
Abstract
Participation of males in the prevention of mother-to-child transmission (PMTCT) programs remains a challenge despite the implementation of guidelines. The study aimed at exploring male involvement in the PMTCT program at a primary health facility in Lilongwe, Malawi. Focus group discussions and in-depth individual interviews were used to collect data from health care workers, men, and women who were attending PMTCT services. Snowball sampling was used to recruit participants who were purposively identified. Alcohol consumption, pressure from work places, stigma, role conflict, denial or nondisclosure of HIV status among women, and lack of awareness were among factors found to hinder male participation in PMTCT services. Therefore, to have an effective PMTCT program, male involvement is needed as this could positively influence the delivery of interventions including antiretroviral treatment among HIV-infected pregnant women. As such, health education awareness campaigns emphasizing the value of men in PMTCT services should be reinforced.
Background
HIV remains a major challenge globally. In sub-Saharan Africa, HIV accounts for 70% of the global burden of the infection, 1 and in Malawi, the HIV prevalence rate is estimated to be 9.2% of the adult population. 2 Women in Malawi are disproportionately affected by HIV, with the prevalence rate being at 14.1% of the 25- to 29-year-old age group. 3 This translates to children who may become HIV positive due to mother-to-child transmission (MTCT). Children get the infection during pregnancy, childbirth, and breastfeeding. 4 Since 2011, efforts in Malawi to prevent and reduce MTCT, especially after the implementation of Option B+, have resulted in a drastic reduction in the MTCT rate. 5 In order to increase the uptake of prevention of mother-to-child transmission (PMTCT) to further reduce MTCT of HIV infection, previous reports have shown that literature states that male involvement is crucial.6-9 Male involvement has been linked with increased adherence to PMTCT. 10
Male involvement remains low despite being registered as an integral part of the implementation of the PMTCT program in sub-Saharan Africa and Malawi specifically.7,11 Male involvement in Malawi has only been partially implemented within PMTCT service provision, despite its inclusion in the PMTCT program guidelines.11,12 In a Malawian study of 467 HIV-positive women enrolled in PMTCT at a district hospital, only 13.7% reported male partner involvement. 4 The reasons for the lack of male involvement could be attributed to shock, disbelief, violence, and discrimination among male partners of pregnant women who disclose their HIV status.13-16 Therefore, fear of disclosure and facing stigma are barriers that hinder women from seeking and receiving male support.17-21 Other barriers to male partner involvement include a lack of male-friendly services,8,22,23 patriarchal cultural beliefs,5,7,24-26 and a lack of knowledge regarding PMTCT.7,16,20 Despite male involvement being encouraged, with substantive strategies on how to include male participation,7,11,12 there are limited studies that explore barriers to male involvement that are specific to the context and cultural setting of Lilongwe, Malawi.
A recent study done in Kenya reported that men are at times unaware of PMTCT services, yet their understanding is the platform for rendering support to a partner. 27 Spousal support and disclosure of an HIV status is influenced by the strength of the relationship with solid relationships creating a safe environment for disclosure. 27 Women are key in spousal support, because in some instances, women do not want their partners accompanying them for PMTCT services, which hinders male involvement. 9
Findings from other studies and cultural contexts cannot be generalized to a different cultural setting and context. Previous studies in Malawi focused on the rural and peri-urban settings.6,25 This study focuses on an urban setting of Lilongwe. Most research has focused on what the importance of male involvement in PMTCT is. This study compares the perceptions of barriers to male involvement among couples. The study also contrasts the male and female perceptions of what male support entails, which reveals a gap in the definitions of male support. There is a gap in the understanding of male involvement among men and women, and as a result of this difference in understanding, there are some barriers to male involvement that the study explores.
Methods
Selection of Study Participants
Inclusion Criteria
Participants recruited were HIV-infected pregnant and postpartum women with a male partner attending PMTCT services at Area 25 Health Centre Clinic, aged 18 years and above, gave consent to participate, or were health care workers at the clinic.
Exclusion Criteria
Women were not included if they did not have a male partner during the time that they were attending or had attended PMTCT, and if they were not attending or had never attended PMTCT at Area 25 Health Centre Clinic. Males were not included if their female partner was not attending or had never attended PMTCT. Health care workers were not included if they had not worked at Area 25 Health Centre Clinic in PMTCT program for more than a year. Those who did not give consent were not included to participate in the study.
Sampling and Recruitment of Study Participants
Health Care Workers Focus Group Discussion Participants
Purposive sampling28,29 technique was used to identify participants for the focus group discussion (FGD). The researcher deliberately sought out people who were able to and were willing to provide the information about barriers to male support, by virtue of knowledge or experience in PMTCT services at the Area 25 Health Centre. The researcher was introduced to the PMTCT health care workers by the manager of the PMTCT services at the health center. To recruit participants, the PMTCT services manager mobilized 6 health care workers who had been working in the PMTCT program for over a year. Three were male and 3 were female, in order to have a balance of perspectives from a gender point of view. The FGD was conducted at the Area 25 Health Centre, and it lasted for 77 minutes, following the structure of the health care worker FGD guide.
Female FGD Participants
The 7 female FGD participants were conveniently sampled. To recruit the participants, the PMTCT services manager and the other health workers identified potential participants based on the researcher’s eligibility criteria. In addition, frequent announcements while conducting health talks and as patients were waiting in queues to receive services were made, and these encouraged women to participate in the study. The women who met the eligibility criteria and who gave consent to participate in the study were asked to meet behind the PMTCT area. This was a private outdoor area within the vicinity of the health center where the FGD was conducted. The discussion lasted for 60 minutes, and the questions asked were based on the female participant FGD guide.
Key Informant Interview Participant
The key informant was purposively selected based on her knowledge and expertise in PMTCT services. Her experience as the focal contact for HIV testing and counselling allowed her to provide insight concerning the PMTCT services at the health center, the barriers and facilitating factors for PMTCT uptake, and the implementation of male support in PMTCT. After she gave consent to participate in the study, the interview was conducted at the Area 25 Health Centre, and it lasted for 45 minutes. The questions that were asked were guided by the key informant in-depth interview guide.
Female In-Depth Interview Participants
Four females were conveniently sampled for in-depth interviews (IDIs). Some of the females were identified because they had attended antenatal care (ANC) or they were at the clinic for the collection of their antiretroviral therapy (ART). Health care workers at Area 25 Health Centre Clinic Antenatal Department and PMTCT Department identified some females who fit the inclusion criteria. The study was explained to each female individually. Thereafter, we obtained informed consent prior to study participation. We conducted in depth interviews at the health care center at a quiet and private outdoor location, following the interview guide. Each interview lasted about 35 minutes.
Male In-Depth Interview Participants
Two males were conveniently sampled for IDIs. Health care workers at Area 25 Health Centre Clinic identified the 2 males who fit the inclusion criteria. The 2 male participants who were selected were at the clinic for collection of their ART. We sought their informed consent and included them in the study after they voluntarily agreed to participate. They met with the researcher and agreed on an appointed date and time when the interviews would be conducted. One participant was interviewed at the health center, and the other participant chose to be interviewed from his workplace in Area 25. Both of these IDIs were conducted following the male partner interview guide, and they lasted up to 35 minutes.
Couples In-Depth Interview Participants
A total of 3 couples (3 men and 3 women) were conveniently sampled. The first phase of sampling was done by health workers at the Area 25 Health Centre by identifying couples who were collecting their ART at Area 25 Health Centre Clinic. Those who showed interest were referred to the researcher. The couples were asked to first discuss with the partner on whether the couple was interested in participating. Only couples where both the woman and the man met the eligibility criteria and gave consent to participate were interviewed. Two of the couples who were collecting ART at the health center were interviewed on the same days that they were recruited, at the health center. One couple chose to be interviewed from their home in Mchezi, which is within the catchment area of Area 25.
We sought mutual consent between the husband and the wife cognizant of the patriarchal culture in this area, which confers the responsibility on making key decisions to a man. It was also important that the couple came to a consensus of participating in the study together to avoid conflict within their households.
The subsequent male and female participants were separately interviewed using the same IDI guide to avert communication barriers due to gender and norms inherent in a patriarchal culture, 7 and to capture differing views of male support required. These interviews lasted between 20 and 45 minutes.
Characteristics of Study Participants
Females in FGDs, IDIs, and Couple IDIs
In total, we included 14 women to participate in the FGD and the IDIs in the study. Seven participated in the female FGD, 4 participated in IDIs, and 3 were in the couple IDIs. The ages of the female participants ranged between 21 years and 42 years, with the median age being 33 years. Of these participants, 7 were pregnant, 6 were postpartum and still attending PMTCT services, and 1 was postpartum and was no longer attending PMTCT services. Eight of the women were unemployed, 1 was formally employed, 4 were self-employed, and 1 did not disclose her employment status. Two of the women had not attended any school at all. Three other women stopped their schooling before completing primary school, and 2 completed primary school as their highest level of education. Six of the women had attended secondary school but did not complete their schooling. One woman completed her secondary education. None of the women had attended college. Eleven of these participants were literate, and 3 were illiterate (Table 1).
Sociodemographic Characteristics of Participants.
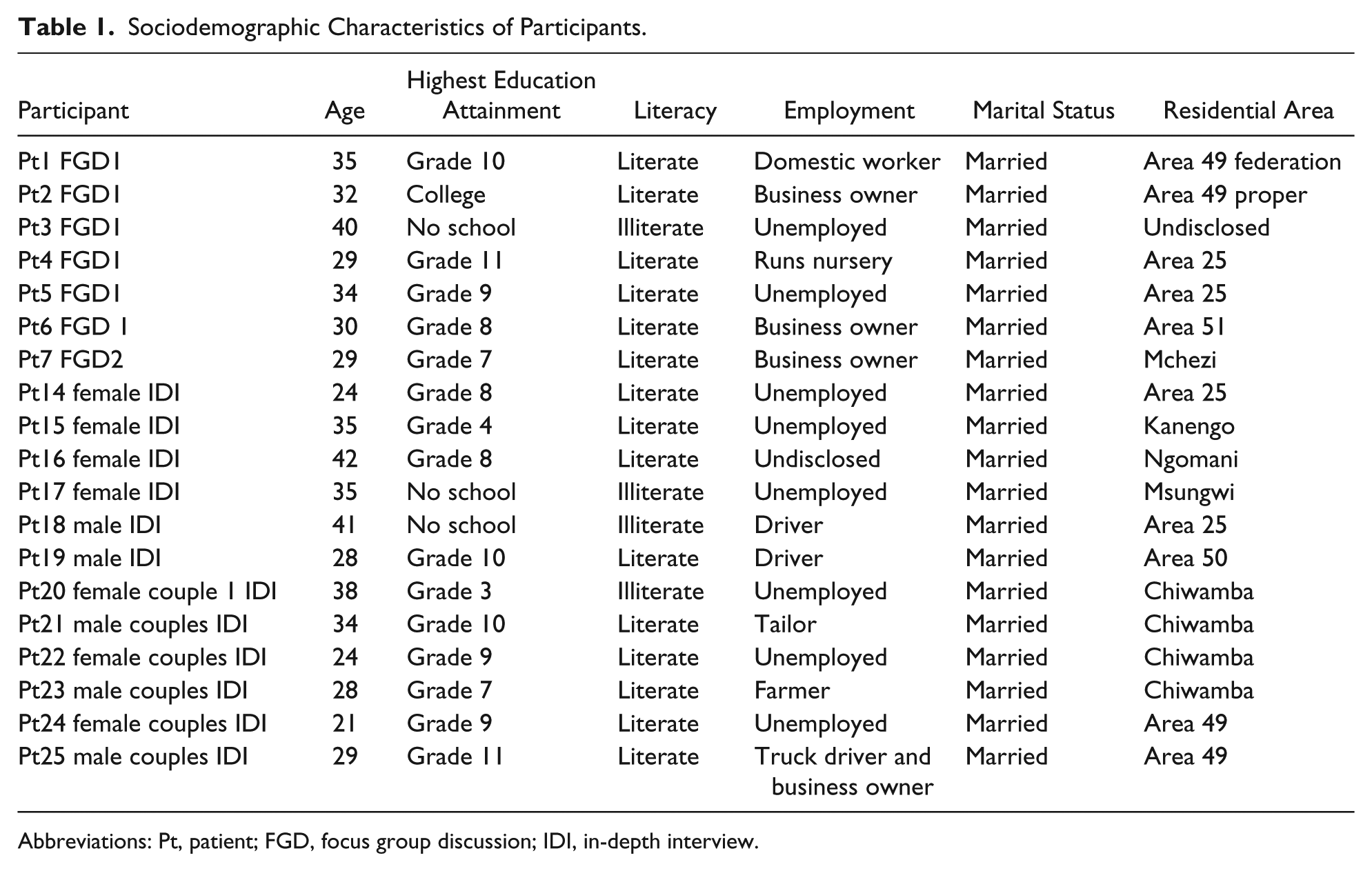
Abbreviations: Pt, patient; FGD, focus group discussion; IDI, in-depth interview.
Males in IDIs and Couple IDIs
We interviewed 5 men in the study. The age of the 2 male IDI participants and 3 males in the couple IDI category ranged between 28 years and 41 years, with the median age being 29 years. Of these participants, 3 had wives who were pregnant and 2 had wives who were postpartum and still attending PMTCT or had attended PMTCT services. Three of these men were employed as drivers, 1 was a self-employed farmer, and 1 was employed as a tailor. One man had never attended any form of schooling, and 1 attended primary school but did not complete his schooling. The other 3 attended secondary school, and only one of these completed his secondary school education. None of the men had attended college. Four of these participants were able to read and write, and one was not able to (Table 1).
Health Care Workers
Of the health care workers who participated in the FGDs, 3 were female and 3 were male. The key informant that participated in the key informant interview was female. All participants had been employed at the center for more than 1 year (Table 1).
Data Analysis
We used a thematic analysis approach as stipulated by Braun and Clarke’s 6-phase framework for thematic analysis to analyze our data. 30 We also developed matrixes to compare and contrast the responses from the various respondents included in the study to highlight the similarities and differences.
Transcription
Data were recorded digitally, transcribed, and translated from the local language Chichewa into English. To prevent straying from the original meaning of responses when translating from Chichewa into English, the researcher familiarized themselves with the digital recordings by listening to them several times while transcribing. Data were checked for quality and consistency by proof-reading the final copy of transcripts and referring to the original audio recordings whenever some clarification was needed.
Familiarization
After transcribing the data, the researcher read each individual transcript many times over and took notes to identify repeated patterns of barriers to male involvement as well as perceptions of male involvement. During this process, notes were being taken and repeated patterns were being marked with highlighters, in order to begin shaping ideas for the coding process. 30
Coding
The data were coded manually. The transcripts were coded by developing notes and marking patterns of the data that were being analyzed and then grouping them into the various codes. 30
Searching for Themes
The codes that were generated were then analyzed and sorted into various potential themes and subthemes. Tables and mind maps were used to categorize the codes into potential themes.
Reviewing Themes
The themes and subthemes were reviewed and refined. First, all the codes that had been sorted into potential themes were read in order to verify whether they formed a cohesive pattern in line with the theme. 30 Codes that were found to be incoherent with the themes resulted in a changing of the theme, development of a new theme entirely, merging some themes, moving the codes to another theme, or discarding of some themes. 30 The result of this refining was a thematic map. The thematic map was refined by rereading the codes and transcripts developed earlier in order to identify any codes and themes that might have been missed, and also to examine if the thematic map was an accurate representation of the data collected. 30
Ethical Approval
The study was approved by Monash University Human Research and Ethics Committee (Approval Certificate Number 2016-0668-959). Authority to conduct the study at the Area 25 Health Centre was given by the Lilongwe District Health Office. We obtained written informed consent from all participants who were able to write and verbal consent from those who could not write prior to study participation. To preserve the participants’ confidentiality, we used identification codes rather than disclosing the names of the participants in the processing of research data. All IDIs and FGDs were conducted in a private space within the vicinity of the health center except for 1 couple interview that was conducted at their home and 1 interview with a male partner that was conducted at his workplace on his suggestion. The risk of causing tension among couples was minimized by ensuring that couples decided together on whether they wanted to participate in the study, as well as letting them know that the nature of the study did not allow the researcher to disclose to the other partner what they discussed in the interview.
Findings
The study reveals several relevant issues that impede male involvement in the PMTCT services. The barriers to male involvement originates from challenges with disclosure with all its associated factors; denial of an HIV status; difficulties in convincing a male partner to be involved in PMTCT; cultural and gender dilemmas; lack of knowledge on PMTCT; knowledge gaps within the PMTCT policy; socioeconomic demands; and the distance to the facility. The study also shows that women had a more extensive definition and understanding of what male support involves compared with their male partners (Tables 2 and 3).
Perceptions of Male Support Between Male and Female Partners.

Abbreviation: HTC, HIV testing and counselling.
Main Themes.

Abbreviation: PMTCT, prevention of mother-to-child transmission.
Participants’ Perception of Male Support
Women perceived male support as being reminded to take medication; emotional support in the form of allaying anxiety; being accompanied to clinic appointments and HIV testing and counselling; nutritional support through husbands ensuring that their dietary needs are met; home support that involved being assisted with household chores; husbands agreeing to use condoms; and last, husbands providing them with financial support such as transport money for the appointments.
When asked what kind of support she expected from her husband, one woman responded in the following way: I expect my husband to make sure that I do not lose heart and get anxious. I want him to remind me of my hospital appointment dates as well as reminding me to take my medication at the times that I am supposed to. (Female, in-depth interview)
Another woman stated ways in which she thought that male support was displayed: One way to show support can be reminding the woman to take medication and also helping the woman with household chores, and also looking after the children and bringing them to the hospital when they fall sick. (Female, focus group discussion)
When asked in what additional ways husbands can show support to their wives who attend PMTCT, another woman from the FGD said the following: But also, if he accepted your status, he can support you in your nutritious needs based on the counsel that you receive when you come here to the hospital. (Female, focus group discussion)
One woman who was interviewed highlighted what form of support she would have loved to see from her husband, that she was not receiving: The main way he can support me is taking medication and using condoms. (Female, couple in-depth interview)
The most commonly stated form of support that was mentioned by male partners was reminding their wife to take medication.
When asked if he supports his wife, one male participant answered in the following way: Yes, I support her. I tell her that we need to protect our child I made sure that medication was not skipped. Our child was found HIV negative because I made sure that my wife did not miss her hospital dates and that she took her medication when she was supposed to. (Male, in-depth interview)
In support of this, another man had a similar response when asked how he supported his wife who was attending PMTCT: I make sure that she takes her medication and that she remembers her hospital appointments. (Male, in-depth interview)
The common perceptions held by both women and men were the following: reminding the wife to take medication, helping the wife with labor preparations, and assisting the wife with household work. It is worthy to note that wives perceived male support in a more extensive way compared with the male partners.
Barriers to Male Involvement in PMTCT
Disclosure Dilemmas and Stigma Issues
Disclosure dilemmas were found to be major impeding factors to up-taking and adherence to PMTCT for both pregnant mothers and their spouses/partners. These dilemmas were also compounded by the existing stigmas prevalent in the communities regarding HIV-positive people. There was a dilemma of disclosure between spouses and a dilemma of disclosure in general.
Disclosure Dilemmas Between Spouses
Disclosure dilemmas between spouses were mentioned as a major impeding factor as the pregnant mothers did not want to disclose the positive diagnosis to their spouses/partners for fear of repercussions. The following quote aptly explains the fear and worry embedded in the disclosure of HIV-positive status: It affects people because they worry.
Furthermore, in the event of a positive HIV diagnosis, there was the inherent fear of other people finding out and that had a direct impact on their adherence to PMTCT. Study participants reported that they were also worried about how to deal with the diagnosis in the wider community context in as far as stigma issues were concerned. A male participant reported: If they [women] go and get tested, they will be found HIV positive, and when people find out, then that will be the end of them. (Male, in-depth interview)
To overcome this dilemma and the related stigma issues, couples often resorted to choosing health facilities that were far away from their communities. A male participant aptly put it this way: From where we live, it was difficult for both of us to come here together. We chose this hospital because we were afraid of being stigmatized. This place is far from our community and the people that we know. There is one hospital we could even walk to in the area close to our home. (Male, in-depth interview)
Disclosure Dilemma in General
In the same vein, there is also the dilemma that comes with the disclosure of the HIV-positive diagnosis in general. The stigma attached with a positive diagnosis needed courage to even disclose that the person is HIV positive. Hence, The courage to disclose.
Disclosure of HIV status is a complex matter especially when one has to consider the impact on one’s life after disclosure. Dealing with the post-disclosure consequences such as the already disclosed status at the health center and the timing of the disclosure to the spouse were found to be extremely difficult moments of one’s life. The following quotes provide an insight into this issue: I took 2 weeks to gather courage to disclose my status to him because he was not here with me when I came for HIV testing. (Female, focus group discussion) When I disclosed my status to my husband when I was pregnant, he was very upset with me and he left me because I was found to be HIV positive. When he was away and thought things through, he came back to me and realized that what he did was wrong. . . . It is God’s grace that he came back. (Female, focus group discussion)
Then it was also dependent on who disclosed first regarding uncertainty prior to a marriage and post-marriage consequences. A few male respondents said the following: I used to live alone. . . . I really wanted to get married. I had that as a target. I figured that if I told her my status before we got married, she never would have wanted to marry me. (Male, in-depth interview) Some women fear that their marriage will end if they are found HIV positive and they disclose to their husband. They wait for their husband to be the first to disclose his HIV status to them. (Male, in-depth interview)
Reaction to HIV-Positive Diagnosis and Disclosure
After the positive diagnosis, if a person is not properly counselled prior to taking the test, a number of reactions may be presented. One of such is denial of the diagnosis. In this study, it was found that when study participants revealed the positive diagnosis to their spouses, the latter went into denial of the HIV-positive status. Thus, Refuses to accept . . . status.
A female study participant highlighted that her husband was in denial of her HIV-positive status and that he did not want to accompany her to the clinic for PMTCT services. She said, We found that those of us that chose to start taking ARTs were very few, whose husbands also accepted their status. A lot of us were saying that their husbands do not accept their status and would not set foot at the health center. (Female, in-depth interview)
This was concurred to by a male study participant who said: It’s painful for a woman when her husband does not accept her status. You find that a woman will be found HIV positive at ANC and when she has to explain her status to her husband, the husband refuses to accept her status. It makes women anxious. You find that for some couples, one partner is HIV positive and the other is HIV negative. So when a woman is being denied by her husband, I am sure it is very painful. (Male, in-depth interview)
One participant in the FGD stated how the denial of HIV status by male partners jeopardized PMTCT: But for those husbands that do not accept the status, and are cruel, now this increases the risk of the child being born HIV positive. Some men become cruel to their wives when they are HIV positive. (Female, focus group discussion)
Finding the Opportune Moment to Disclose the HIV-Positive Status
Related to the disclosure dilemmas is the fact the person who is HIV positive tries to find an opportune moment to disclose the status to the spouse. Thus, Don’t know how to disclose their status.
This finding was revealed during the health provider FGD. Participants reported that most of their clients struggle to find a way to share the HIV-positive status to their spouses. Thus, breaking the news and preparing themselves on how to deal with the anticipated reactive response from the receiving spouse required some skills.
Sometimes I think it depends on us women. . . . The approach that we take with our husbands. You need to know your husbands and . . . understand how they react when you speak to them in certain ways. So, you need to tell them gently and humbly, so that he should understand and . . . willing to listen. (Health care worker, focus group discussion)
An example shared was the following: Some women are short tempered, and they don’t know how to disclose their status to their husbands in a way that is conducive. If disclosed well, the husband can receive the news well and be encouraged to visit the clinic for testing. (Health care worker, focus group discussion)
Lack of Male Involvement and Adherence to PMTCT
As a result of the various factors that have been outlined prior, the most important impact on the disclosure dilemma was the fact that it affects male involvement and hence affects adherence to PMTCT.
Male involvement and adherence.
An example of the implication of not knowing of the other spouse’s HIV status was shared during the health provider FGD. The FGD revealed that lack of knowledge of the spouse’s HIV-positive status affected and compromised PMTCT treatment adherence. One health care worker said, Sometimes when we go into the field and conduct a pill count, we find that some women have more pills than they are supposed to because when they have not disclosed their status, they will say that because their husband was around, it was difficult for them to drink the pills. So male involvement and adherence for the women go together. (Health care worker, focus group discussion)
Apart from the discomfort of nondisclosure resulting in nonadherence was the typical lack of interest by the male partner after disclosure resulting into the wife taking the responsibility for her treatment and that of her children who were also on treatment. One woman in the FGD said, It makes me sad because my husband does not really care about adhering to ART. So sometimes I do indeed forget to take my medication and he does not really support me by reminding me or reminding me to give my other child medication. When I ask for his support in this way, he says that he does not take medication and so he cannot be bothered to be reminding me about when to take my medication. (Female, focus group discussion)
Challenges Encountered in Males to Participate in PMTCT Services
The study found that to convince males to participate effectively and to keep them engaged in PMTCT was not an easy task. The difficulties included ensuring that the couples get tested together and cultural dilemmas on what is considered a female-dominated issue.
Get tested together.
The study found that there was usually a problem if one partner was tested and not the other. A female study participant revealed, In some cases, you find that a husband will be HIV positive and on treatments but will not tell the wife. I think that this is not smart and it is better for the couple to agree to get tested together and to encourage and to support each other. (Female, in-depth interview)
In addition, the findings show that being psychologically ready to be tested was an issue. One study participant revealed that he was so afraid of being found HIV positive that it took him 4 years after his wife was found HIV positive to muster the courage to go and get tested. He said, At the time my wife had come for HIV testing, it took me a much longer time to come to get tested because I was afraid. I thought that if I get tested, it would just make me feel some type of way. But after 4 years, I figured that I should just get tested so that I can move on with my life. (Male, in-depth interview)
The study also revealed that sometimes there were cases where there were discordant couples who need to be counselled and tested together. A health care worker said, Sometimes, more so now than ever, there are a number of cases where the husband is actually HIV negative and the wife is HIV positive. So, when they get tested together, it is helpful to counsel them . . . to strengthen their marriage. This is different from when a woman comes here and gets tested on her own because should the husband ever discover that the woman is on ART, in some cases, you find that the husband secretly goes for HIV testing himself. When he finds that he is HIV negative, it is very easy for the marriage to come to an end. (Health care worker, focus group discussion)
However, the study found that this was not as easy as it seems. A female respondent said, There are some women that come here to ANC and for HIV testing alone . . . when they ask for their husband to accompany them . . . the husband will refuse and tell the wife to go to PMTCT on her own. . . . In some cases, you find that a husband will be HIV positive and on treatment but will not tell the wife. (Female, couple in-depth interview)
Cultural and Gender Dilemmas Impeding Male Support in Use of PMTCT Services
The study revealed that the study participants experienced the influence of the prevailing culture especially in cases where the issues were considered female domain.
In Malawi, issues relating to ANC, PMTCT, and even going to access health services are considered women-only issues. Traditionally, men do not go to health centers unless they are very ill themselves. As such, the structural environment of the health center and its related services posed a major challenge for the men accompanying their spouses. The whole environment was not conducive to their participation. A common theme was the following: What business do they have being around all the women there?
A health care worker said, At first, the clinics were built with the design that shows that they did not think of the future. With our culture, men think that ANC is for women and not men. Now, we have discovered that men are also important, and they need to know information about PMTCT and other services that are in the clinic. So, the setup that is at the antenatal clinic was conducive for women only and not men.
The health care worker continued, The structures have remained the same. We want men to be involved, and yet we have not changed the environment to be suitable for these men. Like how they sit for example. Some men feel shy among many women. . . . They want to be separated. (Health care worker—Focal person for HIV counselling and testing)
Furthermore, due to the fact that the health center is considered a women-only center, most men felt out of place and did not come along with their spouses. A health care worker said, For example, at ANC, there will be very many women, maybe up to 100 and there will only be about 5 men. Men will be thinking that there are far too many women. . . . So many men feel shy to be among such a big group of women. (Health care worker, focus group discussion)
The few men who did accompany their spouses tended to rather wait outside the center: In some cases, we find that a man will indeed accompany his wife to PMTCT, but he does not sit with her. Rather he waits at the gate. Only when we ask the women about the whereabouts of their husband is when they tell us that their husbands are with them but are waiting at the gate because they are too shy to be among women and other people at PMTCT. (Health care worker, focus group discussion) Men have no place in such matters.
Another health care worker highlighted how traditional beliefs hinder male support: Some believe that culturally, certain things, especially pregnancy related matters are for women and . . . men have no place in such matters. They believe that their contribution to the pregnancy ends and impregnating the woman and that’s it. Although the information about escorting and supporting women undergoing PMTCT goes out, some men are still behind and they still do not come. (Health care worker, focus group discussion)
When asked how culture may hinder male support, an interviewee put it in this way: Some men think that if they escort their wife to the hospital, they will be thought of as dumb. For three quarters of the men, having a child is something for them to boast about. But when their wife is pregnant, a lot of men are ashamed to escort their wife. A lot of men are ashamed to be seen with a pregnant woman because some of them believe that they will not be seen as youthful because of that. (Male, in-depth interview)
The Traditional Role of Male in Society
The traditional role of men in Malawi is to provide for their families. This study found that most of the men were involved in some economic activities such as being employed or running some informal trade. Most of the women in this study reported that their spouses were always busy. Thus, He is always busy.
A lot of men living within the health center surroundings were employed in the neighboring industrial areas. As a result, these men were usually unavailable to attend the clinic visits at the health facility because their employers would not give them time off to work.
What hinders my husband from supporting me is his work. He is employed so when you are working for a company, you cannot just skip work as you please or else you will get fired. But without him going to work, then we will have nothing to eat and things will not go well for us. (Female, focus group discussion)
The issue of sustaining a stable income and ensuring the needs of the family are met by the men took precedence over accompanying their wife as stated by this participant.
A lot of us in this area have come from various places to make money by running our own business or seeking employment. The ones that run their businesses know that they need to work for their families to eat. So, the husband has to work and strive, for the business to succeed, in order to provide for his family. Because of this, the husband sends the wife off to PMTCT on her own. (Health care worker, focus group discussion)
The traditional role of a man is to be the “head” of his household, and this means that he makes most of the decisions in the home without consulting the wife. Thus, a few study respondents said, Women cannot demand and tell us what to do.
This traditional perceived male role of the “head” of the household resulted in an automated role of women adopting the submissive, passive role. A few health care workers revealed this fact in a FGD. One said, It is a common view in Malawian culture that we men are the heads of our households and that means that women cannot demand and tell us what to do. (Health care worker, focus group discussion)
The Intertwined Male Dependence Versus Being Supportive and Adherence to Treatment
The study found that male support provided to their spouses who were attending PMTCT with the much-needed psychosocial support for the latter needed to continue with the treatment. By attending and accompanying their spouses to attend PMTCT services, they enabled their spouse to have a better quality of life, and thus improving their well-being. One woman said, I would live a very troubled life if my husband were to stop supporting me. He makes me strong. If I were on my own, I would not be able to work and I would not be able to take care of myself. (Female, in-depth interview)
It could also lead to Skipping appointment dates, and I would not know what I am supposed to do. That would put my life in danger. (Female, in-depth interview)
Therefore, the approach is to Just have to get on with it . . . come to the hospital. But it makes life very bitter. (Female, focus group discussion)
In other instances, it was more than just having to get on with it despite all the efforts because, He feels ashamed, and he eventually begins to help you. No woman should stop using PMTCT services because the husband is not supportive because this leaves the life of the woman at risk and the life of the baby at risk as well. (Female, focus group discussion)
The 2 latter quotes show that even though the male spouse support was provided, the relationships took a lot of strain.
Low Level of Education
The study found that most of the study participants had low levels of education that affected the way they responded to their spouses’ request for support. A male partner with a low education status or illiterate is not as open-minded to PMTCT as one that was educated. Evidently, if an educated husband has a wife that is on PMTCT, he will most likely understand what is required of him and hence accompany his wife for PMTCT services. Such a man is open-minded and more receptive to the information and counselling that is received at PMTCT. A health care worker emphasized the issue by saying, Another barrier that I see is the level of education. Someone that has not gone to school has very little knowledge and it is, therefore, hard for them to see the importance of male support. Some hospitals allow husbands to visit their wives when they are recovering after delivery. But if someone did not go to school, they think that it is vulgar to be with their wife when she is in labor or after she delivers her baby and is recovering. (Health care worker, focus group discussion)
A male participant also said, I also think that school is another factor. I have found that with most of the people that reject information, it comes back to their level of education. They will think that the information is useless. (Male, couple in-depth interview)
Knowledge Gaps in Policy Adherence
There is a policy that was designed in Malawi to ensure that there is partner involvement in the issues of sexual and reproductive health, and this includes HIV-related services. However, this study revealed that was lack of knowledge regarding this policy among men. The commitment to support in PMTCT is more than just agreeing to get tested together. One of the issues is the policy of male spouse obligatory support in the PMTCT. A common theme under this finding was that of partner support.
He would work hard at supporting me and I would work hard too.
The question whether the male spouse is aware, has the necessary knowledge, understands, and has the ability to come to terms with what PMTCT support entails is illustrated in the following quotes. The willingness “to go that extra mile” to support the female spouse was stated in this way: I think that he does not know the policy that the hospital has. So maybe if he had knowledge about it, he would work hard at supporting me and I would work hard too. (Female, couple in-depth interview)
Women in the FGD stated that it is difficult to receive support from a husband who does not know what support is needed.
I have seen that very few men understand what exactly you really need when you are trying to explain it to them. It takes them a long time to understand what you need. So, this increases problems. (Female, focus group discussion)
The knowledge gap was acknowledged by some of the men in the study who then requested to be assisted to acquire such knowledge to provide the support that their spouses needed. A typical example in this regard was illustrated by a male spouse to provide the support required within the PMTCT context.
If you were to tell me ways in which I can support my wife more, I would do it. I do want to support her. I’m not really certain of all the ways in which I can support her. (Male, in-depth interview)
The issue of couples coming to the health center was also mentioned as a way of assisting the couples to be on the same page as far as knowledge was concerned. Health care workers emphasized that they have an advocacy role, which they use to limit the knowledge gap that may exist between spouses in that they create a platform to provide support to the spouses. Health care workers also explained that the issues relating to PMTCT are very complex and difficult for the female spouse to manage on her own.
When they come here together, they hear everything together, and if this is the case, there are no difficulties when they need to help each other accordingly at home. But when a woman comes alone, she is not able to explain to her husband everything as it was explained to her at the hospital, and because of this the husband cannot help her. (Health care worker, focus group discussion)
Socioeconomic Reasons for Not Supporting the Spouses
The study also found that most men found it difficult to manage their finances as they spent their money on things that were not basic necessities of life such as alcohol. Resource management was a real challenge for most men in this study, and they did not want to share their money with their spouses. The most common phrase was the following: When he finds money, my husband drinks too much alcohol. When he makes money, he spends it on alcohol. He does not see the benefit of giving me any money when he can spend on alcohol. (Female, in-depth interview)
To overcome this distress, female partners often resorted to a plea to get cooperation. This took some talking to and sensitizing their male counterpart on the negative effects of alcohol intake.
In the past, he used to drink too much alcohol. I talked and reasoned with him and pleaded with him to stop because it used to give me anxiety. So now he has stopped taking alcohol indeed. (Female, in-depth interview)
On the other hand, the male partner was appraised for the hard work and managing resources efficiently as illustrated by this participant.
Sometimes, it is hard for him to provide transport money. So sometimes, when the day of my hospital appointment arrives, it is difficult because he will not have money because his work is very hard but when he finds money, he gives me. (Female, couple in-depth interview)
Distance to Hospital
Couples who lived far away from the hospital were less likely to attend PMTCT together due to a lack of finances for transport. It was very expensive for husbands to provide transport for their wife in these circumstances. The couples prioritized getting the woman to PMTCT, which they could barely afford. A male participant highlighted that living far from the health center affected his ability to support his spouse. He said, If we can’t both make it, then she can go to hospital on her own; but if there is the freedom and availability of transport, then we can go to the hospital together. From where we live, it was difficult for the both of us to come here together. (Male, couple in-depth interview)
Discussion
The study has revealed that there are a number of factors that impede men’s ability to provide support to their spouses who are accessing PMTCT services. These included the following: disclosure dilemmas and stigma; lack of male involvement in PMTCT services; cultural/traditional and gender roles of men and women; lack of education and knowledge; and socioeconomic reasons. Ultimately, these can be discussed by addressing them as socioeconomic barriers, structural barriers, social barriers, cultural barriers, and effects of lack of male support on the uptake of PMTCT.
Socioeconomic Barriers
The socioeconomic issues that emerged in this study that were barriers for men supporting their wife in PMTCT were alcohol abuse and distance from the hospital. With alcohol abuse, it was reported that this hindered some men from providing financial support. Rather than providing finances for transport and nutrition, these husbands were reported to spend their finances on alcohol. The alcohol abuse resulted in anxiety among the women who were attending PMTCT. When men could not provide financially for their wife, this prevented a woman from attending PMTCT scheduled appointment dates and collection of ART. It also meant that the nutritional needs advised by health care workers for women in PMTCT were not met. Evidently, this minimized the uptake of PMTCT services and adherence to PMTCT treatments. A similar study conducted in Zambia explored barriers to male participation in PMTCT and alcohol abuse was found to be one of the barriers. Men that abused alcohol did not provide support for women undergoing PMTCT. 8 The men that abused alcohol would insist on having unprotected sex with their wife and threaten divorce if the wife refused, which would leave the wife without any financial support. 8 Alcohol abuse not only threatened a lack of financial support but also resulted in a lack of emotional support, because women would be fearful and anxious about their future.
Structural Barriers
As for distance from the hospital, it was found that the farther away from the hospital a couple lived, the more difficult the husband found it to provide adequate finances for transport money to the health center. This limited the participation of husbands in PMTCT as well as a woman’s attendance to these services. This supports findings from a study in Nigeria on barriers to uptake of PMTCT for women. Women highlighted that high transport costs, which their husbands could not afford, as one of the major reasons for skipping scheduled ANC visits. 17 For couples living too far from the health center, women were not always able to make it to the health center on their scheduled appointment dates. In a Malawian study in the rural district of Ntcheu, 72.7% of women reports the ANC clinic being too far as a reason for missing scheduled ANC appointments. 31 In some cases, the husband was only able to provide transport for one, and therefore, the husbands could not accompany their wives. When a husband is not able to participate in PMTCT services, it causes difficulty in communication about what type of support a woman requires. This is because when a husband does not attend PMTCT and does not receive the same counsel a woman does at PMTCT, it is hard for the woman to communicate and to convince her husband of what is required of him in terms of support and participation. The result is a lack of awareness among male partners. This finding is consistent with findings from a study in rural South Africa where 68.5% of men did not attend ANC with their wives, and ultimately, the lack of the male partner involvement resulted in poor communication between men and their partner involved in PMTCT. 32
For some, being far from the health facility was not optional because that was the closest hospital to their residential area where they could seek services. However, there were some who deliberately chose the health facility despite there being other health centers much closer to their residential area. The reason that was highlighted for choosing a health center far from their residential area was for the sake of avoiding stigma from the community. Self-preservation from stigma took precedence over having a center that is nearby with affordable transportation costs. Stigma and discrimination were a pervasive barrier that transcends more than just social and cultural barriers but is also interlinked with the socioeconomic barriers that have been mentioned. In a descriptive study in Makurdi, Nigeria, 90.5% of women missed their scheduled ANC visits because they did not want people to see them or find them. 17
Social Barriers
As for the social barriers, employment was identified to be a key barrier for male support. Males that were employed were less likely to find time to support their wife in PMTCT by attending the services with their spouse. Male partners were mostly employed in the health center’s neighboring industrial area, Kanengo, and did not have time to accompany women to PMTCT. It was not easy for most of these men to take time off work because this risked putting their families under financial strain. A study in Uganda identified males seeking to make ends meet and to provide for their family as their priority and a barrier to attend ANC with their partners. 10 In this study, female partners and male partners stated that they recognized the importance of males attending PMTCT with their wife; however, it was not always possible. 10 Despite the fact that the male partners were mostly unable to attend PMTCT, their work allowed them to provide financial support for their wife. The men viewed attendance to PMTCT as important but not as crucial as their role as a breadwinner and provider for their families. Most female partners, therefore, had no expectation of their male partner to always accompany them, but instead they expected financial support. However, by negating PMTCT attendance to provide financial support, the men missed out on receiving information and counselling together with their wife. This, therefore, resulted in a lack of awareness among some of the men because the wife was not always able to properly communicate what she was told at the hospital, or when she did, the husbands did not take the wife seriously.26,32
Disclosure of HIV status was among the social support barriers that were identified in this study. Fear of disclosure and nondisclosure went hand in hand. Most of the partners would not disclose their status due to fear of the reaction of the partner and fear of losing their marriage. This is evidenced by a study in South Africa on the barriers of male participation in MTCT services, which reported that women were afraid to disclose their HIV status because they wanted to preserve their marriage. 22 Nondisclosure resulted in decreased adherence to treatments and missed appointments. Some partners went to the extreme of taking their pills in secret in order to keep their HIV status a secret from their partner. This resulted in skipping doses of ART if their partner was around and therefore preventing adherence to ART. It also resulted in women not attending PMTCT services after discovering their HIV status and being initiated on Option B+. Several studies exploring barriers and facilitators for PMTCT adherence to treatment from the time of HIV diagnosis at the HIV clinic stated that nonattendance of HIV services and delayed attendance of HIV care services were associated with nondisclosure.21,27,33-35 When a partner is unaware of the HIV status of their spouse, they cannot initiate any support for a wife in PMTCT. This also results in a lack of awareness of the male partner on how he can support his wife and the importance of doing so. Furthermore, it is evident whatever the pervasive stigma there is a direct association between the fear of disclosure and being afraid of being stigmatized by one’s partner.
Stigma and discrimination are barriers that are interrelated with several other barriers. As mentioned, nondisclosure was associated with a fear of being stigmatized. Stigma also resulted in some couples accessing the health center since it was far from their community but demanded a lot of transport money. Fear of stigma also resulted in unsupportive behaviors among male partners who included refusal to get tested and denying the status of their wife, which resulted in marital tension.6,7,22,36 Another barrier that is interlinked with stigma is having HIV discordant status among the couples. When males were found HIV negative and their wife HIV positive, a lot of the wives carried the additional burden of anxiously wondering whether their marriages would carry on and if they would be stigmatized by their spouse. In support of this, a study in Ethiopia that explored barriers to the effectiveness of PMTCT programs reported stigma among one of the top barriers. 20 Women were said to be unlikely to return to the hospital where they got diagnosed for ART initiation. 20
Cultural Barriers
As mentioned earlier, culturally, some men in Malawi are not comfortable being among a big crowd of women, especially at ANC or PMTCT. These have predominantly been considered as women-only services. The structures at these PMTCT services have been reported to only be female-friendly and not very accommodating to the males. Men feel uncomfortable sitting among a large crowd of women, and the services do not have designated seating areas for men. Shyness, therefore, prevents the men from participating on PMTCT if they attend, or some are simply reluctant to attend PMTCT because it is not male-friendly. A study in Tanzania reports men being reluctant to participate in ANC activities because culturally, ANC was recognized as a service for women and children and not men. 37 Furthermore, some men are more concerned with trying to uphold the traditional norms where the role of the man is to provide financially for the family, and the role of the woman is anything that is related with pregnancy and raising children. Therefore, when a man is asked to escort a woman to PMTCT, where he knows he will be among a lot of women, he is reluctant to go because it is believed that he will be perceived as emasculated and dumb. This is evidenced by several studies that report that men shy away from PMTCT programs because of their culture that gives them a fear of being seen as less than what a man should be.26,31,37
However, there is a sharp contrast between men who have a high educational attainment compared with those with a low educational attainment. Men with higher educational attainment reported not being shy and were more open-minded to participating in PMTCT programs, despite traditional norms. Men with lower educational attainment were more likely to be reluctant to participate in PMTCT programs and more likely to subscribe to the traditional beliefs. In support of this, there is a study that was conducted in Ethiopia on male support in PMTCT that shows that the higher the educational attainment of a male partner, the more likely he was to participate in PMTCT. 38 The study found that males with an education level of above grade 12 were almost 4 times more likely to be involved in PMTCT than those who did not have education level. 38
Effects of Lack of Male Support on the Uptake of PMTCT
Literature highlights that a lack of male support in PMTCT results in women not adhering to PMTCT regimen and lower uptake of PMTCT services. When a woman enrolled in PMTCT services lacks male support from her husband, it increases the likelihood of nonadherence to ART and skipping hospital appointments. This is evidenced by a cross-sectional study in Ethiopia, which showed that HIV-positive pregnant mothers who had male support had 8 times more odds to adhere to PMTCT care. 39
In addition to this, a cross-sectional cohort study on the association of male support with uptake of PMTCT in Malawi showed that male partner involvement for women enrolled in PMTCT was significantly associated with completion of follow-up in the PMTCT program. 4 However, in contrast to these findings, it was reported that when a woman has been adequately empowered, a lack of male support has no direct impact on her adherence and uptake of PMTCT services. 18 A woman that has been empowered continues to attend PMTCT services and adhere to ART even in the absence of male support. 18 The lack of male support was directly linked with increased stress, anxiety, and depression, but did not affect the adherence. This is supported by one study on perceptions that Sudanese women had on PMTCT. 18 It was found that doctors were more influential than husbands about HIV testing, which is one part of PMTCT. 18 These findings are similar to those of this study, whereby some women that refused to let a lack of male support disturb their adherence showed that their husbands were not the most influential people in their decision to attend PMTCT.
This study identified several issues from health professionals and the attending spouses, which the local health facility can use to modify, refine, or develop strategies and interventions to enhance the male support more especially with managing resources at a household level and the implications for the spouses and beyond. In addition, there was a need for conducting seminars and workshops with industries to allow their workers to attend PMTCT clinic with their spouses.
Limitations of the Study
The study sample size for male participants was limiting. The ideal would have been to have a larger sample of male participants. However, this was a challenge as most potential study participants were not available due to work commitments and obligations. The study also suffered from study participants not willing to share in-depth information regarding the topic as compared with other studies on the same issue. This could be attributed to the sensitive nature of the topic of HIV in this community. Last, the data collected in this study cannot be generalized for the country as it was qualitative in nature and hence was looking for in-depth rich data that could assist in explaining the phenomenon under investigation.
Conclusion
This study highlighted similarities to other studies on the issues pertaining to male participation and support in terms of PMTCT within the sub-Saharan African context. Of importance are the specific issues such as resource sharing, the traditional dominant role of the male spouse as the breadwinner, and the dependent female spouse to take responsibility and ownership of the maternal aspect. From the male perspective, the health center was not conducive for male spouse attendees as it created the potential for stigma. In order to increase male involvement in PMTCT, there is a need for field visits and awareness campaigns, which will include education programs and health care workers engaging with community through encouraging community members to become active in promoting male involvement. Another approach would be to begin to engage influential community leaders and village headmen in scaling up of community awareness campaigns on the importance of male support in PMTCT services.
Footnotes
Author Contributions
Conceived and designed the study: NN LM PN. Analysed the data: NN LM PN. Wrote the paper and Reviewed it for intellectual content and approved the final version: NN LM CM NM PN.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.