaviors, and the tertiary referral nature of the hospitals, which likely receive more mothers, referrals as high-risk pregnancies and preterm births. However, the persistently high rates highlight continuing challenges in maternal and newborn health, such as suboptimal antenatal care attendance, infections such as UTIs, malaria, and nutritional deficiencies. A robust healthcare and social system could, not only, potentially aide to curb the rise of preterm delivery but also offer solutions and strategies to adequately identify high risk pregnancies during ANC, management of the preterm, and offer resources to build capacity to manage the LBW neonates and mitigate the environmental challenges to curb pollution and improve air quality.
For maternal factors associated with LBW, only marital status was found to be significantly associated with birth weight classification. Single mothers, as compared to cohabiting and married mothers, were less likely to have a low-birth-weight neonate. The study could not ascertain the possible explanations to this finding due to the limited study numbers and study design. Thus, more research in this specific area is needed.
In regards to factors associated with LBW, gestational age was found to be statistically significant. The observed association between gestational age and LBW is consistent with numerous studies demonstrating that prematurity remains the most important determinant of LBW.4,12,14,16,20 -22 All the low birth weight neonates in this study were preterm according to gestational age. This was estimated using either the LNMP or Ultrasound scan. A modified Ballard was used for estimation of gestational age when the above 2 were not documented. Low gestational age is associated with complications of prematurity like failure to maintain euthermia, apnea of prematurity, RDS, NEC and jaundice.1,12,14,16,20 -22 This predisposes preterm to higher mortality and morbidity.
In contrast, parity, maternal age, multiple pregnancies, ANC attendance and previous obstetric complications were not significantly associated with LBW in this study. This finding differs from earlier studies which noted parity, multiple pregnancies, extremes of age, poor obstetric history, infections during pregnancy and ANC attendance being associated with preterm birth.1,2,4,6,8,12,14,16,21,22 The variation could be attributed to sample size, differences in antenatal care utilization, and regional disparities in maternal health services.
This study noted a very high number of mothers who did not attend ANC however no significant association between ANC and LBW was found. This is similar to a study in Uganda and another in Cameroon which found that ANC visits were not associated with preterm delivery.17,23 Although no significant association was found between ANC attendance and LBW, studies have highlighted the importance of ANC in preventing LBW and its complications.4,12,14,21,22,24,25 A study in western Uganda noted that women who attended ANC more than 3 times less likely to have preterm deliveries as compared to those with less than 3 ANC visits. 22 Similar findings were noted in across SSA and India.2,6,12,17,25,26 Studies have shown the protective nature of ANC attendance maternal health, early detection of pregnancy related complications, risks of preterm delivery, and its associated complications, and overall poor neonatal outcomes.1,2,4,6 -9,12,15,17,21,22,25 -27
Despite the fact that maternal illnesses during pregnancy especially UTI’s, malaria, and HIV were not statistically significantly related to LBW from our study, it is important to highlight that one of the commonest causes of prematurity and intra-uterine growth restriction in Malaria endemic settings like Uganda is malaria, HIV and UTIs.1 -4,6 -9,22 -25,28,29 On HIV, the study had a low prevalence among the mothers with LBW and no association with low birthweight was found, similar to other studies in the region.4,14,22 -25 Similarly with UTIs and malaria, a lower prevalence was noted and no association with LBW was noted similar to other studies.4,17,22,23 This low prevalence could be attributed to the prompt management of the mothers during ANC and availability of programs to prevent and manage malaria, UTIs and HIV in Uganda.3,4,8,14,21,22,24,25
The most encountered diagnoses among the admitted LBW were Respiratory distress syndrome (RDS) 97.1%, neonatal sepsis 63.9%, presumed sepsis 35.6%, Neonatal jaundice 23.9%, Necrotizing enterocolitis 14.6%, Persistent Pulmonary Hypertension 3.4% and Apnea of prematurity 3.4%. LBW neonates have many associated complications due to their prematurity status rendering them not ready for extra uterine life. They are most affected by their inability to manage thermal regulation thus are susceptible to hypothermia, inability to wade off infections (immature immunity), and immature organs to facilitate proper metabolism and homeostasis.1,4,6,8,12,22,24,25,30,31
No LBW was reported to have been managed for hypothermia or birth asphyxia and its cerebral complication of Hypoxic Ischemic Encephalopathy (HIE). However severe studies have documented the association of LBW with HIE.22,31 -35 Strong associations have been reported among LBWs weighing less than 2500g having approximately twice the risk of developing HIE.33 -35 For hypothermia, multiple studies have noted it as a complication associated with prematurity.2,10,12,15,18,21,22,31,32 This is due to the fact that they have limited fat reserves, have slower mechanisms of heat production due to aberrant homeostasis given their immature organs and higher heat loss compared to normal weight neonate.2,4,8,12,22,24,25,31,32
Meanwhile RDS with neonatal sepsis, plus necrotizing enterocolitis and jaundice were the most common combination diagnosis with RDS and sepsis accounting for 63.4% of combined diagnoses with for those affected. This was followed by the co-occurrence or combination of RDS and Neonatal jaundice at 23.4%, and Neonatal jaundice and sepsis at 21.5%.
On multivariate analysis, RDS and apnea of prematurity were found to be significantly associated with LBW in the study. These findings are in line with various studies which show associations of RDS and apnea of prematurity to prematurity.4,6,12,14,15,21,22,25,31 Respiratory distress syndrome and apnea of prematurity are complications associated with prematurity. This is due to the immature development of the lungs and brain which are essential for the initiation, control and maintenance of breathing. Presenting with difficulty breathing, use of accessary muscles for breathing, grunting, gasping and cessation of breathing, RDS and apnea of prematurity can occur independently or concurrently with high rates of mortality.
LBWs with RDS and apnea of prematurity carry a significant risk for mortality compared to those without.1,12,14,22,31,32,36 In our study, LBWs with RDS contributed the highest number of mortality though no significant association with mortality was found. All the deaths reported had more than 1 diagnosis. Combination of more than 1 diagnosis heralds more physiological burden and metabolic demands for the low birth weight with higher mortality. This is similar to findings from other studies.1,12,14,22,25,27,31,32,36,37 The neonates with multiple diagnoses contributed a greater percentage of mortality and the co-occurrence of apnea of prematurity, neonatal sepsis and RDS was a predictor of mortality. The unavailability of surfactant, mechanical ventilation, and poor referral methods of affected LBW using unsuitable mechanisms unsuitable referral methods of affected LBW (during transportation to the hospital) could potentially increase mortality of these neonates.
A high prevalence of neonatal sepsis was reported. This was clinical sepsis as no bacteriological confirmation was done. The study reported a prevalence of 63.9% for neonatal sepsis. This was higher than 35.8%( no bacteriological confirmation) in Kawempe National Referral hospital and 12.8%( with bacteriological confirmation) at Mulago national Referral Hospital.30,38 These wide variations in proportions may be due to differences in geographical areas, protocols and diagnostic criteria used, index of suspicion, and nature or design of study adopted. Preterm neonates tend to have a prolonged hospital stay due to their prematurity status, and as such their care encompasses both management for complications of which infections, and hypothermia are common. Infections in this age group can be acquired vertically from the mother, care givers, and intra-hospital based. Kembabazi et al noted maternal pyrexia, cord care, chorioamnionitis and meconium stained liquor as being associated with sepsis. 30 Late onset sepsis constitutes a high number of neonatal cases.26,30,38,39 High mortality rate is associated with neonatal sepsis in the LBWs.26,30,32,38 -40 Thus a high index of suspicion is required to diagnose, and treat neonatal sepsis and emphasis on seeking care for management of infections during pregnancy, maternal hygiene, and strengthening of the infection, prevention and control practices in health facilities are paramount in reducing neonatal sepsis.
In regards to health outcomes during hospital, 84.8% of the admitted low birth weight neonates were discharged. Mortality was 8.8% which is lower than 35.2% and 31.1% in Kiwoko and Mbarara respectively.22,41 This could be attributed to fewer numbers, and possibly prompt management within the first few hours to 24 hours on admission. The first 24 hours with close monitoring is associated with improved outcomes. Studies show that the first hours are critical for improved outcomes for neonates, especially low birth weight preterm.22,40 -42
The most affected category of low-birth-weight neonates was the VLBW. They were reported to have had poorer outcomes compared to both the LBW and ELBW. VLBW had 3.9% of the total mortality reported as compared to LBW (2.9%) and ELBW (2%). Meanwhile on Case fatality, the VLBW category contributed 44% approximately half of the deaths and they had combination of Apnea of prematurity, RDS and sepsis as the diagnosis. These findings are similar to previous findings across SSA which report mortality being associated to RDS, sepsis, and prematurity.1,2,12,15,24,25,31,32,36
The high burden of LBW in this study underscores the need to emphasize, and reinforce antenatal care programs aiming at early risk detection and prevention of preterm births. Ensuring adequate maternal nutrition, malaria prevention, and family planning services can significantly mitigate LBW risk. Furthermore, establishing functional neonatal intensive care units (NICUs) manned by well-trained, competent and skilled human resource at lower-level health facilities plays a significant role in improving survival outcomes for LBW infants.
The Study Had Some Limitations
This study was limited by its retrospective design, which relied on secondary data from hospital records. Some important variables, such as maternal nutritional status and socioeconomic indicators, were unavailable and no follow up of the LBWs was done. The study also used the documented diagnoses which were made basing on the clinical signs and symptoms with limited laboratory and no instrumental investigations such as routine cranial ultrasound scan, echocardiography, full blood count, CRP, procalcitonin, LDH, blood culture, arterial blood gases, lactic acid, and blood pH potentially leading to an overestimation of prevalence. Secondly the study was conducted at a referral hospital, which may over represent complicated pregnancies and thus overestimate LBW prevalence compared to the general population. Nonetheless, this study has shown that there is a high prevalence of low birth weight in Kayunga with the VLBW having poorer outcomes.
Conclusion
This study revealed a high prevalence of low birth weight among neonates at Kayunga Regional Referral Hospital, with approximately half of them being less than 2.0 kgs and the majority being preterm deliveries. Gestational age, respiratory distress syndrome and apnea of prematurity were key determinants of LBW, while multiple pregnancies, parity and previous obstetric complications showed no significant associations. Mortality was notably higher among very low birth weight (VLBW) and extremely low birth weight (ELBW) and Low ANC attendance was noted overall.
The study findings highlight persistent challenges in maternal and neonatal health, specifically inadequate antenatal care (ANC) utilization, and insufficient neonatal care services and resources and therefore recommends: emphasis, promotion, and strengthening early and regular ANC visits; increasing access to skilled birth services; advocacy for, and establishing and functionalizing neonatal intensive care units (NICUs) with competent, and skilled human resource, drugs, and equipment at all levels of health care; and lastly strengthening infection prevention and control in hospitals.
Footnotes
Acknowledgements
Special thanks go to all the patients, parents, guardians, and KRRH management and staff.
This work was made possible by funding from the Government of Uganda through the Ministry of Health. We appreciate the support from the parents, and guardians of the neonates, the administration of Kayunga RRH, Kayunga RRH staff especially from the department of Pediatrics and child health, the neonatal Unit and Obstetrics and gynecology for their various contributions to this work.
Acronyms
ANC Antenatal Care
ELBW Extremely Low Birth Weight
HIV Human Immune Deficiency Virus
IUGR Intrauterine Growth Restriction
KRRH Kayunga Regional Referral Hospital
LBW Low Birth Weight
MoH Ministry of Health
MUREC Mildmay Uganda Research Ethics Committee
NICU Neonatal Intensive Care Unit
PET Pre-eclamptic Toxemia
REC Research and Ethics Committee
RRH Regional Referral Hospital
SRRH Soroti Regional Referral Hospital
SCU Special Care Unit
UBOS Uganda Bureau of Statistics
UDHS Uganda Demographic Health Survey
UTI Urinary Tract Infection
VLBW Very Low Birth Weight
Ethical Considerations
The study was approved by the Mildmay Uganda Research & Ethics Committee (MUREC) under the number
Consent to Participate
A waiver for informed consent was granted by the MUREC and UNCST due to the retrospective nature of the study, and secondly, prior consent had been obtained from the parents before admission of their neonates to the hospital for management.
Consent for Publication
Kayunga Regional Referral Hospital approved the publication of this manuscript.
Author Contributions
EIEE conceived the study idea. EIEE, SN supervised the study. EIEE, SN designed the database. EIEE, LN, RB, CW collected the data. EIEE, and AO conducted the data analysis. EIEE wrote the first draft of the manuscript. SN, LN, ST, JN, HS, RB, CW, and RS participated in writing the manuscript. EIEE, LN, RS and AO participated in data analysis and visualization. EIEE, SN supervised and were essential in the writing and proofreading of the manuscript. All authors proof read and approved the final manuscript for submission.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study received funding from the Government of Uganda through the Ministry Of Health under its mandate to foster and improve research in its institutions. The funders had no role in the study design, data collection, analysis, decision to publish, or preparation of the manuscript thus the views, and opinions expressed herein do not necessarily reflect those of the Government or the Ministry of Health of Uganda.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.*