
Abstract
The efforts to prevent mother to child transmission of HIV in Malawi are impeded by the loss to follow-up of HIV-exposed infants (HEI) in care. Early infant diagnosis (EID) of HEI and linkage to care reduces morbidity and mortality. There has been limited attention to infants who are lost to follow up despite their mothers being compliant to the PMTCT program. This study explored factors that influence loss-to-follow up among HEI in the EID program whose mothers were retained in care for up to 24 months in Phalombe district, Malawi. We conducted a descriptive phenomenological qualitative study from May 2017 to July 2018. We purposively conducted 18 in-depth interviews among HIV positive mothers whose HEI were enrolled in the follow-up program and 7 key informant interviews among healthcare workers (HCW). All interviews were digitally recorded, transcribed, and translated verbatim. Data were analyzed manually using a thematic step-by-step approach. Results showed that retention in care is facilitated by aspirations to have a healthy infant and linkage to a nearer facility to a mother’s place of residency. The barriers to retention were non-disclosure of HIV status, inadequate resources, and support, suboptimal guidelines for, a lack of privacy, and unsynchronized hospital visits between a mother and her baby. The study has shown that successful implementation of EID services requires concerted efforts from various contextualized stakeholders whilst focusing on family-centered care. To maximize retention in EID and innovative ways of reaching mothers and babies through flexible guidelines are urgently needed.
Background
Despite the implementation of Option B+ since 2011, 1 Human Immunodeficiency Virus (HIV) infection remains a major public health burden in children. There are 4300 new pediatric infections annually in Malawi. 2 The early infant diagnosis (EID) program was established to improve the identification of HIV-exposed infants (HEIs) to accelerate linkage to care 2 which falls within the fourth prong of the Prevention of Mother to Child Transmission (PMTCT) guidelines. 3 Early infant diagnosis for HIV-exposed infants is a series of events starting from birth to 24 months of age. 4 It has a testing protocol that involves collecting blood samples of HIV-exposed infants for HIV testing at 6 weeks, 12 and 24 months of age. 3 The prophylaxis drug of choice within the EID program is nevirapine (NVP) which an infant receives from birth until 6 weeks followed by cotrimoxazole from 6 weeks and taken up to 24 months. 4 Both the infant and the mother have monthly scheduled visits during the first 6 months of a child’s life. For the remaining period of up to 24 months, visits are scheduled every 3 months. During these visits, a mother refills her ARVs, she is counseled on adherence. Her viral load is monitored and is given isoniazid preventive therapy (IPT). Mothers further receive cotrimoxazole prophylaxis, routine Tuberculosis screening, and services are in some settings integrated with non-communicable diseases and family planning services. 3 Beyond the normal under-five services, HIV-exposed children also receive cotrimoxazole for prophylaxis, and once HIV infected they are initiated on antiretroviral therapy (ARVs). 5
Evidence shows that early infant identification and linkage to care reduces morbidity and mortality associated with HIV infection. 3 Malawi has made positive strides in the implementation of the EID program including; mother-infant pair follow up clinics up 24 months, improvement in sample transportation, and use of point of care (POCs) in a few facilities. The use of POCs has resulted in a reduced turn-around time of the DNA PCR results from 60 days to as low as 1 day in facilities with POCs. 4 Furthermore, improvements have been registered in screening for HIV amongst children under the age of 5 years in various pediatric settings. 4 However, loss to follow up from the EID program remains a major challenge that threatens the progress gained to date and derails progress toward achieving the goals of the program. A client is deemed lost to follow up when a client does not return to the clinic 2 months after running out of ARVs. 5 As of 2016, the proportion of HIV positive mothers on Option B+ that were lost to follow up (LTFUP) at 24 months for Phalombe district was at 30% while among HIV-exposed infants it was 39% to 46%.5,6 Similarly, in the south-eastern zone where the study was conducted, the rate of LTFUP for exposed infants has on average been at 37% while it was 51% in the specific district where the study was conducted.5,6 It has been noted that while mothers continue with care, most infants do not report in subsequent visits. The reasons for the discrepancy between mothers and infants in the continuity of care remains unclear. A loss to follow up alongside with poor feeding practices contribute to Mother to Child Transmission (MTCT) of HIV in Malawi. 7
Most studies conducted on loss to follow up in the PMTCT program have focused on loss to follow up of PMTCT mothers from antenatal to postnatal periods with limited attention on infants who are lost to follow up despite their mothers being compliant to the PMTCT program.8-12 Given the relevance of adhering to EID of HIV services and as a measure of closing the gap in identifying HIV infected infants, this study explored factors influencing loss-to-follow up among HIV-exposed infants in the EID program in Phalombe district, Malawi. The study focused on infants whose mothers were retained in care for up to 24 months without their children despite that their children were still living. Exploration of these factors would shed some light on how to optimize uptake and retention in EID services.
Conceptual Framework
The study was guided by the Health Belief Model (HBM) which is a psychological model that explains and predicts health behaviors. It has 3 principal concepts which include: individual perceptions, modifying factors, and variables affecting the likelihood of initiating actions. 13 The model explained and predicted the health behavior of the mothers of HIV-exposed infants on their attitudes and beliefs toward follow-up and related a socio-psychological theory of decision making to individual health behavior. 13 It can predicted that the perceived susceptibility of mothers transmitting HIV to their infants would be a motivating factor for a mother to continue with follow-up visits in the EID program. Perceived severity in this study encompassed consequences of non-compliance to follow up schedules including a late diagnosis in the baby, with the potential of compromising an infant’s immunity consequently affecting the infant’s response to treatment thus yielding poor treatment outcomes. We conceptualized perceived benefits of follow up visits as receiving recommended prophylaxis thus reducing morbidity rates in HIV-exposed infants, overall infant monitoring at every visit including early uptake of an HIV test to trigger initiation of ART immediately. We also assessed perceived barriers that may affect follow-up visits. In this study, cues to action were interpreted as any factor that motivated PMTCT mothers to remain in the EID of HIV program including mother’s knowledge on PMTCT, previous experience, support from husband, and family members. We interpreted self-efficacy as PMTCT mother’s courage and willingness to take action like bringing the infant to all recommended follow-up visits. 13
Methods
Study Design
A descriptive qualitative study was conducted and it followed a phenomenological approach in Phalombe district, Malawi from May 2017 to July 2018 to investigate factors that were associated with loss to follow-up of HIV-exposed infants in the EID services within the PMTCT program. In-depth interviews among mothers of HIV-exposed infants and key informants among health care workers. Interviews allowed investigation of social issues by assessing people’s experiences, behaviors, perceptions, feelings, and opinions about the phenomenon.14,15 This approach provided room for the participants to express themselves freely and also gave in-depth information. 15
Study Setting
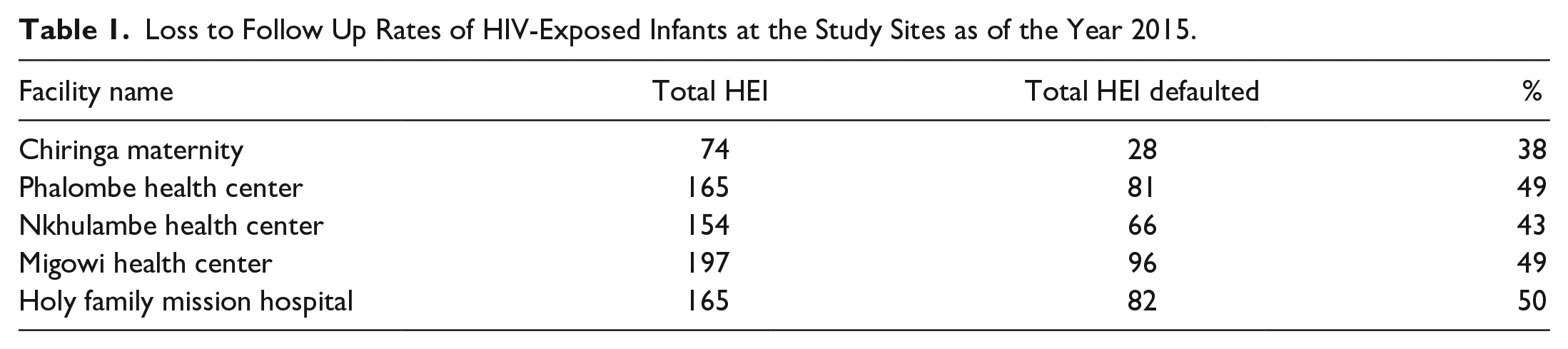
The study was conducted in Phalombe district which is in southern Malawi. In 2017, Phalombe district registered a total number of 1721 HIV-exposed infants of which 666 (38%) were reported as lost to follow up. Five health facilities indicated in Table 1, with high default rates of HIV-exposed infants were purposively selected in this study and these are Chiringa Maternity, Phalombe, Nkhulambe, Migowi, and Holy Family Mission Hospital. 16
Loss to Follow Up Rates of HIV-Exposed Infants at the Study Sites as of the Year 2015.
Sampling and Sample size
Twenty-five participants were selected 18 and of these were HIV infected women from 5 selected facilities and 7 were health care workers who run HIV-exposed infant clinics in the 5 selected facilities. Extreme deviant case sampling was employed in the selection of HIV infected mothers. We included 10 HIV positive mothers who were retained in PMTCT care whose HIV-exposed infants were lost to follow up; 4 HIV positive mothers who were compliant to PMTCT follow up clinics with their children; 4 HIV positive mothers who were lost to follow up with their infants. Such a selection guaranteed a sample rich in the information to achieve depth in the subject sampling. 16 We sampled 7 health care workers working in PMTCT/ART clinics. Mason 17 contend that 15 is the smallest acceptable sample size for qualitative research. However, the study interviewed 25 participants and at this point, saturation was reached when no new information was generated from the participants.17,18
Recruitment of Study Participants
Enrollment of HIV infected mothers
Permission was sought from the Director of Health and Social Services (DHSS) and the respective facility in-charges of each center before recruiting participants. The ART teams were briefed and introduced to the aim and objectives of the study. With assistance from the ART clinic health workers, the cards of HIV-exposed infants lost to follow up in the PMTCT program, and the mothers’ ART cards were identified from which the date of the next appointment was noted. Meetings were scheduled on the day of their next appointments especially for mothers who were retained in care. The mothers who were not retained in care were followed them in their respective homes with the help of expert clients. Expert clients were HIV infected volunteers who were responsible for tracing clients who missed their appointments in the program. 3 None of the 18 HIV infected mothers refused participation in the study.
Mothers with infants lost to follow were approached as they reported to the clinic and were screened for recruitment. We verified that the infant was lost to follow up through checking records of exposed infants in under 24 months cards that have ART numbers that link an infant to a mother. Recruitment of study participants was varied by considering the following: proximity to the health facility, number of living children, marital status, and employment. 19 We sampled from the 2014 cohort because by 2016, at the time the study was conducted, this group was finishing their 24 months EID follow-up period 19 which allowed for a comprehensive assessment of their child’s status. In general, there was inclusion of women who were: 18 years of age and above and were willing to participate in the study; HIV infected mothers who consistently reported alone to the facility whose HIV-exposed infant was lost to follow up; HIV infected mothers who inconsistently reported to the facility whose HIV-exposed infant was lost to follow and HIV infected mothers who consistently reported to the facility with an exposed infant.
Enrollment of health workers
Health workers from the ART/PMTCT clinics were identified with assistance from the facility in-charge and were briefed on the study. Enrollment included (a total of 7) EID focal persons from the 5 facilities including; clinician, nurse, HIV Testing Services (HTS) counselor, or ART clerk. The participants were approached at their facility and all of them were enrolled in the study.
Data collection
Data was collected using a semi-structured interview guide from the mothers. The guide was designed based on the specific objectives of the study. It was also guided by the conceptual framework (Health Belief Model) and literature. It was piloted at Phalombe health facility. The semi-structured interview guide were administered by the corresponding author. All sessions were recorded using a digital recorder and lasted for 26 minutes on average and were conducted at the health facility or the community as per participant’s preference. The interview guide was reviewed by ALNM and tested to ascertain its adequacy. 20 We ensured the credibility of the findings through member checking which was done by summarizing key points at the end of the interview. 14 The audio recordings in Chichewa were transcribed verbatim to English to avoid loss of information. A unique identification number was assigned to each recorded interview. The security of the recordings was ensured by using password protection only accessible to authorized users.
Ethical considerations
Issues of confidentiality, privacy, and autonomy of choice were addressed in the study. Before we could approach participants authorization was sought from authorities such as DHSS and health facility administrators. We informed participants on the purpose of the study, its significance, benefits, and risks before conducting an interview or administering questions. Participants who agreed to the study provided a written or thumb-printed informed consent and were free to stop the interview or filling the questionnaire at any point during the study. They were informed that their refusal to participate or withdrawal from the study will not affect their access to health services at the clinic. No incentives were given to participants. Codes to identify participants were used to conceal their names for confidentiality. Interviews were conducted in a private room to achieve privacy. All study documents and recordings were stored securely in lockable cabinets and password protected on a computer and only accessible to researchers involved in this study. The study was reviewed and duly approved the institutional review board College of Medicine Research Ethics Committee (COMREC P.10/17/2293).
Data analysis
Data was analyzed manually following a thematic approach as suggested by Braun and Clarke. 21 Audio data were transcribed and translated verbatim from Chichewa into English. The transcripts were read multiple times for data immersion and familiarization, and also to get meaningful segments and essence. During this process, notes and markings were made within the transcript for coding. 21 Two other independent authors proofread and coded the transcript. The different codes were discussed and agreed to establish a coding framework. The generated themes were reviewed iteratively, to assess if they were relevant to be theme or sub-themes and this determination was based on the richness of the codes under the theme. Themes that did not have enough supporting data were separated and combined with other themes to form 1 theme. 21
Results
Demographic Characteristics of Health Care Workers
Among the 7 health workers that were interviewed, 5 were males and 4 were nurses by profession, a clinical officer, an ART clerk, and a PMTCT focal person. All the participants were trained in PMTCT and demonstrated knowledge on the algorithm for the EID test and FUP schedule. All the participants had been working in the ART Clinic for more than 2 years.
Demographic Characteristics of Study Participants (HIV Infected Mothers)
Among the 18 PMTCT mothers interviewed, 4 had defaulted from the PMTCT program together with their HEI and 4 PMTCT mothers together with their HEI were compliant on the PMTCT program. The other 10 PMTCT mothers had their HEI lost to follow up while the mothers were active in PMTCT services. The age range of the participants was from 18 to 46 years with a median of 26 years. A total of 11 participants were married, 6 were divorced and 1 never married. Fifteen participants had a primary level of education while 3 reached the secondary level. Fourteen participants were not employed while 4 ran small-scale business. Fifteen participants were on ART and 13 had disclosed their status to husband, family members, and friends. Fifteen participants had 2 children and above and the average number of children was 3 children.
Motivating Factors to Retention in EID Services
HIV positive mothers who were retained in care together with their infants were motivated because they desired to have a healthy child and they attributed this motivation to the knowledge which they have on the importance of EID/PMTCT services (Table 2).
“Aspiring to have a Healthy child”
Factors that Influence Retention in EID Services.

The primary motivator to continue with EID follow-up among mothers of was to have a child-free of HIV infection. Mothers stated that their responsibility was to prevent the transmission of the virus to their babies.
“The importance is that the child will be born negative . . . he will also pass two years while still negative, so if he contracts the virus it should be by himself . . . but at least I have helped him.” PMTCT mother in care with HEI – LTFUP #11
The knowledge women had on the benefits realized after compliance to EID program strengthened a woman’s quest to have a healthy baby. They embraced the role of protecting their child with the information and continued participation in the services.
“My problem should not affect the child . . . What I mean is, if I neglected following the doctor’s advice, the child would be infected from breast milk.” PMTCT mother compliant #3
Although mothers of HIV-exposed infants that were lost-to-follow-up reiterated on the importance of complying to EID schedules they did not practice that fully.
With the way I am (HIV positive), I need to make sure that the child does not become positive . . . Both PMTCT Mother and Baby non – compliant #2
Follow Up and Linkage to Nearer Health Services
Ensuring that mothers and their children are linked to the nearest facility to their place of residency motivated them to remain in care. Distance is a notable challenge that makes compliance difficult to achieve. Health care workers assess the distance a mother has to cover and advise her to access EID follow up visits at the facility that is closest, to her to curb defaulting or interruptions in care.
“. . . for the mother who complains of long-distance, we explain to them the advantage of receiving drugs from a nearby hospital, so we tell them to make sure they are nearby a hospital if they think this one is too far from their residence by requesting for a transfer letter, they should go to a nearby hospital so that they do stop follow-up due to long walking distance to the facility with the baby.” Migowi_Health Centre_H/W #4.
Role of Expert Clients
The availability and inclusion of expert clients in service provision motivates retention in services. Expert clients are lay people who are HIV infected and have publicly disclosed their status and share characteristics of the other parties. They serve as role models that support others in their context and usually are resident in the same areas as the participants. In facilities where they are present, they conduct follow-up activities to the clients to encourage them on retention in care and offer other psychosocial support that a client may need.
“Together with the Expert Clients we go through our records and also the patient cards showing them which patients haven’t come to the clinic and they take the necessary addresses so that they should follow that patient who hasn’t come here.” Phalombe_ Health Centre H/W #1.
Expert clients counsel women is drawn from their lived experiences and encourage them to remain in care even in cases where the distance covered is quite long.
“In collaboration with expert clients who have the technical know-how on follow up of clients. They help with this issue to encourage them that despite coming from far they should try to always take their medication. They tell them the goodness of taking drugs and to come to the clinic on the date given, yes! that they should try at all costs, they should not be absent.” Holy family mission hospital_H/W #5.
Barriers to Retention in EID Services
The barriers are presented across different levels of individual, family, and health systems. Although they have been categorized as such for presentation purposes, they are interrelated and should be viewed as such (Table 2).
Individual Level Barriers to Retention in EID of HIV Services
Reluctance to continue with the services
Both health workers and mothers of HEI reported that some women are reluctant to return for follow up visits because they would conclude the status of their child as infected as well. A lack of optimal knowledge on the transmission paths of HIV from a mother to her child perpetuates this practice.
“The reason would be, let me say reluctance since I was sick (HIV positive). So I just felt my child will be sick too.” Both PMTCT Mother and Baby non - compliant #1
Reluctance to attend the services could also be influenced by a child’s HIV test results especially in instances where a child has tested HIV negative at both 2 and 12 months of age, a mother would conclude that her child is negative and may not need the services.
“Maybe I would say faith right, thinking their child is fine. They think the results would not change . . . if they are negative they will continue being. . . negative.” Holy family mission hospital H/W #5.
Ongoing denial of a mother’s HIV-infected status results in her abandoning the program if she initiated or may not even initiate into it.
“Some women fail to accept that their child could be in this programme because the programme is too much involving, they give us drugs to be taken every night.” PMTCT mother compliant #1.
Reluctance to be in the service may further push a mother to provide incorrect residential addresses so that any means of reaching her should remain futile. This creates a challenge that is compounded with low cellphone ownership in rural areas.
“At times they register under a group village and when you ask in the village for the group village, its difficult to find the specific village it becomes a problem too, as a result, you walk the whole day searching for them.” Migowi_health Centre_H/W #4.
Lack of disclosure of an HIV-infected status
Health workers reported that some mothers of HEI opt for non-disclosure of their HIV positive status to their relatives. As a result, they register fake names at the hospital to avoid being followed up. The resultant effect of non-disclosure is a gap in follow up activities even when expert clients want to trace them.
Specifically for married people, lack of disclosure was common among women who remarried because they feared losing the new husband which contributes to a baby missing EID services.
Non-disclosure of an HIV status is perpetuated by fear of adverse consequences following disclosure thus women feared intimate partner violence if they ever disclosed their status or are found taking ARVs. The need to conceal their HIV status coupled with a failure to covertly take their ARVs and administer the same to her child results in non-compliance with services “People talk a lot at home . . . so if they knew then everyone will know and when they know the will be shouting at me, so I saw it wise not to tell anyone.” Both PMTCT Mother and Baby defaulted (non - compliant) #1.
One woman shared her experience when she was abandoned by her boyfriend following disclosure of her HIV infected status. Women prefer preserving their marriage even when it costs their compliance with PMTCT/EID services.
“I was abandoned by my boyfriend when he realized that I’m HIV positive.” Both PMTCT Mother and Baby defaulted (non - compliant) #1.
Fear of side effects from the drugs
A mother’s experience of the side-effects coupled with sub-optimal information on ARVs made them deduce that their baby will also experience the same worse-off side-effects which made them not to enroll a child in that service.
Lack of financial resources
Health workers who operate Mother-Infant-Pair clinics said that mothers of HEI prefer to leave the child at home when coming for PMTCT follow up clinic because they sometimes don’t have money to buy food for the child while at the hospital. The lack of finances becomes pronounced when there is a long waiting time at the clinic which could be influenced by health system factors.
“Any delay in starting the clinic makes the children stay longer in the queue and they feel hungry, and as a parent, if I don’t have money to buy food for the child during clinic days it becomes hard to attend the clinics . . . I sometimes just think of not going for follow up visits.” PMTCT mother in care with HEI - LTFUP #7
Family Level Barriers to EID
Lack of support from family members
Mothers with no or minimal support from their family members found it challenging to cope with an HIV-infected child and continue with services. This was apparent in single mothers or those with more children to care for by themselves.
PMTCT mothers reported that they feared being discriminated by the relatives for being HIV positive, as such, they would not do anything that may expose their status to their relations. Some activities that a mother would abandon would be the attendance of EID services as that would indirectly expose of her status.
Lack of child spacing
Other participants reported that they became pregnant before their baby was 24 months of age which imposed a challenge for them to continue with EID services. They further reported that at that point the health system requires that they access their ARVs at the antenatal clinics and not at the MIP clinics which made them leave the other child home so that they proceed with ANC services alone. The connotation of ANC as a space for pregnant women with services for pregnant women creates a structural problem for such women. In some instances, a pregnant woman experiencing some minor discomforts of pregnancy would opt to leave the child at home to ease off her discomfort.
“That time I was pregnant, so when I carry him on my back, my leg was hurting, so I thought I should be leaving the child home now.” PMTCT mother in care with HEI - LTFUP (non - compliant) #11.
Customary practices of transferring the care of a child to a grandparent when a mother is pregnant before the other child is older contributes to non-compliance on the child’s part. In this case, the mother may continue her visits to the PMTCT/EID program while the child will not since the child is under another person’s care who may not be aware of the need of EID services.
Lack of male involvement
Non-involvement of a male partner in the services or care of children at home contributes to mothers leaving their children home. All the participants expressed that very few men are involved in the care of HIV-exposed children. The traditional norms that have relegated child welfare issues to a woman propel the non-involvement of men.
“There was nothing he assisted me with . . . because when I tell him about this, maybe he is afraid of this place, he does not want to come.” Both PMTCT Mother and Baby defaulted (non - compliant) #1.
In other instances, a husband is not involved because a wife has not disclosed her HIV infected status especially in interrupted marriage.
“My husband has never taken any part because I hide it from him . . . Yes, because we got separated, so when I was starting taking drugs, he was not there.” Both PMTCT Mother and Baby defaulted (non - compliant) #3.
Besides, some PMTCT mothers mentioned that they failed to come to the hospital because their husbands restricted them from coming to the facility. After all, it may also disclose their status to others.
Other participants mentioned that they were threatened that they would be beaten or face a marriage dissolution if they go to the hospital to collect their ARVs.
“My husband said that I should not go to collect [the drugs] or else he will beat me or that will be the end of our marriage.” Both PMTCT Mother and Baby defaulted (non - compliant) #2.
Health System Barriers to EID Services
Service delivery factors
Lack of consideration of clients with other needs
Phalombe borders with Mozambique such that the absence of clear guidelines in the management of clients from Mozambique leads to non-retention in EID services. Health workers reported that some PMTCT mothers are from Mozambique, so they find it difficult to follow them up because it’s very far and across a national border. These clients intentionally provide a Malawian address to ensure they receive care at the point of enrollment only to realize later that they were from Mozambique.
“I believe that people from Mozambique think that if they tell us that they’re from Mozambique, we will not assist them, so they lie about the villages. They tell us names of the villages from Malawi bordering their country.” Nkhulambe_health Centre H/W #7.
Another category of clients requiring special consideration are those with underlying medical conditions. A medical intervention that a mother and baby may be going through may prohibit a baby’s attendance to EID. One participant cited that compliance to Kangaroo Mother Care (KMC) intervention obstructed her from bringing her baby to the clinic.
“I never brought my child to the hospital because I was under home-based Kangaroo Mother Care (KMC) . . . The baby was born prematurely so they released me earlier and told me that I am not supposed to be walking around with the child, but should be staying at home.” PMTCT mother in care with HEI – LTFUP (non - compliant) #5.
The practice of guardians collecting drugs for PMTCT mothers
Health workers reported that by allowing guardians in the health system to collect ARVs for PMTCT mothers, it inadvertently leads to children defaulting because the guardian tends to come alone without the baby. Administration of pediatric ARVs requires that a baby is weighed at every refill encounter because the dosage is based on weight.
“When guardians are sent without a child, they are not allowed to collect the drugs for the child because the child’s drugs are dependent on the current weight of the baby . . . If this continues, the child’s card indicates defaulted.” Chiringa Maternity H/W #6.
A protocol of unofficial or short-term transfers
Management of transfers that have been initiated by clients without supporting documents from the transferring facility results in mothers failing to access ARVs at the new facility and for their child to continue with EID services. The reasons for initiating a self-transfer varied and included attendance at funerals and other family matters.
“I left here and went to another place for a funeral so I was not expecting that I would spend maybe two months, but it happened that I spent two months without going to the hospital to get drugs. There was no place for me to get the drugs, so I stopped taking the drugs.” PMTCT mother in care with HEI - LTFUP (non - compliant) #5.
Some situations required that a child be separated from their parents hence moving away from their facility of care unofficially resulting into defaulting from the EID program.
Unsynchronized hospital appointments of mothers and babies
Health workers indicated that assignment of different appointment dates was another reason that contributed to the loss to follow up of HIV-exposed infants.
“If health care providers haven’t set the same dates, to say maybe the mother was supposed to come maybe on the 2nd of February and we give the baby 8th February, it happens that the mother will just come on her own to get the drugs on the date set for her and when the date for the baby arrives you find that she hasn’t come to get drugs for the baby, in the end, the mother will be the only one taking drugs.” Phalombe_health Centre H/W #2.
Lack of privacy at the MIP clinics
It was reiterated that mothers of HEI complained about a lack of privacy at the MIP clinic compared to the general ART clinic. Mother-Infant Pair (MIP) clinic entails the integration of services such as antenatal clinic and as a result, it falls short on the privacy spectrum which causes women to opt for general ART for themselves which automatically neglects the child.
“There is a lack of privacy on the MIP clinic day compared to general ART clinic day because these two clinics are run in two different setups. So some women prefer to come alone on a general ART clinic which is offered in a more private place.” Chiringa Maternity_H/W #6.
Supplies and resources
Transport challenges
Health workers reported that there are limited bicycles which Expert Clients use to conduct follow-up visits for those who miss the appointment which prevents optimal tracing. Lack of optimal tracing results in non-compliance among HEI.
“Transportation is a challenge since others do not have bicycles, so we are very grateful to DREAM because DREAM provided bicycles on what we call pool. This is where anyone who would like to use this bicycle can get it and use it. If it has a breakdown since it does not have ownership . . . they walk for a long distance.” Chiringa Maternity_H/W #3.
Transportation and long distances were not only limited to health workers as mothers reiterated the same. Long distances to the health facility was a contributing factor to LTFUP of HEI in the PMTCT program. Most parents fail to bring their children to the hospital considering the long distance that they travel to come to the hospital with the child at their back.
“The only problem I see is carrying the child on my back, bring him here, then taking him back home.” PMTCT mother compliant #2.
Timeliness of services
The participants stated that the clinics open late for services, leading to longer waiting times and their children become hungry while waiting to be assisted.
“They start running the clinic late at around nine AM. So for a child to be here until this time, it becomes difficult . . . you find the child has not eaten anything since morning till now, so the child is irritated and tends to be a nuisance . . . and maybe at this time, it’s when they are starting with service delivery. . . and one maybe going home around 3 PM while has not eaten anything.” PMTCT mother compliant #1.
A resultant effect from longer waiting times is that children become tired and tend to cry more which was said to cause some health care workers to suspend dispensation of ARVs if a mother is failing to soothe her baby. This practice by health workers discourage mothers from attending EID services with their children.
“We come in the morning, maybe you haven’t eaten, the child hasn’t eaten anything . . . so when giving out drugs they may start late, so sometimes it happens that the child is crying . . . in the end they (health workers) may be angry and shout at us. They may be pissed off and stop dispensing the drugs.” PMTCT mother in care with HEI - LTFUP (non - compliant) #7.
However, the health workers stated that the delay in initiating services was mainly due to morning handovers among health care workers and nutritional assessment before starting the clinic and shortage of staff.
“They say we start work very late, so here we first thing is we go for morning handover report. When we come back from there around past 8 or to 9 we start looking for the cards to give them and then we start doing a nutritional assessment. So they think we are delaying them and they feel that their children stay hungry and start crying so this indeed contributes to some mothers just coming to get their drugs alone.” Phalombe_health Centre H/W #1.
Discussion
The study revealed that factors that motivate retention in EID of HIV services include aspiring for a healthy child, ability to be linked to a nearer facility to a mother’s place of residence, and involvement of expert clients that follow-up and motivate mothers to remain in the program. The barriers to retention in EID were classified at individual, family, and health system levels. At the individual level, a mother’s reluctance to be enrolled in the program, a lack of disclosure of a mother’s HIV Infected status, fear of side effects from ARV, and inadequate financial resources impede retention or initiation of EID services. Lack of various support systems from family members, male partners influences non-retention in EID services and a lack of child spacing in a family prevents retention. Delivery of services such as suboptimal guidelines in the management of mothers that are coming from other countries, the practice of allowing guardians to pick drugs on behalf of the mother, unsynchronized hospital appointments between a mother and child, and lack of privacy within the health system influences non-retention. Lack of supplies like transportation mediums for conducting follow up of clients and non-timeliness of the services evidenced by long queues and late opening times for the clinics affect retention on EID services. Our findings should be interpreted in the context of the health belief model.
Motivating Factors to EID Follow Up Schedule
Our finding that a quest for a healthy child motivates a mother to retain in EID of HIV services is similar to earlier studies that reported of women being motivated and encouraged to engage in EID services because of the benefits realized.22-24 Furthermore, Mpinganjira et al 25 reported that perceived good health after taking ART was another motivating factor for continuing with follow up. This resonates with the tenet of perceived susceptibility under the HBM which we contextualized as the likelihood of a mother transmitting HIV to her infant and this was a motivating factor for a mother to protect the child hence continued with the follow-up visits in EID. 13
Limited understanding of PMTCT and EID services as observed in the study mirror results in previous studies.24-26 In Malawi, women harbored a poor understanding of the indication and purpose of ART consequently resulting in women whose children tested HIV negative at 9 to 12 months disengaging from PMTCT and EID services despite receipt of prior counseling about the risk of infection during breast feeding. 25 Similarly in Kenya, children that were perceived to be healthy coupled with a negative HIV test were less likely to be linked to HIV care because their caretakers had concluded that the children were negative and only brought them to the clinic when they developed an acute illness. 26 It has been argued that healthier babies become lost to follow up with successive HIV negative results. 25 This finding resonates well with the Health Belief Model that contends that one’s perception of susceptibility to a certain threat determines their response and also that if the threat is minimal, one may relax in their response like it was observed in the study. 13 It is important that the messaging to mothers of children who test HIV negative whilst still on the program emphasize on the possibility of a child contracting HIV if the exposure remains. 27 Promoting the knowledge that women have on PMTCT and EID services has the potential of increasing retention in the services. 27
Although the study did not investigate the existence of associations, the study showed that most mothers in the PMTCT program had little formal education in a district literacy of 69.4% which is slightly lower than the national average at 72.1% (MDHS, 2015-16). 28 An earlier systematic review 27 reported an association between lower maternal educational level and not receiving/taking ARV prophylaxis. 27 This also influences poor knowledge of HIV transmission and the relevance of ARV resulting in dropping from PMTCT/EID programs.26,29 Arguably, maternal education is a factor that cannot be ignored in the conduct of EID services and is founded on the Health Belief Model that asserts that a person’s education level is one of the external stimuli within the cues of action that is needed to trigger one’s decision making process. 13
A good follow up mechanisms for tracing those lost to care as suggested for in this study is comparable to those reported in studies conducted in Malawi and Zimbabwe.8,27,30 Some of the follow-up strategies include the use of mobile phones8,30 that was not recommended in the study because it was conducted in a rural setting where few women own mobile phones. The study recommends the use of expert clients who are available in most communities and could support tracing and encourage mothers to be retained in care. 23 The key to this type of support is contextualizing the approaches for instance organizations like Mothers to Mothers (M2M) could be encouraged to continue with services that ensure peer support among HIV infected mothers. 31 Mothers to Mothers is an international organization working toward ending Acquired Immunodeficiency Syndrome (AIDS) and creating bright futures for women and families across sub-Saharan Africa, among other things it employs women living with HIV as Community Health Workers called Mentor Mothers, these women help in doing follow-up of a patient on ART who are lost to follow-up. 31
Linkage to a nearer health services was reported in this study as a main facilitating factor in retaining the infants that were lost to follow up. This agrees with the results of a systematic review where patient convenience and accessibility was one of the factors that help retain patients in care. 32 Related to linkage to care is drafting and implementation of guidelines that serve clients that are from neighboring countries.
Despite good follow up mechanisms, follow up of cross-boarder clients in Mozambique due to the long-distance and provision of wrong addresses by some clients was a challenge that needs collaborative effort with the Mozambican government.
Barriers to Continuing with EID Follow Up Program
Becoming pregnant before their child was 24 months of age was a unique barrier to have HEIs returned in care whilst the HIV positive women remained in care. The burden created by the long distances resulting in a reluctance to continue with EID services is similar to an earlier Malawian study that reported that mothers of HEI found carrying their children to the clinics exhausting. 25 The minimal perception of risk of MTCT coupled with the long distance is explained within the HBM that a mother may not follow through with the expected visits. 13
Disclosure of an HIV infected status remains a critical barrier to accessing HIV services. Non-disclosure was favored and used as a way of averting intimate partner violence and dissolution of a marriage resulted in non-retention in PMTCT and EID services. This finding adds to the literature that has shown repeatedly that if mothers anticipate a negative reaction from their partner or family, they would not disclose their HIV-infected status thereby failing to continue with PMTCT/EID service.21,33 Non-disclosure led mothers to register with fake names or addresses so that any form of tracing should be futile. This finding is similar to a study conducted by Cataldo et al 34 which found that women that were lost to follow up would give a range of reasons for not coming back to health facilities and often implicitly chose against being traced by providing a false address at enrollment.
Lack of disclosure is intricately related to lack of male involvement and the latter has been associated with reduced odds of early infant HIV testing.27,35,36 Our results on lack of male involvement and family support remain consistent with many Sub-Saharan African studies, which have highlighted these as ongoing factors that continue to plague PMTCT programs and was categorized as a major barrier to uptake of PMTCT interventions.23,24,27,29 Consequently, it has been argued that addressing domestic relationship dynamics, including emotional violence and encouraging HIV status disclosure to the male partner and other family members, may play an important role in maternal uptake of early infant HIV testing.27,37 Nonetheless, male involvement in PMTCT increases the uptake of services by HIV positive women 4 and creates a motivating atmosphere for a mother to continue with the services.27,37 The support from male partners adds to the social and family support that also encourages participation in PMTCT services.29,38 Leveraging of existing community groups to support mothers in their circle may promote compliance for both mother and infant with a potential of diffusing stigma. 39
Our findings showed that remarried mothers who did not disclosed their HIV infected status to their new partner experienced challenges in accessing PMTCT services without their new partner noticing it. This underscores the relevance of couple counseling and testing before marriage. 40 The fear of stigma and status disclosure to partners and family members remains the most frequently cited barrier to uptake of PMTCT.8,32,37 Furthermore, unplanned pregnancy is common among HIV infected women and strengthening of integration of family planning within all HIV services will avert this which may prevent loss to follow up secondary to repeat pregnancies as was expressed in the study. Provision of quality reproductive messages is essential for women to make informed decisions on family planning. 41
Mothers of HEI feared that their children will suffer worse-off side effects from ARVs. This is consistent with findings of other studies that reported that beliefs that ARVs could harm the child were a threat to mothers starting ART26,29 and this belief has in some cases resulted in mothers disengaging from HIV care.13,27 A poor socioeconomic status limits what a mother can provide to her child whilst at the facility especially when she experiences long waiting times. Similarly, socioeconomic status determines access to EID services and leads to LTFUP in previous studies33,35 as it also affected a mothers’ means of transportation to the facility. 24
Uniquely, the study has shown that allowing guardians in the health system to collect ARVs for PMTCT mothers, inadvertently led to children defaulting because the guardian tends to come alone without the baby. The solution to this barrier would be intensifying health education and initiation of village clinics to bring services closer to the actual clients. Our findings on a negative attitude of health care workers are similar to findings from the study in the Ivory Coast which revealed that mothers were afraid of being scolded at by health workers.23,27,37 As also reported in the study, a long-distance between one’s home and the health facility contributed to the loss to follow up for EID service which is further worsened with mothers’ inability to afford transport costs due to long distances to travel to the hospital.4,8,27,29,30 The solution to this burden would be incorporating EID services in village health clinics that are in most villages and provide integrated child health services. 42
Participants complained that clinics open very late which contributed to staying longer at the hospital.30,37 Our findings remain congruent with reports from studies conducted in Uganda and Kenya which revealed that staff shortage was among the reasons leading to the loss of mother-child pairs in the EID program because it resulted in long waiting periods, compromised privacy resulting in some women leaving without being assisted.9,43 An increased workload leading to burn-out yields a poor attitude from health care workers 43 which was also observed in the study. Arguably, the loss to follow up of infant-caretaker pairs may be minimized by addressing major bottlenecks such as shortages of EID/PMTCT staff, lack of staff motivation, lack of skills, and training of staff in effective PMTCT implementation. 35
Lack of privacy which leads to loss to follow up as expressed in the study concurs with results form a Mozambican study that registered 75% loss to follow up secondary to lack of confidential counseling in overcrowded postnatal wards. 44 Absence of privacy creates an uncomfortable environment thus lessening the chances of women returning to the hospital for the baby’s EID. Additionally, fragmentation in the provision of EID services that occurred secondary to services being provided in different buildings from the one where a woman would initially seek care from led to some women failing to navigate the pathways for them to access the needed services possibly resulting in some women getting lost between referral and follow-up. 44 Unsynchronized appointments between a mother and her baby as reported in the study may be solved by integrating ARV services in all maternal, newborn, and child health programs which were effective.
Strengths and Limitations
The perceptions and experiences of those who chose to participate may be different from those that never participated in the study however, we believe that our sampling criteria offer more breadth to the applicable variables. The results provide insights that are useful locally with the potential of validating them in other contexts.
Conclusion
The overall findings in this study showed that the main reasons for loss to follow-up of HIV-exposed Infants in EID program were geographical barriers, functional inaccessibility of the services, socio-economic barriers, individual barriers, perceived fear, follow up mechanisms, and poor support systems. Successful implementation of EID services will require concerted efforts from various stakeholders that are contextualized whilst maintaining a focus on family-centered care. To maximize retention in EID, innovative ways of reaching mothers and babies through flexible guidelines are urgently needed.
Supplemental Material
sj-pdf-1-gph-10.1177_2333794X211004166 – Supplemental material for Factors Influencing Loss to Follow-up among Human Immunodeficiency Virus Exposed Infants in the Early Infant Diagnosis Program in Phalombe, Malawi
Supplemental material, sj-pdf-1-gph-10.1177_2333794X211004166 for Factors Influencing Loss to Follow-up among Human Immunodeficiency Virus Exposed Infants in the Early Infant Diagnosis Program in Phalombe, Malawi by Joe Nkhonjera, Leticia C. Suwedi-Kapesa, Benjamin Kumwenda and Alinane Linda Nyondo-Mipando in Global Pediatric Health
Supplemental Material
sj-pdf-2-gph-10.1177_2333794X211004166 – Supplemental material for Factors Influencing Loss to Follow-up among Human Immunodeficiency Virus Exposed Infants in the Early Infant Diagnosis Program in Phalombe, Malawi
Supplemental material, sj-pdf-2-gph-10.1177_2333794X211004166 for Factors Influencing Loss to Follow-up among Human Immunodeficiency Virus Exposed Infants in the Early Infant Diagnosis Program in Phalombe, Malawi by Joe Nkhonjera, Leticia C. Suwedi-Kapesa, Benjamin Kumwenda and Alinane Linda Nyondo-Mipando in Global Pediatric Health
Footnotes
Acknowledgements
We are grateful to all the participants that took part in the study. We are also thankful for the institutional support from the health facilities for allowing us to conduct the study in their facilities. We are especially thankful to study participants for taking their time to talk to us. Special thanks to academic supervisors for their contribution.
Author Contributions
The study was conceptualized developed and conducted by JN under the supervision of BK and ALNM. JN drafted the initial manuscript and the manuscript was further reviewed and edited by LS, BK, and ALNM. All authors read and approved the final manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The corresponding author Joe Nkhonjera sponsored himself.
Ethical Approval and Consent to Participate
Ethical approval was obtained from Malawi’s College of Medicine Research and Ethics Committee (COMREC number P.10/17/2293) prior to commencing the study. Both the Director of Health and Social Services (DHSS) and individual health facilities provided institutional support for the study. We obtained written informed consent from each participant prior to any study procedures. All participants provided written consent for those who could not write a thump print was used. Use of thumb print was approved by ethics committee. Participants were assured that their participation in the study will not affect their receipt of EID services in the subsequent follow up visits. We maintained participants’ confidentiality, anonymity, and privacy by holding interviews in a private and quiet space. We used codes instead of participants’ names in the study summaries. All audios and transcripts were saved in a password protected computer with limited access to the researchers.
Availability of Data and Materials
The datasets used/or analyzed during the current study are available from the corresponding author on reasonable request.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.