
Abstract
Diabetic ketoacidosis (DKA) is a serious, potentially lethal complication of type 1 diabetes mellitus that may be present at diagnosis. The aim of this study was to determine factors associated with presentation in DKA in new-onset youth and compare the rate of DKA and risk factors to a similar study 15 years prior. This study was a retrospective chart review of newly diagnosed patients with type 1 diabetes mellitus from 2010 to 2013. Of the 276 patients, 29% presented in DKA, compared with 38% 15 years prior (P < .002). Those with Medicaid, those misdiagnosed at initial encounter, and those not evaluated by a pediatrician initially were more likely to present in DKA (P = .002, P = .002, P < .001, respectively). The diagnosis of diabetes was not elicited in one third of patients who ultimately presented in DKA. Pediatricians should be reeducated to ask about polyuria and polydipsia in routine encounters. Furthermore, public awareness initiatives are needed to reduce late presentation in DKA.
Introduction
Diabetic ketoacidosis (DKA) is a serious, potentially lethal complication of type 1 diabetes mellitus (T1D) and may be the initial mode of presentation for patients with new-onset T1D.1-4 Given the classic symptoms of polyuria and polydipsia, both families and physicians should be able to easily identify the symptoms of T1D in a timely fashion. Therefore, the initial presentation of T1D in DKA should be uncommon. However, several studies show that up to 40% of patients with new-onset T1D present in DKA.2,3,5-7
DKA can be associated with various adverse outcomes. Cerebral edema remains the most common cause of mortality in pediatric patients with DKA.8,9 It occurs in 0.5% to 0.9% of patients in DKA with a mortality rate of 21% to 24%.10-12 Not only does late presentation in DKA place the patient at an increased risk for morbidity and mortality, but it also increases health care costs. 13 Those patients in DKA are generally admitted to the intensive care unit and may have an extended hospital stay with various complications that drive up costs. In addition, initial presentation in DKA leads to a poorer prognosis and has been shown to be associated with less residual β cell function after diagnosis and poorer glycemic control.14-17
Risk factors for late presentation in DKA include low socioeconomic status, young age, and delay in diagnosis. 7 The aims of this study were to
Determine factors associated with presentation in DKA in new-onset T1D children and adolescents
Compare the rate of DKA and delay in diagnosis to a similar study at the same institution 15 years ago to see if these factors have changed since 2003 18
Patients and Methods
We performed a retrospective chart review of all newly diagnosed patients with T1D from 2010 to 2013 seen by the Division of Pediatric Endocrinology associated with Cohen Children’s Medical Center located in Queens, New York. Children with other forms of diabetes were excluded. Each patient was analyzed with regard to age at presentation, symptoms at presentation, mode of presentation (hyperglycemia with or without ketosis or DKA [defined by protocol based on pH < 7.3]), family history of diabetes, initial pH at diagnosis, initial hemoglobin A1C at diagnosis, type of insurance coverage (Medicaid or private), median income by zip code, physician who initially evaluated the patient, and timing of presentation (whether or not there was a delay in diagnosis). A “delay in diagnosis” was defined as a patient with new-onset T1D who was evaluated and not sent for immediate further evaluation to the hospital or to a pediatric endocrinologist within 24 hours.
We analyzed the group of patients who presented in DKA and those who had a delay in diagnosis of T1D to identify any apparent risk factors. Specifically, we assessed whether age, timing of presentation, evaluating physician, and socioeconomic status (using type of insurance and median income by zip code as proxies) were significant factors that were associated with presentation in DKA and with a delay in diagnosis.
Descriptive statistics (eg, mean and standard deviation [SD] for continuous variables and frequencies and proportions for categorical variables) were calculated. Chi-square tests of association were performed to assess if any differences exist between each categorical factor of interest and each binary outcome (DKA or delay in diagnosis). Odds ratios (ORs), along with the corresponding 95% confidence intervals (CIs), were also computed as appropriate. Wilcoxon rank sum tests were performed to assess if any differences exist between each continuous factor of interest (ie, age at diagnosis and pH) and DKA as well as delay in diagnosis. Correlation between age and initial pH among patients less than 5 years of age who presented in DKA was assessed using Spearman’s rank-order correlation. For all analyses, a result was considered statistically significant at the P < .05 level of significance.
All analyses were conducted using SAS version 9.4 (SAS Institute Inc, Cary, NC).
Ethical Approval and Informed Consent
This study was approved by the Institutional Review Board of Northwell Health (Ethical Approval Reference Number 16-660), and data were collected and managed using REDCap (Research Electronic Data Capture) tools hosted at Northwell Health. 19 Informed consent not required due to research not involving more than minimal risk and granted expedited approval. REDCap is a secure, web-based application designed to support data capture for research studies, providing the following: (1) an intuitive interface for validated data entry; (2) audit trails for tracking data manipulation and export procedures; (3) automated export procedures for seamless data downloads to common statistical packages; and (4) procedures for importing data from external sources. Medical records were reviewed by the primary author to collect all key information. Validity was checked by other authors if there was any uncertainty into how to classify patients.
Results
A total of 344 cases of new-onset diabetes mellitus were diagnosed in this population from 2010 to 2013. Sixty-eight cases were excluded due to other diagnoses such as type 2 diabetes mellitus, cystic fibrosis, steroid-induced diabetes, and metabolic disorders. There were 288 cases of T1D; 276 charts were available for review (Figure 1).
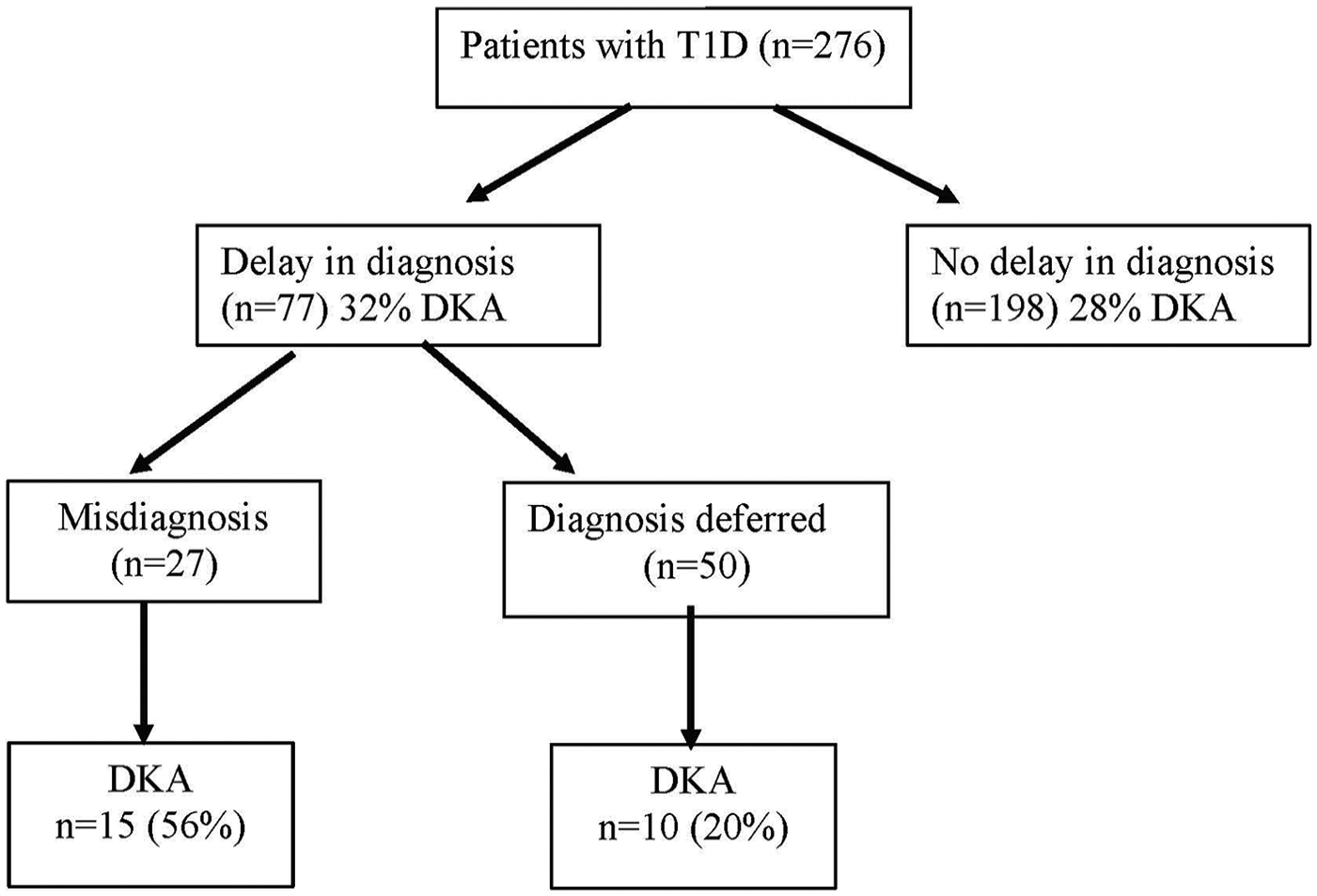
Timing and presentation of T1D diagnosis.
Demographics
Of the 276 patients with newly diagnosed T1D, 143 (52%) patients were male. Age at presentation ranged from 1 year to 17 years (mean age of 9.6 ± 4 years). Forty-nine (18%) were aged 1 to 5 years, 102 (37%) were aged 6 to 10 years, and 125 (45%) were aged 11 to 17 years. Of those who reported race and ethnicity, 119 patients (53%) were White, 47 patients (22%) were African American, 14 patients (6%) were Asian, and 6 patients (3%) were Hispanic with 33 patients (15%) identifying as multiple or other races and/or ethnicities.
Family History
With regard to family history, 204 patients (74%) reported no significant family history of type 1 or type 2 diabetes. While 24 patients (9%) had a first-degree relative with T1D, 32 patients (12%) had a second-degree relative with T1D, and 16 patients (6%) had a first-degree relative with type 2 diabetes.
Insurance and Median Income by Zip Code
One hundred forty-six patients out of 258 with recorded insurance coverage types (57%) had private insurance, while 112 patients (43%) had Medicaid. Using median income by zip code, the median income was $85 997 with a standard deviation of $30 777.
Physician Information
One hundred fifty-eight patients (57%) were seen by a pediatrician on initial presentation, while 108 patients (39%) were seen in an emergency room, in an urgent care clinic, or by a general practitioner. Ten patients were seen by another physician such as a subspecialist (4%).
Clinical Characteristics
Timing of Presentation
Of the 276 patients diagnosed with new-onset T1D, 198 patients (72%) were diagnosed on the day of admission (ie, no delay in diagnosis). In 77 patients (28%), there was a delay in diagnosis, that is, they were diagnosed on a second or later visit; 1 patient (0.4%) had an unclear timing of diagnosis (Figure 1).
Of the 77 patients in whom there was a delay in diagnosis, 27 were given a misdiagnosis and sent home. Of the remaining 50 patients in whom there was a delay in diagnosis, 7 patients were asymptomatic and were found to have hyperglycemia and/or glycosuria on routine laboratory testing and later sent for further evaluation once the results were available. In the remaining 43 patients, the diagnosis of type 1 diabetes was not elicited at the initial physician encounter despite the fact that the patient was symptomatic (established retrospectively following admission).
Of the 77 patients with a delay in diagnosis, 33 patients (42.9%) were initially seen in an emergency room, in an urgent care clinic, or by a general practitioner; 39 patients (50.7%) were first evaluated by a pediatrician; and 5 patients (6.5%) were seen by another physician such as a subspecialist.
Mode of Presentation
One hundred ninety-six patients (71%) presented with hyperglycemia with or without ketosis, and 80 patients (29%) presented in DKA.
Symptoms
The most common symptoms at presentation were polyuria and polydipsia, which were nearly universal despite mode of presentation (91%) as seen in Figure 2. Other signs and symptoms at presentation were weight loss (58%), abdominal pain (17%), lethargy (13%), Kussmaul breathing (7%), and blurry vision (6%). Other symptoms noted included nocturia, enuresis, polyphagia, emesis, fever, weakness, chest pain, and irritability.

Symptoms at presentation and risk of DKA.
Laboratory Findings at Diagnosis
Mean hemoglobin A1C at presentation was 11.3 ± 2.2% (range = 6.3% to 17.6%). Mean pH at diagnosis was 7.3 ± 0.13 (range = 6.85 to 7.55).
Fifty-eight patients (24%) had 1 positive autoantibody, 112 patients (46%) had 2 positive autoantibodies, and 74 patients (30%) had 3 positive autoantibodies.
Aim 1: Factors Associated With Presentation in DKA in New-Onset T1D
Demographics, Clinical Characteristics, and Risk of DKA
The mean age of children with new-onset diabetes mellitus presenting with DKA was 9.0 ± 3.8 years. The rate of DKA was 29% (14/49) in the 1- to 5-year age group, 35% (36/102) in the 6- to 10-year age group, and 24% (30/125) in the 11- to 17-year age group (P = .18). There was no statistically significant correlation between age and pH in those from 1 to 5 years (ρ = 0.15, P = .3).
The mean hemoglobin A1C of those patients presenting with DKA, 11.9%, was higher than the HbA1c of those who did not present with DKA, 11.06% (P = .004).
Family History and Risk of DKA
Sixty-four patients (31%) of those with no family history of diabetes presented with DKA. Three patients (13%) of those with a first-degree relative with T1D presented with DKA. Ten patients (31%) with a family history of a second-degree relative with T1D presented with DKA, and 3 patients (19%) of those with a first-degree relative with type 2 diabetes presented with DKA.
Timing of Diagnosis and Risk of DKA
DKA at presentation was found in 29% of the subjects in whom the diagnosis of T1D was made on the initial encounter compared with 32% of the subjects in whom the diagnosis was delayed at least 24 hours (P = .44). Of the 77 patients in whom there was a delay in the diagnosis of T1D, 27 were given a misdiagnosis, and in 50, the diagnosis was deferred, pending laboratory evaluation. DKA was found in 56% of those in whom a misdiagnosis was given compared with 20% of those in whom the diagnosis was deferred (OR = 5.0 [95% CI = 1.8-14.0]; P = .002), as seen in Figure 1. Table 1 shows the misdiagnoses that were given and the outcome (ie, whether or not the patients developed DKA).
Misdiagnoses.

Abbreviation: DKA, diabetic ketoacidosis.
Insurance Coverage and Risk of DKA
Thirty-eight percent of patients with Medicaid presented with DKA compared with 20% among those with private insurance (OR = 2.4 [95% CI = 1.4-4.2]; P = .002) as seen in Figure 3.

Socioeconomic status and risk of DKA.
Median Income and Risk of DKA
Median income by zip code was not found to be a statistically significant risk factor for presenting with DKA, P = .07 (Figure 3).
Evaluating Physician and Risk of DKA
Fourteen percent of patients who were initially evaluated by a pediatrician presented with DKA compared with 53% of patients evaluated by either a physician in the emergency room, clinic, or by a general practitioner (P < .0001).
Aim 2: Comparisons to Previous Study
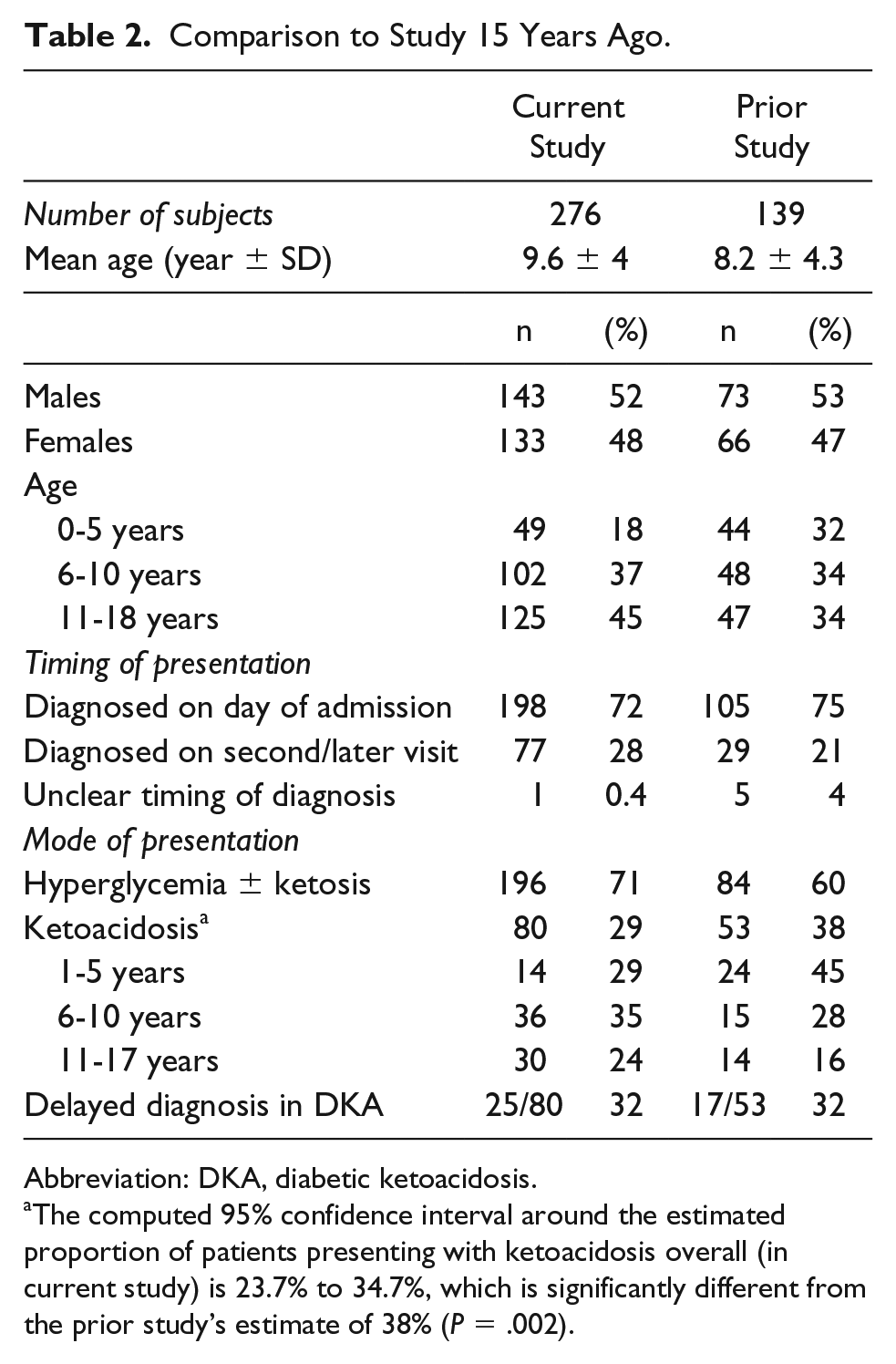
In this study, 29% (80/276) of patients with new-onset T1D presented with DKA, compared with 38% (53/139) in our prior study ([95% CI = 23.7% to 34.7%]; P = .002). Of the patients who presented with DKA, there was a similar delay in diagnosis, 31% (25/80) in the current study, compared with 32% (17/53) in the prior study (Table 2).
Comparison to Study 15 Years Ago.
Abbreviation: DKA, diabetic ketoacidosis.
The computed 95% confidence interval around the estimated proportion of patients presenting with ketoacidosis overall (in current study) is 23.7% to 34.7%, which is significantly different from the prior study’s estimate of 38% (P = .002).
Discussion
Presentation in DKA in patients diagnosed with new-onset T1D should be a rare event since invariably the patients all have prominent symptoms of hyperglycemia, of which polyuria and polydipsia are the most striking. However, the rate of DKA at presentation of children with T1D is relatively common and has remained stable at approximately 30% in multiple geographic areas in the United States from 2002 through 2010. 20 For example, the rate of DKA at presentation in the Pediatric Diabetes Consortium in 2013 (composed of 7 pediatric diabetes centers) was 34% (ranging from 28% to 40% across the centers), 1 and the rate in the 6 center SEARCH study between 2002 and 2004 was 29.4%. 4 These US rates are higher than those reported in Canada (18.6%) 21 and Finland (19.4%), 22 but similar to the rates in some European studies that have remained unchanged over the past 20 years. 23 Similar stable rates without decline have been noted in New Zealand. 5 Even more alarming is the fact that in one large center in the United States (Barbara Davis Center for Diabetes in Denver, Colorado), the rate of DKA at diagnosis actually increased from 29.9% in 1998 to 46.2% in 2012, temporally correlating to an increase in child poverty from 10% in 2000 to 18% in 2012. 6 This rate is consistent with the rates in countries with poor access to health care and low public and physician awareness of diabetes. 24 In our population, we saw a modest decline from 38% to 29% over the past 15 years. However, the demographics during this study period have changed in that only 18% of the subjects in the current study were aged 1 to 5 years compared with 32% in the prior study. Therefore, this modest decline in DKA rates from 38% to 29% could actually be driven by demographic differences, rather than temporal differences, since presentation in DKA is more common in the very young.
The high prevalence of DKA at initial presentation of T1D demonstrates that not only are the patients and their families unaware of these classic symptoms, but physicians all too frequently are failing to elicit these symptoms at patient encounters. In keeping with other studies, we found misdiagnosis (ie, diagnostic error) and lack of private insurance risk factors for presenting with DKA. 7 Median income by zip code, another proxy for socioeconomic status, did not quite reach statistical significance. Though not found to be statistically significant, there may be a trend toward those living in lower incomes having a greater proportion of patients who present with DKA compared with subjects living in higher income areas (Figure 3).
Several studies, including our prior study, report higher rates of DKA at diagnosis in young children,4,7,22 while others have found higher rates in both younger and older children, perhaps the result of less parental involvement in the older children.22,23 Young age was not shown to be associated with presenting in DKA in our study. This may be partly due to the older mean age of the subjects (9.6 years vs 8.2 years in prior study) and the small percentage of patients presenting under 5 years of age (18% vs 44% in prior study). Thus, this population over a short 4-year period may not have been as representative with a smaller sample size of young patients.
Nonetheless, there are limitations to this study. Median income by zip code is only a proxy for socioeconomic status and may not represent the family’s actual income. In addition, the retrospective nature of this study is limited by completeness of medical record and historical accuracy of parents’ report.
Those evaluated by a pediatrician were less likely to present in DKA, which may be due to less severe symptoms at the time, prompting them to seek routine medical care as opposed to going to the emergency room. Therefore, those presenting to an emergency room does not imply increased misdiagnosis and DKA but rather may have been directly referred due to severity of symptoms.
A bigger challenge is to increase awareness of the early symptoms of T1D in both the general public and among primary care physicians. Thirty-two percent of patients with new-onset diabetes were not identified at initial physician encounter despite the fact that the classic symptoms of polyuria and polydipsia are present in virtually all patients with new-onset diabetes. Among those given a misdiagnosis (ie, diagnostic error), the rate of ultimately presenting in DKA was far higher (56%) than in those in whom the diagnosis was deferred, pending further investigations (20%). Another limitation is that we did not have access to initial encounters outside of the hospital. Therefore, we could not tell if diabetes was considered on the differential or if the initial provider truly failed to elicit these symptoms. In addition, often there is an intercurrent illness that leads to a more severe presentation of diabetes. Consequently, some of those that were misdiagnosed should have been co-diagnosed with diabetes.
In order to attempt to reduce the risk of DKA at presentation of T1D, pediatricians and primary care providers should be reeducated and reminded to ask about change in thirst and urination in office encounters. Perhaps, these key questions should be added to the electronic medical record encounter to prompt physicians who often have minimal time to see patients. This should reduce the rate of misdiagnosis, that is, diagnostic error and ensure that these questions are a part of their routine review of systems.
A public awareness campaign focusing on those less than 5 years of age has been proposed, specifically geared toward educating pediatricians, pediatric nurses, mothers, and nursery school teachers. 25 Although some community-based, poster-focused awareness campaigns have had minimal to no effect,3,26 the more focused Parma campaign in Northern Italy was highly effective. This was a school- and physician-based campaign focusing on the earliest symptom of diabetes, nocturnal enuresis in a previously “dry” child. During the 8-year campaign, the cumulative frequency of ketoacidosis in the province of Parma dropped from 78% to 12.5%. 27
In the United States, the nonprofit Beyond Type 1, founded by celebrities such as Nick Jonas, Juliet de Baubigny, Sarah Lucas, and Sam Talbot, has been leveraging the power of social media and technology to increase awareness of classic signs and symptoms of diabetes through education and advocacy. The Beyond Type 1 campaign has been distributed in 22 states and to over 28 000 pediatric offices, serving over 90 million patients annually. 28 This campaign rolled out in New Zealand in September 2017. 29
Education, Awareness, Support, and Empowerment (EASE) T1D, sponsored by the nonprofit Institute for Education, Research, and Scholarships (IFERS), is a California-based nonprofit that advocates educating parents on the signs and symptoms of T1D at all well baby/child care visits in an effort to prevent DKA. In addition, focusing on educating parents, EASE T1D helped support passage of California Senate Resolution 63 that encourages health care practitioners to discuss the warning signs and symptoms of T1D with parents. 30
A number of national campaigns have been launched, the most well known of which is the Diabetes UK 4Ts (Toilet, Thirsty, Tired, Thinner) campaign aimed at educating the public about the symptoms of T1D. 31 Diabetes Australia has incorporated the 4Ts in its “It’s About Time” early detection of diabetes campaign, 32 and Diabetes Ireland also launched a campaign to encourage earlier diagnosis of T1D. 33 In addition, in October 2018, the National Assembly for Wales Petitions Committee Petition discussed P-04-682 Routine Screening for Type 1 Diabetes in Children and Young People, which mandates checking a child for diabetes if they present with any of the 4 Ts and immediate referral to a diabetologist. 34
Conclusion
Increasing public awareness of the classic symptoms of polyuria and polydipsia can be expected to reduce late presentation in DKA, as has been noted in children with a family history of T1D. In our study, those with delayed diagnosis did not have increased rates of DKA, except in the case of misdiagnosis. Although better physician and community education may improve overall rates of DKA in early recognition and avoiding premature closure after an initial diagnosis is made, it remains to be determined how effective and scalable these public awareness campaigns will be. Economic factors such as poverty and high-deductible health plans may still result in late presentation, so it may be prudent to screen and educate some of these high-risk patients at routine health encounters. Given that almost one third of patients with DKA at presentation were not identified at initial physician encounter, physicians need to be more vigilant about the possibility of diabetes and be reminded to ask about changes in thirst and urination at all encounters.
Footnotes
Acknowledgements
Thank you to Margaret Pellizzari for providing the data. Thank you also to the Pediatric Endocrinology group at Cohen Children’s Medical Center.
Author Contributions
SRM and GF conceptualized and designed the study, drafted the initial manuscript, and reviewed and revised the manuscript; JF performed the data analysis, interpretation of results and reviewed and revised the manuscript; All authors approved the final manuscript as submitted and agree to be accountable for all aspects of the work.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.