
Abstract
Sacro coccygeal teratoma (SCT) is the most common extra gonadal neoplasm in the pre sacral area occurring in neonatal period. They mostly occur in the midline with a female preponderance. They are usually attached to coccyx, They are believed to be arising from totipotent cells that originate from primitive knot (Hensen’s node), hence are usually attached to coccyx. Infection in a sacrococcygeal teratoma has been rarely reported. Here is a report of a case of vague gluteal mass in a neonate and challenges in its diagnosis and management.
Introduction
Though they can occur at any site, sacro coccygeal region is the most common location in neonates as well as in children with an incidence of 1 in 35 000 to 1 in 40 000 live births with female to male ration of 4:1.1,2 Teratomas arise at second to third week of gestation from totipotent cells of primitive knot, a remnant of primitive streak in the coccygeal region. They can be asymptomatic or have severe cardiac failure with foetal/neonatal as well as maternal deaths.1,2
Clinical Summary
A 20 days old male baby born by full term vaginal delivery to gravid 1 mother with a birth weight of 3.6 kg by non consanguineous marriage ; brought to us with history of right gluteal swelling and painful right lower limb movement noticed since 10 days. The antenatal history as well as each trimestral sonographic scans were essentially normal. Baby had received routine vitamin k injection on right thigh on day 2 of life by a health professional.
Baby was absolutely normal till day 10. Mother noticed a vague swelling in the right gluteal region with painful right lower limb movement. Sonography showed vague right gluteal mass with varied cystic septated heteroechoic lesion of 10 × 6 cm extending into the abdomen with septations occupying most of the pelvis and extending into the abdominal cavity with internal echoes . Baby was clinically stable without any anomalies; had restricted right lower limb movements. There was a vague, ill defined mildly tender mass (10 cm × 6 cm)without any redness in the right gluteal region, deep to the muscles extending up to inguinal region anteriorly and to upper third of right thigh posteriorly (Figure 1A and B). There was firm mass palpable per abdomen mainly in the right iliac fossa with a size of 6 cm × 4 cm. Contrast enhanced Computed tomography (CECT) was done showed predominantly cystic mass of size 10 cm × 6 cm in the right gluteal region extending to right upper posterior thigh (Figure 1C and D). The cystic mass was having extension into the pelvis as well into the abdomen with septations and internal echoes with bilateral hydrouretronephrosis due to compression. His alfa fetoprotein (AFP) and beta human chorionic gonadotrophin (βHCG) as well as lactate dehydrogenase (LDH) levels essentially normal.
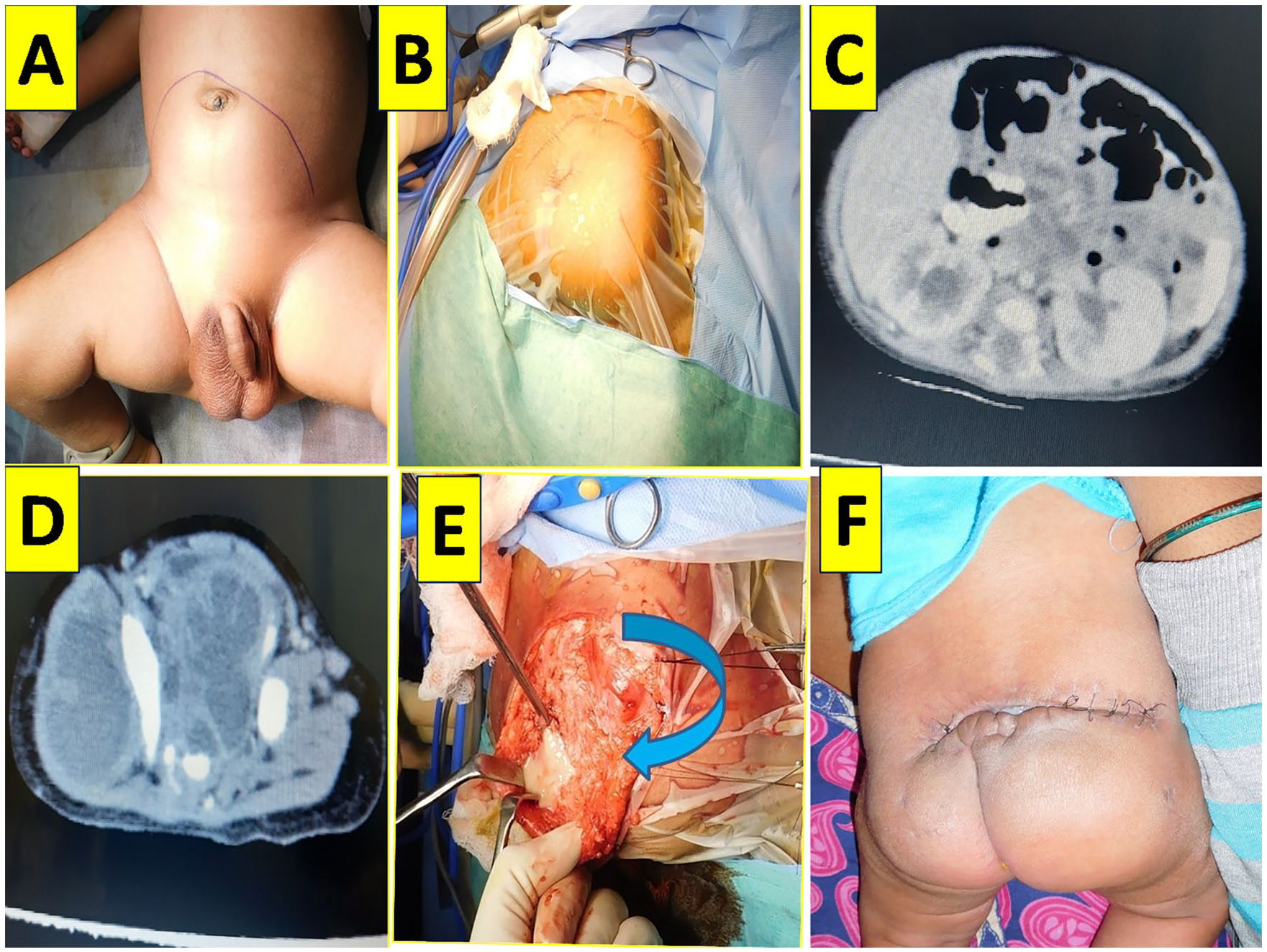
(A) Clinical image of mass per abdomen -marked line. (B) Clinical image of vague right gluteal mass in prone position. (C) Contrast enhanced computed tomographic image (CECT)-multicystic non enhancing per abdominal lesion causing bilateral hydroureteronephrosis. (D) CECT-image of multi cystic septated hypodense lesion occupying most of the pelvis, extending into the right gluteal region and posterior aspect of right thigh. (E) Intra operative picture showing thick purulent material in the right gluteal region and in thigh. (F) Post operative appearance.
Under general anaesthesia and in prone position first perineal component was exposed via inverted V incision (Figure 1B and C); thick pus of around 100 cc located between the planes of gluteal muscles was drained and wall of the cystic mass along with coccyx was also excised (Figure 1E). After giving thorough wash with normal saline, vacuum drain was kept and gluteal muscle reconstruction was done. The abdomen was explored via pfannensteil incision and similarly the varigated cystic mass and thick pus, which was adherent all vital structures like small bowel, bilateral ureters, and major vessels in the pelvis was excised and sent for histopathological evaluation (HPE). Post operatively baby developed perineal wound disruption and fecal fistula from gluteal wound which was managed conservatively (Figure 1F). Baby is now 2 year’s old and doing well.
Pathological Findings
HPE revealed it to be mature teratoma composed of mature adipose tissue, intestinal glands, skeletal as well as smooth muscle bundles in the background of mixed inflammatory cells in the fibro collage nous tissue. An island of neuroepithelial cells was also noted in the specimen (Figure 2A–C). Excised coccyx was normal (Figure 2D)

Histopathological images. (A) Low power view (10×)-showing intestinal glands. (B) Low power view-showing mature adipose tissue. (C) High power view—an island of neuro epitheleal tissue. (D) Low power view of coccygectomy specimen-mature hyaline cartilage.
Discussion
Sacrococcygeal teratomas have tissues derived from ectoderm, mesoderm, and endoderm. They are classified as benign (mature) and malignant or immature (composed of embryonic elements). Mature teratomas are common in neonates (68%) as well as in older children (73%). Immature teratomas are mostly cystic, whereas malignant tumours are solid.1,2
Mature and immature teratomas are considered as benign tumours. Immature teratomas have undifferentiated or poorly differentiated embryonic elements or tissue foci with primitive neuroectodermal tissues. SCTs that contain malignant elements such as yolk sac tumours, embryonal carcinomas and primitive neuro ectodermal tumours are considered to be malignant tumours. The grading system for SCTs: grade 0—¼ tumours contain only mature tissue; grade 1—¼ tumours contain rare foci of immature tissues; grade 2—¼ tumours contain moderate amounts of immature tissues; grade 3—¼ tumours contain large amounts of immature tissue with or without malignant yolk sac elements.1-3
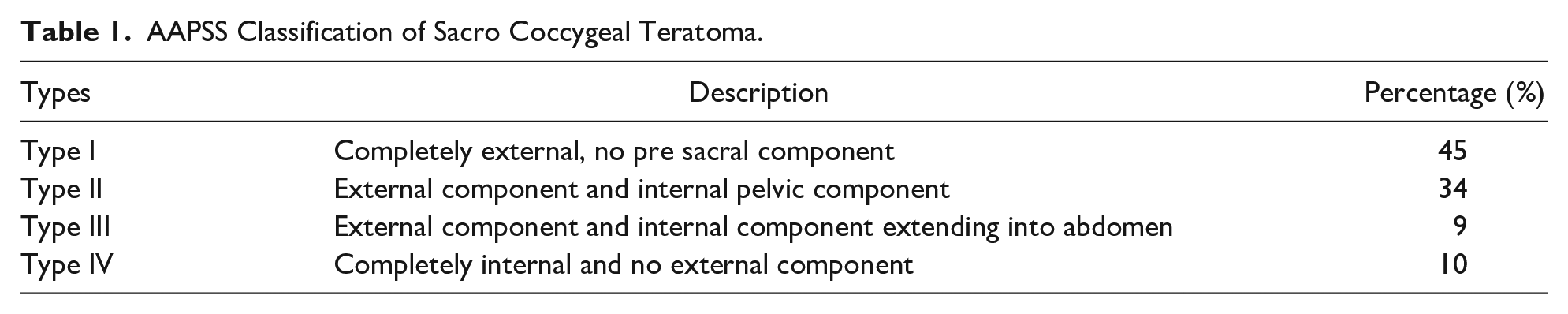
According to the American Academy of Pediatrics surgical section (AAPSS) classification (Table 1), SCTs are graded as : Type I (47%): Predominantly external tumour with minimal pre-sacral component; type II (35%): Present externally but with significant intra pelvic extension; type III (8%): Apparent externally but predominantly a pelvic mass extending into the abdomen, and type IV (10%): Pre-sacral with no external presentation. Our case belonged to SCT type III which was infected at presentation. As such types III SCT’s are rare in occurrence in neonates as well as in children.2,3
AAPSS Classification of Sacro Coccygeal Teratoma.
Failure to remove the coccyx results in 30–40% recurrence rate, with a higher probability of malignancy.2,3 The excised coccyx was histopathologically normal in this case (Figure 2D).
As there are no published reports of infected SCT in neonates as well as in children, only one case has been reported by Rattan et al in a 13-year-old child. 5
Hence author is reporting here, the first ever case of type III SCT containing predominantly cystic component having mature tissue elements (Figure 1A and B) with a foci of neuroepithelial tissue(Figure 2C) predominantly intra abdominal partly right gluteal region as a vague unremarkable swelling, which got infected due to routine intramuscular injection of vitamin K; its diagnostic and management challenges as well as its morbidity in a neonate.
High degree of suspicion as well as alertness amongst the health professionals especially in primary health centers before any injections or interventions on neonates can avoid morbidity and mortality.
Footnotes
Acknowledgements
The author would like to thank all her paediatric surgical colleagues and all the staffs of IGICH, Bangalore.
Author Note
*
Author Contribution
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.