
Abstract

Introduction
Pulmonary vein stenosis (PVS) in pediatric patients can be a rapidly progressive disease. Mortality rate increases with the number of pulmonary veins involved. 1 Surgical repair of total anomalous pulmonary venous return (TAPVR) is associated with a 6% to 8% restenosis rate and an associated mortality of 2% to 18%. 2 The pathological finding in PVS appears to involve intimal increase of myofibroblast numbers. Use of various drugs to inhibit myofibroblastic growth have shown mixed results.3,4 Our collaborative group recently described the presence of “metakaryotic” stem cells in both primary and secondary forms of PVS including TAPVR. 4 These stem cells appear to create myofibroblasts by asymmetric amitotic division as observed in human organogenesis and carcinogenesis. 4 Metakaryotic cells in vitro and in vivo are constitutively resistant to x-rays and most chemotherapeutic drugs. They are, however, killed by widely used drugs such as metformin, verapamil, NSAIDS and antibiotics after several weeks exposure in vitro. 5 In this case series we describe 2 infants who developed restenosis after TAPVR repair that we tried metformin for compassionate use to slow PVS progression and discuss possible implications for future study.
Ethics Approval and Informed Consent
The following case series was approved by the Children’s Hospital of Wisconsin Institutional Review Board 2 (#1346655-3) with a consent waiver and certification for use of personal health information in decedents due to its retrospective nature and use of deceased individuals.
Case Series
The first patient was born full term and noted to be cyanotic with mixed TAPVR to the right atrium (Table 1).
Patient Features.
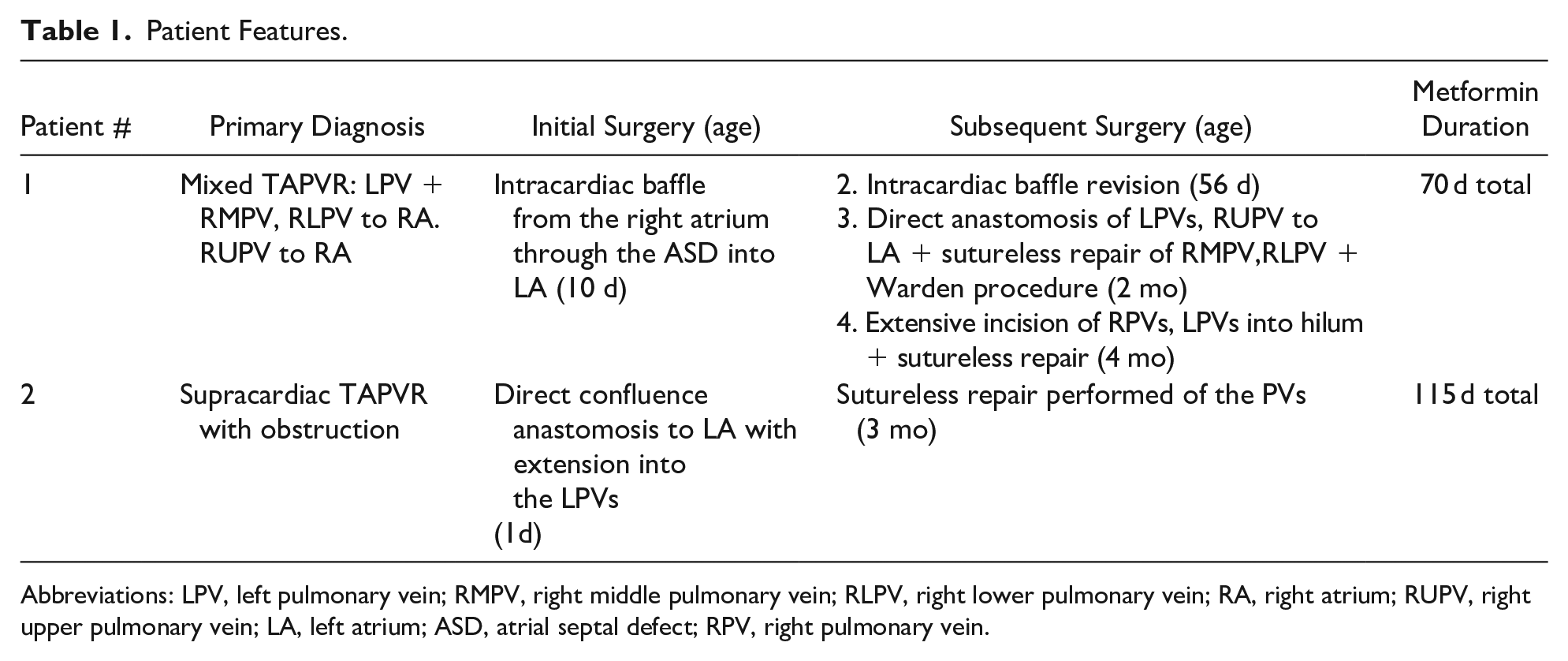
Abbreviations: LPV, left pulmonary vein; RMPV, right middle pulmonary vein; RLPV, right lower pulmonary vein; RA, right atrium; RUPV, right upper pulmonary vein; LA, left atrium; ASD, atrial septal defect; RPV, right pulmonary vein.
He underwent 2 operations (from outside hospital) to alleviate the stenosis and had a cardiac MRI and serial echocardiography to confirm the presence of re-stenosis. At our institution he had 2 more surgical attempts and at his fourth surgery, a PV biopsy performed showed extensive neointimal hyperplasia of all the veins and confirmed the presence of metakaryotic cells (Figure 1) characterized by their hollow bell shaped nuclei which can be readily identified by using modified common histologic technique. 4 In an effort to curtail the growth of the metakaryotic cells, a trial of enteral metformin was given that was initially well tolerated without lactic acidosis or hypoglycemia. After a month of clinical improvement (Figure 2), it appeared that the rate of restenosis was greatly decreased and the drug was stopped but restarted 10 days later due to increased breathing difficulty and worsening PVS on echocardiogram. The drug was discontinued after 2 more weeks due to concerns of hyponatremia which was likely diuretic related. The patient then continued to develop progressive PVS and severe pulmonary hypertension (PH) and died at age 7 months.

Example of bell shaped nuclei of metakaryotic stem cells from patient #1 patient with PVS. Feulgen-Giemsa stain.
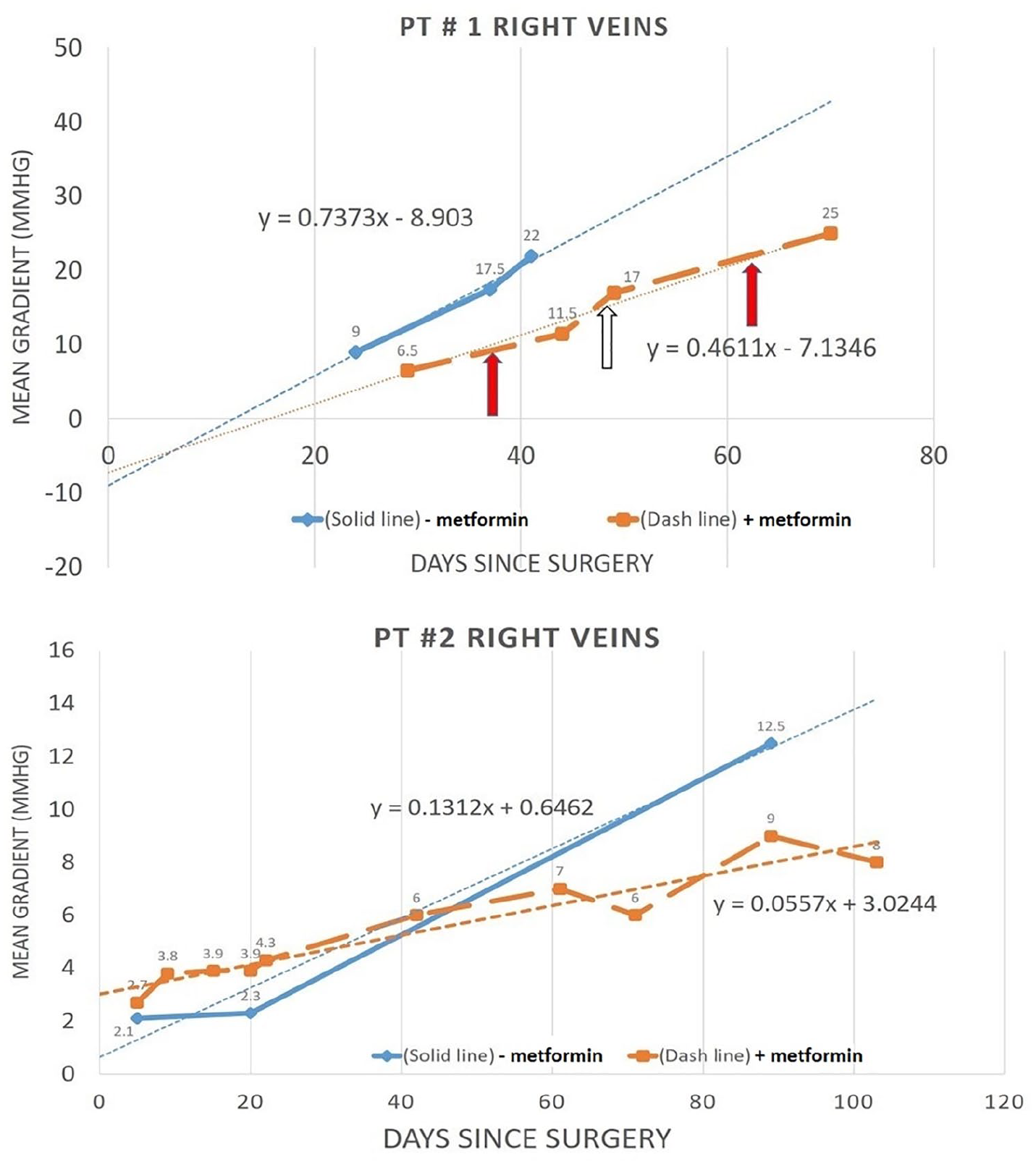
Measured PV gradient after surgery without (–metformin; solid blue line) use of metformin and after repeat surgery with (+metformin; dashed orange line) use of metformin by serial echocardiography. Dotted line (trendline) is for each time period with the equation representing the slope and intercept. Time 0 days represents the first day post-operative. Stenosis was seen in both left and right veins and was worse in the right veins shown here. Solid red arrow in patient #1 is when metformin was stopped and open arrow was when it was restarted. Patients showed a trend to a decrease rate of restenosis with the use of metformin.
The second patient was born full term with a prenatal diagnosis of supracardiac TAPVR with obstruction and had surgical repair on day one of life (Table 1). He recovered well with only a mild gradient of the pulmonary veins by echocardiography. At 3 months of age he was readmitted due to worsening respiratory distress and feeding intolerance. An echocardiogram demonstrated severe stenosis of all his pulmonary veins that was confirmed by CT angiography. He was re-operated upon with a sutureless repair of the PVS. As with the first patient, enteral metformin was started and was tolerated without side effects of hypoglycemia, lactic acidosis or feeding intolerance. He continued with serial imaging (Figure 2), but was noted to have more pulmonary edema and increase in PV gradient by echocardiography. A catheterization showed atresia of the left lower PV and mild narrowing of the right lower PV and left upper PV with mild PH. He continued metformin and showed progressive but slower rate of restenosis. Another catheterization confirmed progressive stenosis of the right lower and middle PV and suprasystemic PH. He passed away at age 7 months.
Discussion
In vitro metformin kills metakaryotic cells after 2 to 3 weeks exposure depending on metformin concentration. 5 The degree of change in the PV gradient after repeat TAPVR repair with the use of metformin was lower compared to the same time interval without metformin in previous surgery as seen by the difference in their trendlines (Figure 2). Though metformin was tolerated in these infants, a lower number of data points and lack of control subjects prevented the change in slopes from reaching statistical significance and the patients did succumb to PVS. Callahan et al demonstrated that an aggressive approach using multiple catheter/surgical interventions with adjunct imatinib ± bevacizumab could improve survival after 72 weeks in 81% that completed therapy versus 67% that didn’t. 3 However PVS still reoccurred in 67% of the patients. 3 This demonstrates the difficulty in treatment of PVS, the need for new therapeutic targets and the importance of finding any change in progression in this devastating disease.
Conclusion
Metakaryotic stem cells likely play a key role in PVS development and are inhibited by metformin with some evidence of slowing restenosis. Therefore we feel that metakaryotic cells could be a novel target for therapies against PVS. Larger clinical trials using metformin in PVS are needed.
Footnotes
Author Contributions
All authors contributed to the article concept, data analysis and editing.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This project was partially funded by the following sources: Edward Adam Jakush Metakaryotic Stem Cell Research Fund Children’s Research Institute at the Children’s Hospital of Wisconsin.