
Abstract
Clinical practice guidelines for diagnosis and management of pediatric hypertension have been available for decades. Yet, most cases of hypertension in children are undiagnosed. Provider and system-based factors, such as the complexity of diagnostic standards, and a failure among physicians to recognize the importance of hypertension in children, play a role in underdiagnosis. It is unclear, however, how patient and family behaviors impact the diagnosis and treatment of pediatric hypertension. We aimed to explore the perspectives of parents whose children have had multiple high blood pressure readings or have been diagnosed with hypertension to inform clinicians with areas for practice improvement. In a 2 site qualitative study, we interviewed parents of 15 children diagnosed with hypertension. Results from semi-structured interviews with parents revealed barriers to the diagnosis of pediatric hypertension, including uncertainty about the diagnosis and concerns around the accuracy of blood pressure measurements. Delay in diagnosis and lack of child engagement emerged as obstacles to the treatment of pediatric hypertension.
Introduction
It has been 40 years since the National Heart Lung and Blood Institute (NHLBI) first issued clinical practice guidelines for hypertension in children and declared that “detection and management of hypertension in children and the precursors of hypertension in adults are the next frontiers.” 1 Since that time, pediatric hypertension has proven to be associated with serious consequences including left ventricular hypertrophy, increased carotid intima thickness, and microalbuminuria.2-4 Moreover, effective and safe treatments not only lower blood pressure but also reverse target organ damage. 4
Despite the longstanding availability of diagnostic criteria and clinical practice guidelines, most cases of hypertension in children and adolescents are unrecognized.5-8 Because no published studies have linked specific blood pressure levels in childhood with cardiovascular disease in adulthood, a diagnosis of hypertension is based on reference standards and defined as blood pressure averaging ≥95th percentile on 3 separate occasions, for a given age, sex, and height percentile.9,10 The complexity of the diagnostic standards9,10 and the need for multiple visits to make a diagnosis likely contribute to the under-diagnosis of the disease.5-8 In fact, national guidelines for the diagnosis of hypertension in children were somewhat simplified in the fall of 2017, in part to address this problem of under-diagnosis. Most cases of hypertension in children and adolescents are unrecognized.5-8
Little is known about pediatric hypertension from the perspective of patients and their parents. Because essential hypertension is an asymptomatic disease, and multiple visits are required to meet clinical criteria, patients and parents need to be fully aware and engaged in the problem in order to reach a diagnosis. Based on documented low rates of recognition and diagnosis, current practice is falling short of engaging patients and parents, and a deeper appreciation of parents’ experience, understanding, and knowledge of pediatric hypertension is needed to make meaningful changes in care delivery and treatment. In this study, our aim was to explore the perspectives of parents whose children have been diagnosed with hypertension or have had multiple high blood pressure readings. We hypothesized that lack of understanding of hypertension, challenging diagnostic and follow up process, and competing priorities at medical visits may contribute to parents’ and children’s care experiences and adherence to clinician recommendations.
Methods
Setting and Recruitment
The study took place in 2 locations: Kaiser Permanente Colorado (KPCO), located in Denver, Colorado, and University Hospitals-Rainbow Babies and Children’s (UH-RBC) and its affiliated primary care network; Rainbow Primary Care Institute (RPCI), in Cleveland, Ohio. The RPCI cares for roughly 137 000 children annually across northeast Ohio. KPCO is an integrated health care system that provides health insurance and care to approximately 127 000 children and adolescents in Colorado. Outpatient care at KPCO is provided at 27 primary care facilities, and KPCO offers traditional health maintenance, deductible, and Medicaid plans.
Parents were eligible for the study if their children were between ages 3 through 17 years, enrolled with KPCO or with UH-RBC in 2018, and had an ICD-10 coded diagnosis of elevated blood pressure or hypertension. We excluded non-English speaking subjects and children with known secondary causes of hypertension. We utilized the National Patient-Centered Clinical Research Network (PCORnet) Common Data Model (CDM) to identify eligible subjects. PCORnet is funded and supported by the Patient-Centered Outcomes Research Institute (PCORI) to enable patient-centered clinical research to be conducted efficiently. Through a query of the PCORnet CDM and a similar electronic data repository at UH-RBC, we identified potentially eligible children through a combination of searches of the structured problem list and encounter diagnosis fields. Based in the inclusion and exclusion criteria, we used convenience sampling strategy to recruit subjects until saturation of themes was reached.
Recruitment took place from November 2018 through February 2019 [in Colorado] and from January 2019 through April 2019 [in Ohio]. Eligible subjects were sent a recruitment letter via mail or email describing the study and were told to expect a phone call to gauge their interest, provide more details and offer participation. Enclosed within the letter or email was a phone number or email address a parent could call or send a message to decline participation should they choose to do so immediately.
Interview Guide
To collect an open-ended data on parents’ thoughts, feelings and beliefs around pediatric hypertension, we crafted an interview protocol. The guide consists of flexible dialogue between the researcher and study participants supplemented by probes and follows up questions. The semi-structured phone interview guide was first drafted by the principal study investigator and then disseminated to the research team to provide feedback.
The research team was composed of core co-investigators and research staff. The final and agreed-upon version of the phone call script included a description and purpose of the study, benefits and risks of participation, privacy and confidentiality assurance, and verbal informed consent to participate in an audio-recorded phone interview. The semi-structured interview guide covered 4 content areas: the experience of diagnosis of pediatric hypertension, attitudes and beliefs about diagnosis and treatment, treatment experience, and changes to lifestyle made as a result of the diagnosis. Each content area included 2 to 7 open-ended question prompts to ensure sufficient information on each area was collected from participants (Table 1).
Question Prompts From Semi-Structured Interview Guide.

Telephone Interview Methods
The phone interview was conducted by research staff. Up to 3 call attempts were made. To accommodate parents’ schedules, research staff offered to call back at a more convenient time if necessary. KPCO offered a $25 gift card incentive for participation, and UH-RBC did not offer any monetary incentive for participating in the study. Prior to obtaining verbal consent, each participant was asked to teach-back what they understood about the study and given the opportunity to ask questions or raise concerns. Each interview lasted between 10 and 30 minutes (average 17 minutes) and was audio-recorded and transcribed.
Analysis
The transcripts of the recorded phone interviews were independently reviewed and coded by 2 researchers using ATLAS.ti 11 (at KPCO) and NVivo 12 (at UH-RBC) software. The researchers used a strategy based on the Grounded Theory, 13 a systematic approach that involves construction of theories through methodological gathering and analysis of data, to code transcripts and held regular meetings to discuss observations, resolve discrepancies, and ultimately agree upon emerging themes through consensus. These themes were shared and discussed with the research team.
Ethical Approval and Informed Consent
The study was approved by the Institutional Review Board (IRB) of Kaiser Permanente Colorado (Reference number 1285199) and University Hospitals of Cleveland (Reference number 20181137). Informed consent was obtained verbally and audio-recorded before participation.
Results
At both study sites, 314 were identified as potentially eligible subjects (167 at KPCO and 147 at UH-RBC). Based on chart review, we excluded 81 individuals who were considered ineligible. Eligible parents received an invitation to participate. Nineteen individuals declined to participate. A total of 15 parents did consent to participate and completed a phone interview (10 in Colorado and 5 in Ohio). Children of the parents who participated in the survey were between the ages of 9 and 17 years, including 5 females.
Most parents did know that their child either had high blood pressure readings (n = 3) or diagnosed with hypertension (n = 6). However, some parents felt uncertain whether their child has a diagnosis of hypertension, which was especially frustrating after multiple diagnostic and follow up visits. Parents were informed of elevated blood pressures at child well visits (n = 7) and sick visits (n = 6). A Well Child Care (WCC) visit is when a child visits their healthcare provider at a regular interval from infancy to adolescence to receive preventive care, health screening and counseling. On the other hand, a sick visit is when a child visits their healthcare provider to address an acute health-related issue.
In this qualitative study, we identified 4 main themes that emerged from the interview responses. These included: (a) attitudes and concerns about high blood pressure and hypertension in children; (b) barriers to diagnosis of pediatric hypertension; (c) barriers to treatment of pediatric hypertension; and (d) challenges with child engagement and lifestyle changes.
Attitudes and Concerns About High Blood Pressure and Hypertension in Children
All parents said that they had a family history of high blood pressure, except one whose child was adopted. Parents believed that high blood pressure is important to monitor and treat and that it can affect the heart and other body organs (Table 2). There were different opinions and knowledge as to how high blood pressure affects children. Five of the parents understood that weight could play a role in high blood pressure, while others thought that high blood pressure was caused by anxiety or did not know the cause. Three parents believed high blood pressure readings in the office were “because of nerves,” and hence did not believe such values reflected their child’s habitual blood pressure (Table 2). One parent voiced that, despite receiving a diagnosis of hypertension, they were confused about the actual reason behind it and were worried whether other family members are at risk.
“. . .the only thing that I just wished or hope that we get to a point where we figure out where this is coming from or if it is genetics, [. . .] the education from that point of view, for other siblings [. . .] knowing how to deal with that or to monitor it.” (Participant 21629)
Parent Quotes Related to Attitudes and Concerns About High Blood Pressure and Hypertension in Children.

Barriers to the Diagnosis of Pediatric Hypertension
A third (n = 5) of the parents we spoke with expressed uncertainty about the diagnosis. They discussed that their child had elevated blood pressures, but that they had not received a diagnosis of hypertension from their pediatrician. Having conflicting blood pressure readings can cast doubt on whether to trust the diagnosis and make the recommended changes to lower blood pressure. Even with ambulatory 24-hour blood pressure monitoring, a parent expressed her frustration and dissatisfaction (Table 3). Children with ongoing medical or mental health conditions face additional challenges, especially if they have already been on other medications or may require additional testing for the diagnosis of hypertension (Table 3). Three parents indicated that they did not know how and why their child was diagnosed with hypertension. One parent mentioned that they had not made an appointment to talk about elevated blood pressures because “the doctor was too busy,” and they were not given the chance to have a focused visit to discuss their child’s blood pressure. Another parent suggested that clinicians be mindful and consider the psychosocial aspects when addressing high blood pressure with the child and their family (Table 3).
Parent Quotes Related to Barriers to the Diagnosis of Pediatric Hypertension.

Barriers to Treatment of Pediatric Hypertension
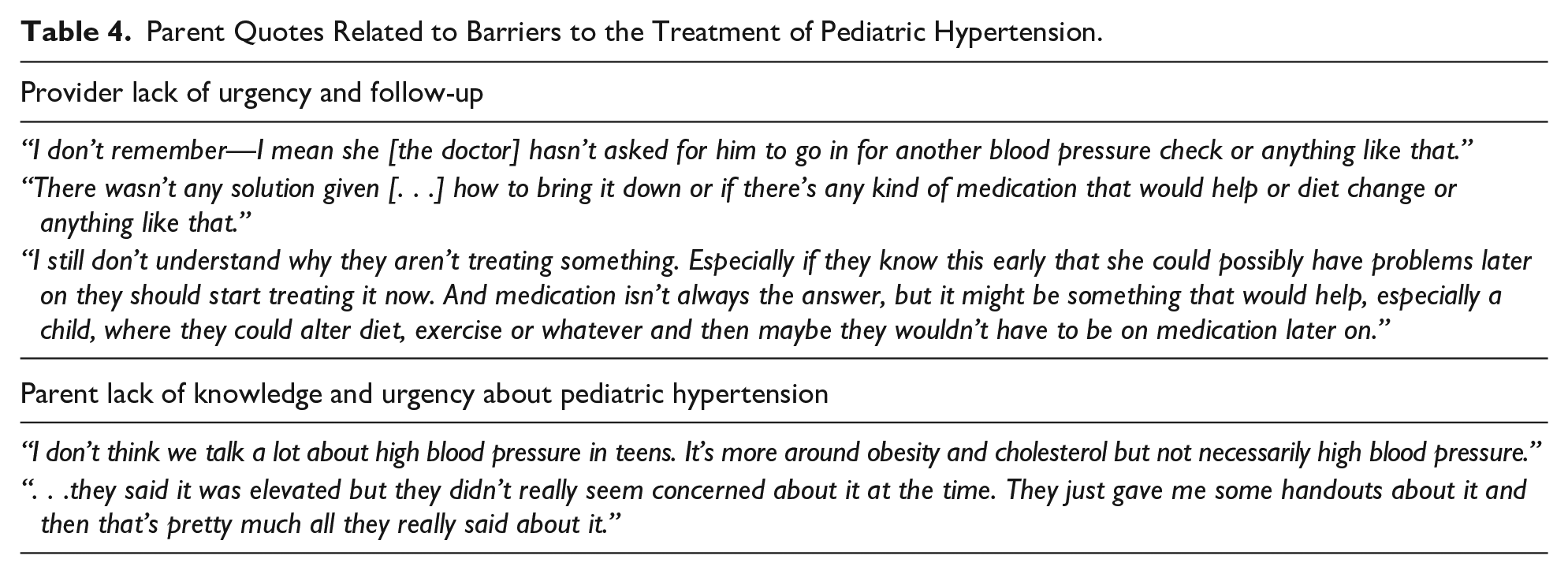
Parents reported that even though blood pressures were elevated, they were not asked to return for follow-up BP checks or given clear advice on what to do next. Parents were also frustrated that the provider did not provide recommendations on how to treat elevated blood pressure to prevent lifelong complications (Table 4). Parents did feel that high blood pressure is a problem for their children but did not know enough about why it is important or did not think of it as an urgent issue. Some parents did not seem to believe that hypertension needs close monitoring and treatment based on their impression of the way that the provider discussed the high blood pressure readings (Table 4).
Parent Quotes Related to Barriers to the Treatment of Pediatric Hypertension.
Challenges With Child Engagement and Lifestyle Changes
Parents voiced frustrations in getting their teenagers to see the importance of controlling high blood pressure and wanted the doctor to have more influence on their child to help them better understand their condition and make healthy lifestyle choices. Other parents described competing family priorities with the follow-up requested for blood pressure checks and dealing with other stressors such as bullying at school (Table 5).
Parent Quotes Related to Challenges with Child Engagement and Lifestyle Changes.

Discussion
Review Key Findings
The findings from these interviews highlight that parents of children with high blood pressure and hypertension acknowledge the importance of diagnosing and treating pediatric hypertension. Although most parents were uncertain why their child had elevated blood pressure, some of them expressed understanding that modifiable lifestyle factors, such as for overweight, obesity, stress and anxiety, may play a role. One-third of parents expressed uncertainty about the diagnostic process, including whether their child had the condition or not. Blood pressure measurements, which varied considerably from a visit to visit, multiple follow-up visits with the child’s pediatrician, seeing one or more specialists, and the use of multiple diagnostic strategies were mentioned as barriers to timely diagnosis of hypertension.
Even after the diagnosis had been established, some parents voiced that it was not communicated clearly with them, and they felt confused about why their child had elevated blood pressure and how to manage it besides simply taking medication. Some parents felt discussions of blood pressure were too short or “rushed” and suggested dedicating a visit to educate them further about pediatric hypertension; specifically, the causes and lifestyle interventions. This was particularly important to parents as it would give them agency in helping their children better manage and support their children’s health. While some parents acknowledged receiving clear recommendations for lifestyle interventions, such as healthier diet, exercise, and weight loss, they did express their struggle motivating their children to make the changes necessary and understand the importance of controlling their blood pressure. Parents raised the need for PCPs to directly communicate with children with elevated blood pressure or hypertension and engage them in understanding their health condition more, as well as encouraging them to make healthier lifestyle choices.
Consistency With What Is Already Known
Our findings are consistent with prior work based on clinician and system factors that describe barriers to identifying elevated BP and diagnosing hypertension in children.5,7 Providers have previously expressed concerns related to BP measurement, including system and individual factors, 14 some of which have also been shared by parents in this study as well. The concerns involve the perceived inaccuracy of office-based blood pressure measurements as well as inconsistent ambulatory and home blood pressure monitoring. These observations corroborate the findings of previous studies,15-17 and emphasize the need to address the variability of blood pressure measurement and monitoring in children.
Implications for Current Practice
Improving Clinician’s Knowledge and Communication
Parents, even those whose children have received a diagnosis, may be confused about the diagnosis simply because clinicians are confused about the diagnosis.5,14,18,19 Medical providers need to engage parents and children in the diagnostic process better. For example, parents could be informed that BP values can vary a lot, which is why an average across 3 appointments is needed. The 2017 American Academy of Pediatrics (AAP) guidelines 20 highlights the importance of accurate and reliable blood pressure measurement in the diagnosis and monitoring of blood pressure in children. Measuring a child’s blood pressure can particularly be challenging because of masked hypertension (MH) or white-coat hypertension (WCH), leading to under- or over-diagnosis of hypertension in children. 20
Reducing Barriers to Diagnosis
One of the barriers that emerged during the semi-structured interviews was the uncertainty in blood pressure measurement, leading to parents’ frustration and, most importantly, delay in the diagnosis of hypertension. While office blood pressure measurement is the current standard of care, 20 there is considerable evidence to support ambulatory blood pressure monitoring (ABPM) and home blood pressure monitoring (HBPM). 21 However, utilization of the latter methods is still limited due to cost, limited normative reference ranges, and the need for provider training. 22 There is a demand for standardized use of ABPM and HBPM as well as clinical decision support systems to help clinicians make an accurate and timely diagnosis of pediatric hypertension.
Reducing Barriers to Treatment
Medical providers need to be familiar with the clinical practice guidelines so they can comfortably guide the children and their parents. It is essential to educate parents and involve them in decision-making throughout the journey. This is especially important for children with modifiable risk factors where lifestyle changes are likely to impact the management of their elevated blood pressure. Furthermore, multidisciplinary approaches to minimize the number of appointments and maximize the yield of the office visit would help parents and their children better understand the plan of care and enhance their compliance with the clinical recommendations.
Child Engagement and Lifestyle Changes
Child engagement is poor, as cited by a few parents. Children and adolescents may not appreciate the importance of their health issues, and so may not adhere to recommended lifestyle changes and medical treatment. One strategy to address this is for parents to serve as role models.23-25 Besides, clinicians should involve the child in the discussion during the visit and engage them in the plan of care.
Limitations
Our study has several limitations. Given the qualitative nature of this work, the relatively small sample size and the convenience sampling strategy, we do not know how prevalent these views are in the broader population. We also do not know if these views would be common among patients seen by different providers in different health care settings. We did find recurring themes after 15 interviews. It is possible however, that a larger sample may have revealed additional insights. The monetary incentive offered to Colorado participants may explain the higher participation rate, compared to the Ohio participants. The majority of parents interviewed had adolescents with hypertension, and it’s unclear how the experience of diagnosis may have differed with younger children.
Conclusion
This study offers key insights into the barriers to diagnosis and management of pediatric hypertension, from the parents’ point of view. Barriers to diagnosis include concerns around the accuracy and consistency of blood pressure measurements and uncertainty about the diagnosis itself. Barriers to treatment include delay in diagnosis and struggle following clinical recommendations. Child engagement emerged as a major challenge as well as an opportunity for clinicians to have more influence on children and support parents through empowerment.
Footnotes
Acknowledgements
KPC: Ruth Bedoy for patient recruitment and conducting many of the interviews, as well as contributing to the analysis and interpretation of the results. UH-RBC: Greta Lazzara for conducting the phone interviews. Sue Able for patient recruitment and help in data collection.
Authors’ Note
Assim M AlAbdulKader is also affiliated with Department of Family and Community Medicine, College of Medicine, Imam Abdulrahman bin Faisal University.
Author Contributions
AMA, MFD, and GR contributed to the study conception and design. All authors have contributed to data acquisition, analysis, and interpretation. AMA and EFM drafted the manuscript. All authors critically appraised the manuscript and gave the final approval.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Patient-Centered Outcomes Research Institute (PCORI) as part of the Patient Outcomes Research to Advance Learning (PORTAL) project (PCORI CDRN 1306-04681).