
Abstract
Health literacy assessment is a major aspect of planning health education for adolescents. We evaluated the health literacy of Japanese adolescents using both perceived and knowledge-based health literacy scales. Study questionnaires were administered to 773 junior and senior high school students aged 12 to 18 years. We tested a model describing the hierarchical relations between functional, communicative, critical, and knowledge-based health literacy using path analysis. Critical health literacy was found to be influenced by functional, communicative, and knowledge-based health literacy, while functional and knowledge-based health literacy were correlated. The model, with slight modification, was supported. The result indicates that perceived functional health literacy scores did not directly correlate with higher perceived critical health literacy; rather, they only informed critical health literacy when participants had high knowledge-based health literacy.
Keywords
Introduction
Improvement of health literacy is a key component for improving public health and well-being. 1 Health literacy is generally defined as the ability to access, understand, and critically judge and apply health-relevant information,2,3 although its specific definition and emphases can vary depending on the context.4-6 In particular, the 3-dimensional, hierarchical view—whereby health literacy is divided into functional, communicative, and critical dimensions—has been widely accepted.1,4 Functional health literacy refers to the ability to read and write about health topics to function effectively in everyday situations. Communicative health literacy is the social and cognitive ability to extract, understand, and use health-related information in everyday circumstances. Critical health literacy is the ability to critically analyze and use the information to “exert greater control over life events and situations.” (p. 264) 1 An overview of the literature on health literacy reveals that this definition of the concept has been extensively researched, specifically on the perceived aspect of one’s health literacy. 7 We focus here on adolescent health literacy because it has recently become a global concern.8-11 Health literacy during this developmental stage has several unique characteristics not observed in other stages. For example, adolescence is a period of self-decision-making, particularly concerning health-relevant behaviors such as diet and daily habits, which sometimes lead to harmful behaviors such as alcohol and smoking. Health promotion efforts that target these behaviors and habits are in considerable demand because adolescents’ lifestyle habits are precursors of adult lifestyle diseases.8,12
The recent trend in studies on the development of health literacy scale is to assess perceived health literacy comprehensively.5,13,14 For example, the European Health Literacy Survey Questionnaire (HLS-EU-Q47) measures health literacy with 12 dimensions and the Health Literacy Questionnaire with 9 dimensions.5,13 This has limitations, however, in assessing the health literacy status of younger generations due to these individuals’ unfamiliarity with the words or phrases in the scale. 15 Specifically, the knowledge needed to solve health problems in younger generations differs from that needed by older generations. 2
Besides, adolescents’ health literacy must be researched in conjunction with health promotion and health interventions in school settings. 16 Adolescents are at risk of diseases associated with certain habits, such as smoking, a sedentary lifestyle, and substance use, and at risk of suicide.17-20 Therefore, improving students’ health literacy might contribute to their preventive behavior against these lifestyle risks, which in turn might lead to a reduction in their disease risk. Health literacy assessment here is an essential step of developing suitable health promotion interventions and health education programs.21-23
In this article, we define knowledge-based health literacy as the ability to read and recognize vocabulary frequently used in the adolescent health domain. 24 At its most basic level, functional health literacy is one’s ability to read and understand information about nutrition, body mechanisms, or disease and to make appointments with doctors when needed. The discrepancy between perceptions of their functional health literacy and their objective level of knowledge-based health literacy is critical for their health care, particularly in cases where they perceive that they have sufficient functional health literacy but have rather poor knowledge-based health literacy. Therefore, this objective side of functional health literacy should be assessed. Of course, it is also important that they recognize their health literacy status because such metacognitions of health literacy can influence how adolescents behave when health-related issues arise in their daily lives. As such, health literacy should be assessed from both subjective and objective perspectives (Table 1).
Two Approaches to Health Literacy Assessment.
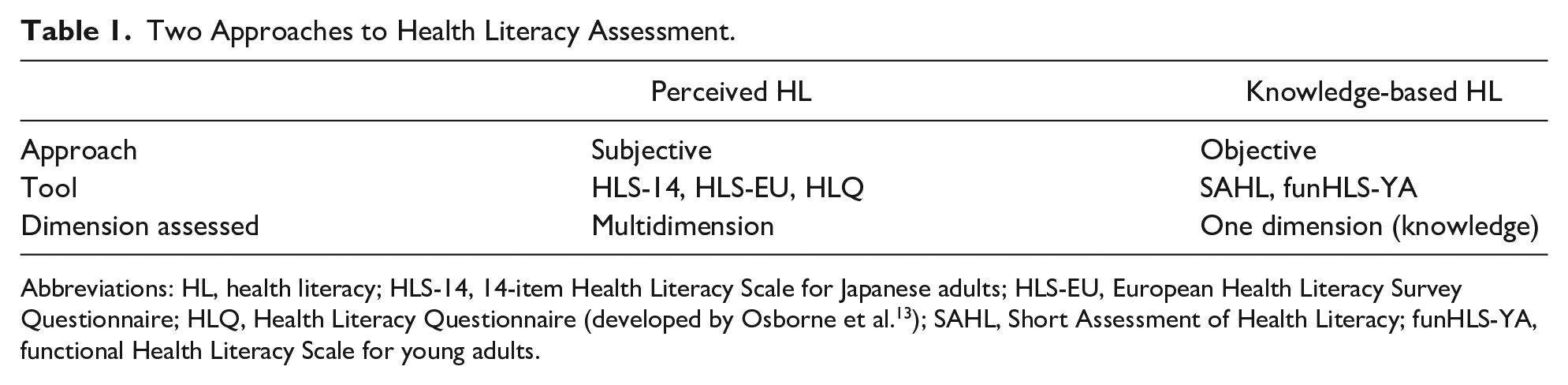
Abbreviations: HL, health literacy; HLS-14, 14-item Health Literacy Scale for Japanese adults; HLS-EU, European Health Literacy Survey Questionnaire; HLQ, Health Literacy Questionnaire (developed by Osborne et al. 13 ); SAHL, Short Assessment of Health Literacy; funHLS-YA, functional Health Literacy Scale for young adults.
Because previous studies have not reached a conclusion on the relationships between perceived health literacy and more objective knowledge-based health literacy, 22 we constructed and tested a full recursive model representing the hierarchical structure of perceived functional, communicative, and critical health literacy as well as knowledge-based health literacy (Figure 1). Specifically, the model is a manifestation of the hypothesis that the critical health literacy dimension presupposes the 3 other types of health literacy (functional, knowledge-based, and communicative), while communicative health literacy is influenced by both perceived functional and knowledge-based health literacy. Finally, perceived functional health literacy was hypothesized to correlate with knowledge-based health literacy. We implement path analysis to test the hypothetical model described in Figure 1.

Path analysis of associations among functional, communicative, critical, and knowledge-based health literacy.
Methods
Participants and Procedure
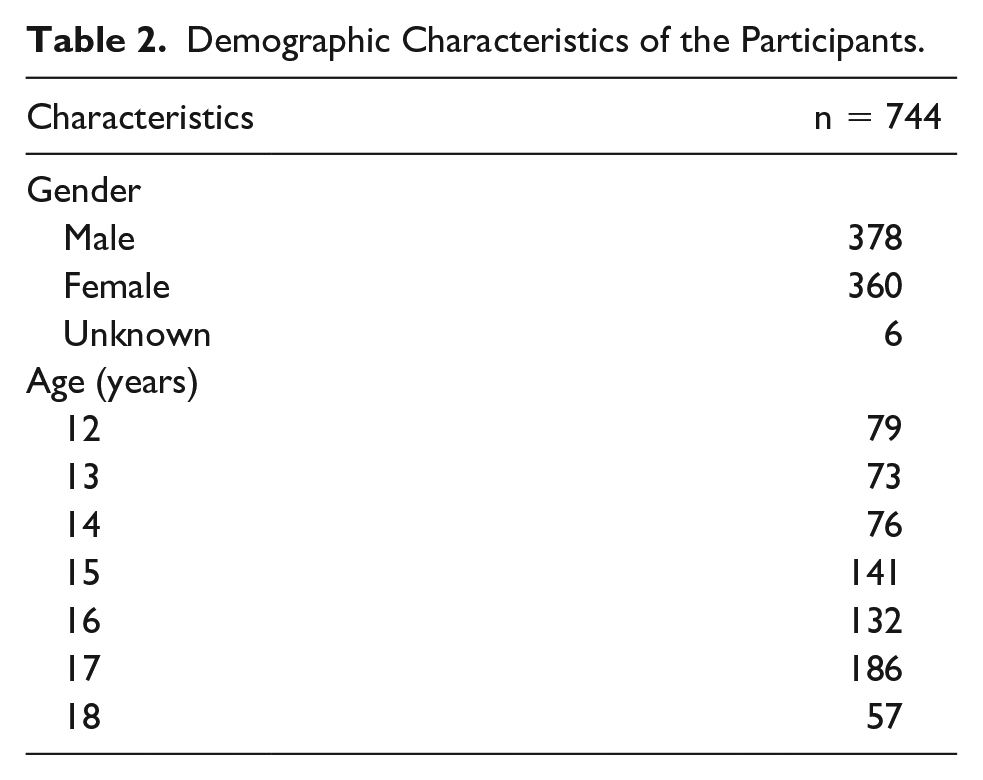
A cross-sectional survey was performed using convenience sampling. We asked the administrative officers at a nearby private high school located in the central part of Japan to cooperate in the survey. The school is located in an urban city in central Japan. Given that it is a private school, most of the students’ socioeconomic status were estimated to be upper middle class or higher, and the percentage of students who attend university or junior college was higher than average in Japan (54.8%). 25 All participants attended the same school. We asked all 773 junior high and high school students (age range = 12-18 years) at this school for their voluntary participation in this survey. All students were provided with both verbal and written explanations detailing how survey participation was voluntary and that they could stop participation any time they wanted during their homeroom hour. We asked students to sign the consent form and explained the data would be anonymized during statistical analysis. Also, students who did not agree to participate in the survey were asked to submit blank questionnaires. It took approximately 5 to 10 minutes to complete the entire questionnaire. Overall, 762 students agreed to participate in the survey by submitting their questionnaire (collection rate of 98.6%). Of these, 18 cases were removed from the subsequent analysis because of their incompleteness. As a result, 744 cases were analyzed. The demographic characteristics of the analyzed participants are presented in Table 2.
Demographic Characteristics of the Participants.
This study was reviewed and approved by the Research Ethics Committee of Nagoya University of Commerce and Business (Approval Number 16021). All the data were collected anonymously.
Measurements
Knowledge-Based Health Literacy (funHLS-A)
We developed a new scale, the functional Health Literacy Scale for Adolescents (funHLS-A), to assess knowledge-based health literacy. This scale is another version of the functional Health Literacy Scale for Young Adults (funHLS-YA), and the construction process was the same with funHLS-YA. 15 Items consist of a word or phrase describing (1) infectious and noncommunicable diseases frequently observed in adolescence, (2) nutrition, (3) the body, and (4) other knowledge needed for medical consultation. Participants are asked to answer each item by selecting the term that best describes the given item out of 4 choices (e.g., the response options for “syphilis” were [1] food intoxication, [2] allergy, [3] sexually transmitted disease, and [4] don’t know). When participants do not know the answer, they are asked to choose “don’t know.” The funHLS-A was developed based on the Short Assessment of Health Literacy–Spanish and English,24,26 with modifications. We chose 21 items for this study based on the simplified Delphi method with informal discussions by 3 experts. Supplemental Material 1 (available online) shows some sample items from the funHLS-A.
Health Literacy Scale for Japanese Adults (HLS-14)
The 14 items of the HLS-14 were used to assess perceived health literacy. 7 This scale is one of the most frequently used health literacy scales in Japan and contains 3 subscales: functional health literacy, communicative health literacy, and critical health literacy. As this measure was designed for adults, we adjusted the phrasing of the items to ensure that they were suitable for adolescents. A 5-point Likert-type scale (5 = strongly disagree to 1 = strongly agree) was used. The sample item in the functional health literacy dimension was, “When you read instructions or leaflets given by the school nurse’s office, hospitals, or pharmacies, do you agree or disagree with the following?” Question 1 was “I find characters that I cannot read” (Item 1). The functional health literacy subscale contains 5 items assessing reading materials on medicine and health. The communicative health literacy subscale also contains 5 items assessing individuals’ ability to collect and understand information, to communicate with others on the topic, and to apply the information in daily life. Finally, the critical health literacy subscale contains 4 items asking participants’ decision-making process. These 3 dimensions of health literacy conform to a hierarchy, with critical health literacy being the most profound, followed by communicative health literacy and then functional health literacy. Participant’s responses to the HLS-14 might be prone to the Hawthorne effect; thus, the correlation coefficients for knowledge-based health literacy (funHLS-A) and the 3 subscales of HLS-14 may provide information on any discrepancy between perceived and objective health literacy.
Statistical Analysis
Calculation of the Ability Parameter in Each Participant as the Knowledge-Based Health Literacy Score
A 2-parameter model was applied to estimate the difficulty and discrimination parameters for each item of the funHLS-A. Based on these parameters, each participant’s ability parameter was estimated. This parameter represents each participant’s knowledge-based health literacy. The ability parameter was then included as a variable (knowledge-based health literacy) in the hypothetical model that acts on both communicative and critical health literacy. We employed R version 3.4.1 and the “ltm” package for the item response theory analysis.
Pearson’s Correlation Coefficients
Pearson’s correlation coefficients were calculated between each of the HLS-14 subscales and the ability parameter of the funHLS-A to estimate the scale relationships.
Testing the Research Model
Any modification of the hypothesized full recursive model was tested via a path analysis using the following fit indices: (1) χ2 statistic, (2) the comparative fit index (CFI), 27 and (3) the root mean square error of approximation (RMSEA). 28 The Akaike information criterion (AIC) was used to compare the relative fit of the model to the data. 29 CFI values of >.90 indicate acceptable model-data fit, while RMSEA values <.08 indicate satisfactory fit (values over .10 signify that the model should be rejected). The model testing and subsequent latent-class analysis were conducted using Mplus 7.4 to analyze the relations with participants’ responses to each item in the functional health literacy dimension of the HLS-14 and the ability parameters of participants in the funHLS-A. 30 To determine the optimal number of classes, varying latent class models, starting from a one-class model, were tested until an optimal solution was reached. The fit indices used to compare the relative fit of the solutions were the AIC, the Bayesian information criterion, and the sample-size adjusted Bayesian information criterion. Likelihood ratio tests such as the Vuong-Lo-Mendell-Rubin and Lo-Mendell-Rubin adjusted likelihood ratio tests and the Bootstrapped Likelihood Ratio Test were also implemented. The criterion for significance was an α < .05. The entropy was also considered to check the degree of homogeneity within and the independence between classes. 31
Missing Cases and Missing Data
We applied the full information maximum likelihood in all cases with missing data. There were 18 missing cases, most of which were from students who did not provide responses to most of the questions. In addition to these missing cases, we observed missing values in several submitted questionnaires. We could not find any common mechanism among these missing cases and missing values.
Results
Ability Parameter Estimation and Descriptive Statistics
The ability parameter estimation was implemented with all 21 items on the scale. The difficulty parameters ranged from −1.66 to 1.91, and discrimination parameters from 0.43 to 1.23. The test information curve indicated that this scale provides more information on those with average or slightly under average health literacy. Using this information, we calculated each participant’s ability parameter.
The descriptive statistics for all variables, along with the correlations, are shown in Supplemental Material 2 (available online). Critical health literacy had a strong positive correlation with communicative health literacy, but weaker positive correlations with the other 2 subscales of the HLS-14 and knowledge-based health literacy.
Path Analysis
Figure 1 displays the results of the path analysis of the research model.
All path coefficients in the research model were significant except for the path from functional health literacy to critical health literacy. The strongest coefficient was for the path from communicative health literacy to critical health literacy. The nonsignificant path from functional health literacy to critical health literacy represents the hierarchical nature of the 3 dimensions of the HLS-14 (from functional to communicative health literacy, and from communicative health literacy to critical health literacy). We modified the model by deleting this path, and the resulting modified model was satisfactorily fit to the data (χ2 = 1.836, df = 1, p = .18, CFI = 0.997, RMSEA = 0.033, AIC = 12616.032). The R2 values for communicative health literacy and critical health literacy were 0.115 and 0.336, respectively.
We also conducted a latent class analysis using the ability parameters of the funHLS-A and the 4 items in the functional dimension of the HLS-14. We found that the 4-class and 5-class models were supported, and we adopt the 4-class model (Supplemental Material 3, [available online]) because of the easiness of interpretation.
Discussion
Item response theory analysis indicated that the funHLS-A is informative for the assessment of those with average or slightly below average health literacy. By the characteristics of this scale, it is thus suitable for use as a screening test, not to determine how much students know, but to identify those who would have difficulty in knowledge-based health literacy. The correlation analysis did not validate this tool, but the relatively low correlation between funHLS-A and HLS-14 suggests a discrepancy between participants’ knowledge-based health literacy and perceived health literacy. The results suggest that health professionals should assess not only the extent to which adolescents “appraise” their functional health literacy but also to what extent they “actually” can read and understand health information. Some past literature has utilized this “subject-object” approach22,32-34 or at least discussed it, 35 and most of these studies reported “weakness of coherence between the underlying constructs measured by the different approaches.” (p. 10) 35 The results of the research model in this study suggested that a mixed approach to the assessment of health literacy (i.e., measuring both subjective and objective health literacy) is more informative when different constructs in subjective and objective approaches are linked with a causal model.
The path analysis results showed that the constructed full recursive model was not supported, which yielded the modified model (Figure 1). More specifically, functional health literacy did not directly contribute to critical health literacy. Nevertheless, our inclusion of knowledge-based health literacy allowed for a more sophisticated interpretation of the associations among the 3 facets of the HLS-14.
Interpretation of the Final Model
The modified research model indicated that high perceived functional health literacy scores led to higher scores in communicative health literacy, which in turn increased critical health literacy scores. However, when communicative health literacy scores were the same, higher knowledge-based health literacy scores had a positive effect on critical health literacy. Additionally, higher knowledge-based health literacy had positive effects on communicative health literacy, which in turn appeared to boost critical health literacy.
As suggested in previous research, 7 3 subscales of the HLS-14 did not equally correlate with each other. A post hoc latent class analysis revealed a possible reason for this point. The latent class analysis contained the ability parameters of the funHLS-A and 4 items from the functional health literacy subscale of the HLS-14. The 4-class and 5-class models emerged as significant, and we adopted the 4-class model for ease of interpretation. The 4-class model suggests that around 22.5% of the participants (#1 in Figure 2) perceived themselves as having sufficient reading ability and did not require help from others (Item 5 in the functional health literacy subscale of the HLS-14). In reality, however, participants in this class had the lowest mean score on the funHLS-A of the 4 classes. While none of the items of the funHLS-A test reading ability, those who do not seek help from others when they have difficulty in reading may have fewer opportunities to check and correct their latent-reading difficulties. This is particularly an issue with the Japanese language, which utilizes 3 different character systems: hiragana, katakana, and kanji. The former 2 are basic phonetic lettering systems in which characters are relatively easy to pronounce because they comprise phonograms; kanji, on the other hand, is a logographic system with characters borrowed from the Chinese language, which are more difficult to pronounce because they comprise logograms. Most items in the funHLS-A include kanji characters. However, we cannot definitively conclude that the weak relationships between functional health literacy and critical health literacy in the HLS-14 resulted from participants’ difficulty in reading kanji characters. Future research might add items assessing how to read given kanji characters in the funHLS-A.

A latent class analysis of perceived functional health literacy and ability parameter of knowledge-based health literacy.
Limitations
First, this study used a cross-sectional design, which is an inherent limitation. Second, funHLS-A evaluates health literacy by forcing participants to read silently. In a future study, it would be better to include items that ask if participants can read the words in the item correctly, as in the SAHL (Short Assessment of Health Literacy)-E/S. 24 Third, the selection of the items in the funHLS-A should be more systematic—for instance, other studies used a more systematic Delphi method or more systematic procedures.14,36 Forth, the funHLS-A has not been validated using other similar assessment tools, such as SAHL, albeit the new tool was developed using item response theory. Despite the limitations, this study has strength in focusing on previously under-described areas, that is, the health literacy of Japanese adolescents.
Conclusion and Recommendation
Knowledge-based health literacy adds to our understanding of the 3 dimensions of perceived health literacy and their relationship. Specifically, the knowledge-based health literacy score (i.e., the ability parameter) can differ even when all dimensions of perceived health literacy are aligned. Based on the result of latent class analysis, we strongly recommend that health professionals implement health literacy measurements using both subjective and objective approaches. These results also contribute to constructing and enhancing tailor-made health promotion programs for the given health literacy classes (e.g., #1-4 in Figure 2) in educational settings.
Supplemental Material
Sup_1 – Supplemental material for Assessing Knowledge-Based and Perceived Health Literacy Among Japanese Adolescents: A Cross-Sectional Study
Supplemental material, Sup_1 for Assessing Knowledge-Based and Perceived Health Literacy Among Japanese Adolescents: A Cross-Sectional Study by Takashi Tsubakita, Nobuo Kawazoe, Mahoko Ichikawa, Satoko Matsumoto and Masumi Sugawara in Global Pediatric Health
Supplemental Material
Sup_2 – Supplemental material for Assessing Knowledge-Based and Perceived Health Literacy Among Japanese Adolescents: A Cross-Sectional Study
Supplemental material, Sup_2 for Assessing Knowledge-Based and Perceived Health Literacy Among Japanese Adolescents: A Cross-Sectional Study by Takashi Tsubakita, Nobuo Kawazoe, Mahoko Ichikawa, Satoko Matsumoto and Masumi Sugawara in Global Pediatric Health
Supplemental Material
Sup_3 – Supplemental material for Assessing Knowledge-Based and Perceived Health Literacy Among Japanese Adolescents: A Cross-Sectional Study
Supplemental material, Sup_3 for Assessing Knowledge-Based and Perceived Health Literacy Among Japanese Adolescents: A Cross-Sectional Study by Takashi Tsubakita, Nobuo Kawazoe, Mahoko Ichikawa, Satoko Matsumoto and Masumi Sugawara in Global Pediatric Health
Footnotes
Acknowledgements
The authors thank Nagoya University of Commerce and Business for their contributions that helped in the support and management of the study.
Author Contributions
TT: Contributed to the conception and design; data collection and analysis; drafted the manuscript; finalized the manuscript.
NK: Contributed to the conception and design; data collection and analysis; drafted the manuscript.
MI: Contributed to the conception; designing and finalizing the questionnaire; data collection.
SM: Contributed to data analysis and the interpretation of the results; critically revised the manuscript.
MS: Contributed to conception and design; the interpretation of the results; critically revised the manuscript.
All authors reviewed the initial manuscript and participated in the preparation of the final manuscript.
All authors approved the manuscript for submission.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study was funded by a general research grant from Nagoya University of Commerce and Business.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.