
Abstract
Background. Pre-school children are at a higher risk to acquire infectious diseases such as hand, foot and mouth disease due to their immature immune system. Good hand hygiene prevents transmission of infectious diseases. This study aimed to determine the knowledge and practices of hand hygiene among pre-schoolers. Methods. In this prospective, multi-center study, the pre-schools were selected according to the selection criteria. A questionnaire consisting of socio-demographics, knowledge and practices of hand hygiene were administered via face-to-face interview during the pre- and post-intervention period. A total of 435 pre-schoolers aged 5 and 6 years old from 2 pre-schools within Klang Valley, School P (test group) and School C (control group) were involved in this study. The test group was provided with comprehensive hand hygiene education including video on proper handwashing technique during the 2 months intervention period, whereas the control group did not receive any form of intervention. The data were statistically analyzed using descriptive analysis and independent t-test. Results. Majority of pre-schoolers gained knowledge of handwashing from their parents. However, only 63% demonstrated good handwashing technique. Test group were significantly better (P < 0.05) in handwashing technique and hand hygiene routine score. Conclusion. A comprehensive hand hygiene education program should include proper handwashing facilities, resources, and awareness of the care-givers in instilling and sustaining good hand hygiene behavior.
Introduction
Young children are more susceptible to infectious diseases such as respiratory tract infections, hand, foot and mouth disease (HFMD), gastroenteritis, and many more due to the naivety of their immune system and comprehension of personal hygiene. 1 These diseases often are transmitted via droplets, aerosol, and faeco-oral route.2,3 Contact with nasal discharge, saliva, faeces, urine, and blisters require vigilant transmission precaution. 4
In Malaysia, most parents send their children to pre-school as a preparation for their children before primary education. Generally, pre-schools are a closed environment with numerous inanimate objects serving as vehicles of infection transmission. There are often inadequate and inappropriate handwashing facilities thus predisposing the children to the spread of infectious diseases. 5 Children attending childcare centers have an increased risk of acquiring respiratory infections, acute otitis media, diarrhoeal disease, invasive bacterial disease, HFMD, and varicella. 6 Department of Statistics, Malaysia reported that the number of young children enrolled into pre-schools increased by 1.2% from 2014 to 2015. 7 Eventually, the resultant overcrowding of children in pre-schools will too increase the risk of communicable disease transmission in the Malaysian community. 8
Young children may not possess the ability to implement their own personal hygiene and comprehend the importance of proper hygiene, and hence, diligent care and supervision is required by caregivers. Whereby, the integration of appropriate hygiene, nutrition, and administration of vaccines (age-dependent) to provide a basis for healthy age-appropriate growth, development and immune response needs to be highlighted. Hand hygiene is one of the most important elements of infection control that has been proven to significantly reduce the risk of cross-transmission of infections in healthcare facilities.9-11 Not only that, previous studies also suggested that infectious diseases could be prevented with proper hand hygiene practice at home and at school.12-16 Therefore, increasing the awareness and knowledge of the community on the importance of basic hand hygiene in disease prevention is vital.
In the past year, there are increased and recurrent HFMD epidemics occurring worldwide. It was reported that decrease in the population immunity and increase in number of children were the factors influencing prevalence of young children toward HFMD epidemic.17-19 In 1997, the first HFMD epidemic within Malaysia was identified in Sarawak where 2600 children were infected and 48 died.20-22 In 2018, there was a surge in the incidence of HFMD in Peninsular Malaysia. As of 26 May 2018, 21 644 cases have been reported in comparison to 19 398 in the previous year. A total of 316 pre-school, nurseries and daycares have reported incidence of HFMD among their attendees, amounting to 52% of the outbreak. 23 Hence, in order to reduce the incidence of absenteeism among pre-school children due to HFMD, they were highly encouraged to practice proper hand hygiene as it was proven to be able to prevent infectious diseases and to be cost-effective.24-26
Assessments regarding hand hygiene in Malaysia concentrates more on high risk groups such as food handlers.27-30 To our knowledge, data pertaining hand hygiene compliance in Malaysian pre-school children is still scanty. Hence, this study aimed to assess hand hygiene practices among pre-school children in Klang Valley. The data collected may serve as a baseline to provide a platform to improve awareness and compliance on the importance of proper hand hygiene.
Methods
Study Population
This study focused on the population in the Klang Valley area. The actual calculated sample size was 254 (Confidence interval of 99%, power of study 95%) with taking into consideration a non-response rate of 0.20. Two pre-schools, School P (test group) and School C (control group) were managed by the Majlis Agama Islam Wilayah Persekutuan (MAIWP), a government agency, were selected according to the selection criteria; that is, number of students, infrastructure and logistics requirements. The pre-schools had to have proper and functioning water-taps for hand-washing. Parents were provided with subject information sheet together with consent form which consisted of study importance, background, risks and objectives. The study excluded children allergic to povidone iodine-based products, with thyroid disorders and no parental consent.
Data Collection
A previously validated questionnaire 31 (Bacterfree) was improvised based on suitability for this study. The questionnaire was divided into 3 sections, that is, demographic, handwashing knowledge, and hand hygiene practices. In the first section, their demographic details consisted of gender, race and age were obtained. Knowledge of handwashing was identified in the second section, whereby they were questioned on who taught them hand washing. In this section, the participants could answer more than one based on the options stated in the questionnaire. The last section was to assess the children’s current handwashing technique and hand hygiene routine. They were interviewed on their hand hygiene routine whether they perform handwashing during the 5 crucial times; namely after toilet, before and after meals, after playing outdoors, after coughing and sneezing and after playing with pets. The hand hygiene routine times were presented in images and simple scenarios to ease the children to choose and describe their answers during the interview. Each correct response was given a score of 1 with the maximum score of 5. The methods of performing these hand hygiene routines during the 5 crucial times were not specified during the interview but it was described as hand washing in general. Subsequently, the interviewers observed the students’ handwashing technique based on the steps recommended by World Health Organization (WHO). We outlined 11 hand washing steps which are; wetting hands thoroughly under running water, using soap on the hands, rubbing hands palm to palm, rubbing hands with fingers interlaced, rubbing one palm over the back of the other hand, cleaning the back of fingers to opposing palms, rotational rubbing of the thumbs, fingertips and wrists, rinsing hands with water thoroughly and finally drying hands. Materials such as soap, tissues, and dustbins were provided. Similarly, for every step performed, the child was given a score of 1 with a maximum score of 11. No educational material and lectures were given prior to the interview sessions. Absenteeism and health conditions were also recorded as supportive data.
Statistical Analysis
Questionnaires were collected, and the data were statistically analyzed using Statistical Package for the Social Sciences (SPSS) software Version 20; IBM Corp., Armonk, NY, USA for Windows. Descriptive analysis was performed for demographic information of samples. Gender, age, and school-based comparisons were analyzed using independent t-test. The level of significance was set at P < 0.05.
Ethical Approval and Informed Consent
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional research committee (Human Medical Research and Ethics Committee of Universiti Sains Islam Malaysia, USIM/JKEP/2017-20) and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards. This article does not contain any studies with animals performed by any of the authors. Informed consent was obtained from all the parents of the individual participants included in the study.
Results
Data was collected from 435 students from 2 pre-schools, School P (test group) and School C (control goup).
Demographics
The demographics such as gender, age and pre-schools for each child were identified. There were a total of 276 children from School P and 159 children from School C were involved in this study. Out of all the participants, there were 221 boys and 214 girls. With regards to age, the students were all 5 years (47.4%, n = 206) and 6 years (52.6%, 229) of age.
Knowledge
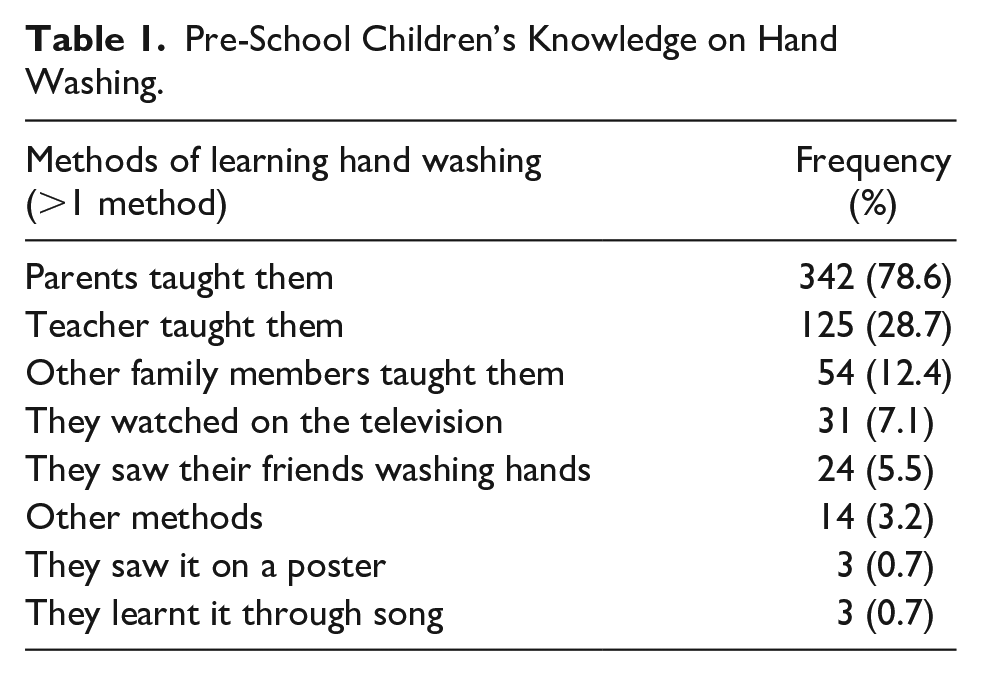
In the next section, their background knowledge of hand hygiene was assessed specifically on their methods of learning handwashing as listed in Table 1. Majority of the children claimed that their background knowledge on handwashing can be attributed to their parents. The next biggest contribution of handwashing knowledge on the children is their teachers (28.7%). Out of the total, 54 students said that they were also taught by other family members including siblings and grandparents. About 5.5% of them said they learnt from watching friends wash their hands. Not only that, 7.1% of the students also claimed that they learnt handwashing by watching the television followed with 3.2% of them said that they learnt handwashing by themselves which was categorized as other methods. A small number of them said they learnt from a hand hygiene poster (0.7%, n = 3) or through songs (0.7%, n = 3).
Pre-School Children’s Knowledge on Hand Washing.
Practice
Hand hygiene routine
In the first part of this section, the children were also assessed on their current hand hygiene routine daily (Table 2). Out of the 5 crucial times for handwashing, it was mostly performed before and after meals and after they go to the toilet. Out of the total, less than half washed their hands after playing outdoor. Handwashing was least performed after playing with pets and after coughing and sneezing. The mean score of the children’s hand hygiene routine is 2.89 ± 1.674.
Current Hand Hygiene Routine Among Pre-School Children.

Handwashing technique
Table 3 illustrates the descriptive statistics of the pre-school children’s handwashing technique. The most performed steps in handwashing are wetting the hands under running water, followed by rubbing hands palm to palm and rubbing hands palm to palm with fingers interlaced (53.8%, n = 234). The 3 most commonly missed steps are the rotational rubbing of the thumbs, rotational rubbing of both wrists and rotational rubbing of the fingertips on palm. Interestingly, it was observed that only 52.6% (n = 229) of them use soap when washing their hands. Almost half of them did not rinse their hands thoroughly with water. Furthermore, only a third dries their hands after handwashing even when they were provided with tissues and a dustbin. The mean score of handwashing technique is 4.20 ± 1.845. The score obtained by each of the students were then compared to the mean score calculated. Those who scored higher than the mean was categorized as having good practice of hand hygiene whereas those who scored lower than the mean was categorized as having poor practice of hand hygiene. Overall, out of 435 children, only 275 (63.2%) of them had good practice of hand hygiene.
Observation on Pre-School Children’s Handwashing Technique.

Comparison of hand hygiene practices
The children’s hand hygiene practices were then compared according to the gender, age and pre-schools as shown in Table 4. Females scored higher than males in handwashing technique. However, the score was similar for hand hygiene routine. It was revealed that students of School P attained higher scores of handwashing technique and hand hygiene routine compared to School C. Hence being female and attending school P were significant attributes for higher handwashing technique score. For hand hygiene routine, attending school P was the only significant attribute. Even though, 6 years old performed slightly better in handwashing technique and hand hygiene routine, age was not statistically significant.
Gender, Age and School-Based Comparisons of Hand Hygiene Practices.
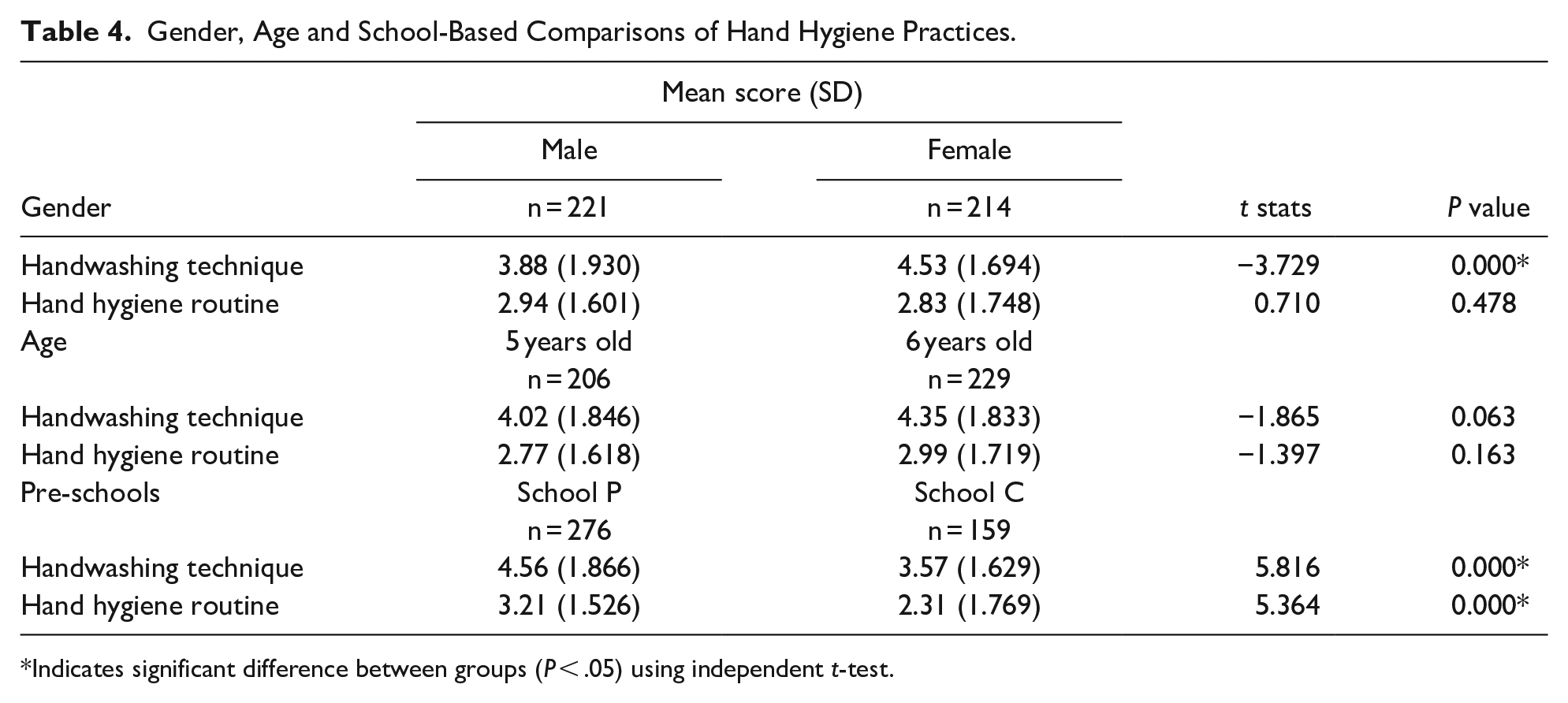
Indicates significant difference between groups (P < .05) using independent t-test.
Discussion
Adequate knowledge on hand hygiene has proved to yield positive hygiene behavior.32,33 Present study showed that parents are the greatest influence in teaching the children handwashing (Table 1). This result supports a previous study by Mohamed et al 31 who found that most parents agreed that they should teach their children how to wash hands properly and that children’s hands should always be kept clean. Furthermore, it was also observed that parents generally have a good understanding on the importance of hand hygiene and demonstrated good attitude toward hand hygiene. 31 Aside from that, similar to previous studies, we found that teachers also play an important role in educating children on handwashing and showing good example toward them.34,35 This is relevant as apart from parents, children spend most of their time at school with their teachers. Rosen et al 35 in their study found that teachers do agree that handwashing aids in disease control and they demonstrated positive attitude toward handwashing. 35 In this study, the children also stated that they learned handwashing from other family members including siblings and grandparents. Only a small percentage of them gained handwashing education from watching the television, reading hand hygiene posters or through songs. These methods are considered passive tools of education. Children would be more enthused with action-oriented lessons which will increase their ownership of the new knowledge. 36
Besides that, the children were also observed and scored on their current handwashing technique. The children’s handwashing performance might be influenced by the presence of interviewers since they were being closely monitored. Out of 11 handwashing steps outlined, the mean score of handwashing technique was found to be only 4.20. We found that the most commonly performed handwashing steps are wetting hands thoroughly under running water, rubbing hands palm to palm and rubbing their hands with fingers interlaced. Most of them skipped rotational rubbing of the thumbs, fingertips, and wrists. Not only that, it was found that only a small percentage of them clean the back of their hands to opposing palms with fingers interlocked. This conforms with the most areas missed whilst handwashing even for healthcare workers. 37
Handwashing with soap has been shown to remove bacteria more effectively compared to handwashing with water alone. 38 This is because soap contains surfactants that dislodge microorganisms from the skin. Subsequently, the soap should be rinsed away under running water, to minimize skin irritation and prevent recontamination, respectively. 39 However, our study found that only half of the children use soap and less than half of them rinsed their hands thoroughly after using soap . Lastly, it was observed that, even we provided them with tissues and a dustbin; only 35.4% of them would dry their hands with the tissues provided after hand washing. This step is crucial as the friction caused by rubbing will remove the pathogens and the moisture. 40 Deficiency of practice might be because these children were unfamiliar with the hand hygiene materials and its use due to limited hand hygiene resources that were provided by the schools.
In this study, it is revealed that out of the 5 crucial times for hand washing, it was mostly performed before and after meals and after toilet. This reflects their basic practices as most parents and teachers would have taught them to do so. Less than half of them have a habit of washing their hands after playing outdoors. This is because most of them answered that they preferred to play indoors due to logistics and safety factors. Hence, most of them did not wash their hands after playing indoors. The unaccustomedness of playing outside might have contributed to their answer which they have stated that they would not wash their hands if they were to play outdoors. Similarly, handwashing was also less commonly performed after playing with pets since most of them do not own pets at home. Lastly, the least performed handwashing time was after coughing and sneezing. They were nonchalant to this, as coughing and sneezing might be deemed as ordinary behavior that does not pose any risk to them. It is very crucial to encourage them to practice the right cough etiquette because coughing and sneezing are well-known to be as one of the modes of transfer of germs from an infected person to another person. These findings highlight the knowledge gaps in the pre-school children that can be addressed by teaching them the importance of proper handwashing technique and hand hygiene routine. These results are in congruent with previous studies that suggest that the children have to be frequently reminded on their basic hand hygiene routines.33,41 This is where the care-giver, that is, parents, teachers, extended family members and peers can encourage each other to perform proper hand hygiene.
Present study also revealed that girls scored higher than boys in handwashing technique. This result is in agreement with a previous study which described that girls were easily motivated to practice better handwashing as compared to boys. 34 It was also found that there is no difference in hand hygiene practices between 5-year olds and 6-year olds. However, when compared between schools, it was observed that students of pre-school P attained higher scores of handwashing technique and routine compared to pre-school C. Based on our observation, pre-school P were provided with soap and had adequate number of height-appropriate sinks at the toilet for the students. In contrast, the students of pre-school C were not provided with the same facilities, whereby the school was not equipped with proper sink and soap. Since, the pre-school building were within the compound of a mosque, hence, they also had to share the toilet facilities with the public who visited the mosque. They also have very limited number of sinks and were only equipped with few pipes connecting water directly from the water tank. This might have strongly influenced on the children’s hand hygiene practices at school. Several studies have proven the importance of adequate hand hygiene facilities and materials in encouraging children to have proper hand hygiene practices.32,42 Apart from lack of infrastructure and resources, other studies reported that poor hand hygiene compliance among school children were due to time constraints 33 and inadequate awareness and knowledge. 42 Administration of schools and parents may allocate certain amount of budget to enhance the hand hygiene facilities and promote good hand hygiene behavior.
This study managed to demonstrate differences in the current hand hygiene knowledge and practices among the pre-school children from 2 different school in different environment and facilities. We also managed to get larger number of participants even after excluding several participants from each of the pre-school since this study was conducted in 2 of the MAIWP’s pre-school with the highest number of children as compared to the other pre-schools. This is because the rest of the MAIWP’s pre-schools could only cater for a smaller number of children due to the logistics and demands. Therefore, we were able to collect varieties of responses from the young respondents. However, this study also had few limitations such as having unable to verify and validate on the self-reported hand hygiene routines as the score were given based on what was being answered by the children. Besides, different interviewers may have different style of conducting the interview session depending on whether they managed to get the children to response on every of the questions asked. Besides, there are also few special needs children participated in the interview session which might require different approach in interviewing them. It would be better if the interviewers had experience in dealing with these special children. However, throughout the interview session, none of the participants had an issue in answering each sections of the questionnaire and they were able to follow the instructions given by the interviewers since the session was also being monitored by their homeroom teachers.
Conclusion
In conclusion, it was observed that parents and teachers play an important role in educating children to perform hand hygiene; girls demonstrated better handwashing technique as compared to boys and adequate hand hygiene facilities has an influence on the children hand hygiene practices. Age was not a factor in adhering to proper handwashing technique or hand hygiene routine. In the future, proper hand hygiene education and training programs such as workshops and forums focusing on hand hygiene technique and practices should encompass the care-giver roles in instilling and encouraging good behavior among the children. A comprehensive hand hygiene education program should include parents and teachers in the pre-schools’ education syllabus to inculcate positive hand hygiene. Hence, by having good handwashing knowledge, proper facilities, resources and maintenance could strongly enhance the sustainability of positive hand hygiene behavior among pre-school children.
Footnotes
Acknowledgements
The authors would like to thank Majlis Agama Islam Wilayah Persekutuan (MAIWP) for granting permission and giving full cooperation for us to perform this study at the pre-schools under their management. We are very grateful to the representatives from Universiti Putra Malaysia for agreeing to collaborate on this study.
Author Contributions
All authors contributed equally to this paper.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by Mundipharma Pharmaceutical Sdn. Bhd (Grant number: USIM/MUNDI/FPSK/052002/42817).
Ethical Approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional research committee (Human Medical Research and Ethics Committee of Universiti Sains Islam Malaysia, USIM/JKEP/2017-20) and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards. This article does not contain any studies with animals performed by any of the authors.
Informed Consent
Informed consent was obtained from all the individual participants included in the study.
Data Availability
Data in the study can be made available upon request from the corresponding author. Corresponding author had full access to all the data in the study and had final responsibility for the decision to submit for publication.