
Abstract
Objective
This study aimed to investigate the feasibility and reliability of pulse oximetry combined with cardiac auscultation in screening neonatal congenital heart disease (CHD).
Methods
This was a retrospective, observational, screening study. All newborns included in the study were at the Second Affiliated Hospital of Wenzhou Medical University from July 2019 to January 2020. Primary screening of CHD was conducted by pulse oximetry combined with cardiac auscultation assays. Indices, including sensitivity, specificity, the positive/negative predictive value, the positive/negative likelihood ratio, and the diagnostic odds ratio, were calculated. The area under the relative operating characteristic curve of the subjects was measured.
Results
A total of 3327 neonates were enrolled, among whom 139 were diagnosed with CHD and the incidence of CHD was 4.2%. The sensitivity, specificity, diagnostic odds ratio, and area under the relative operating characteristic curve of pulse oximetry combined with cardiac auscultation were 89.9%, 94.7%, 169.0, and 0.923, respectively.
Conclusions
Pulse oximetry combined with cardiac auscultation is a novel screening method with acceptable accuracy and feasibility for neonatal CHD. This combination method is worth promoting widely.
Introduction
Congenital heart disease (CHD) is the most common congenital anomaly of newborns, and it is mainly caused by abnormality of the fetal heart and large blood vessels during embryonic development. 1 As emerging economies improve basic neonatal care, death due to traditional causes, including sepsis and perinatal asphyxia, have dramatically decreased. Therefore, CHD is being increasingly recognized. 2 The estimated incidence of CHD is 1% at birth, while CHD accounts for approximately one third of all infant deaths within the first year in China.3,4 However, the majority of patients with CHD fail to be diagnosed at the early stages after birth because of a lack of specific symptoms.5,6 This prevents infants from receiving effective surgical repair or palliation in a timely fashion. 7 Additionally, delayed diagnosis may lead to irreversible cardiovascular dysfunction and eventually death in children, which becomes a heavy medical and economic burden in society.8,9 Therefore, developing an effective tool for early detection of CHD is paramount for decreasing perinatal mortality caused by this disease.
At present, heart auscultation and echocardiography still play an important role in diagnosing CHD.10–13 However, there is still a sizeable proportion of patients with CHD who cannot be diagnosed by cardiac auscultation, which is an experience-dependent skill and is affected by many factors.14,15 Echocardiography, which is an indispensable tool for diagnosing CHD, is limited in clinical application in most basic medical institutions owing to its high cost, especially in developing countries. 16 More critically, there is an insufficient number of pediatric cardiologists or congenital cardiac sonographers who are experienced in performing a comprehensive cardiac ultrasound. 17 Pulse oximetry has been recommended as a reliable screening tool of CHD for newborns in a number of developed countries.18–21 Nevertheless, several recent pioneering studies have obtained an extremely high specificity, but only a moderate sensitivity, of pulse oximetry in detecting CHD.19,22–25 Therefore, a novel screening method with both high sensitivity and specificity for early screening of CHD is urgently required.
Information focusing on addition of pulse oximetry to auscultation as a screening method for CHD has not been extensively reported. Therefore, this study aimed to investigate whether pulse oximetry, in conjunction with cardiac auscultation, improves accuracy in neonatal CHD screening.
Methods
Study design
This retrospective, observational, screening study was conducted at the Second Affiliated Hospital of Wenzhou Medical University. Data were collected from July 2019 to January 2020. Written informed consent was obtained from the participating newborns’ parents. Ethical approval was gained from the Second Affiliated Hospital of Wenzhou Medical University Ethics Committee before performing the study (approval number: 2021-K-44-01).
Inclusion and exclusion criteria
As a prerequisite, enrollment of subjects was determined by the predefined inclusion and exclusion criteria as follows. (1) All asymptomatic neonates born by spontaneous vaginal delivery or cesarean section during July 2019 to January 2020 were included. (2) Newborns with prenatally diagnosed CHD were excluded from the current study. (3) Exclusion also occurred if screening information was missing and not able to be obtained from newborns of all gestations.
Measurements
Two modalities, including pulse oximetry and cardiac auscultation, were used in the primary screening of CHD in this study. These two examinations were performed in neonates aged between 6 and 72 hours. Taking into consideration that the auscultation result would be influenced by knowledge of a pulse oximetry test, cardiac auscultation was performed by the same clinician just before pulse oximetry measurement. Any newborn with the presence of any abnormal finding in the two screening methodologies was regarded as positive in screening. All newborns with positive screening results for CHD were referred to the Cardiology Department for echocardiography within 1 week of primary screening. For newborns who screened negative for CHD, a postpartum routine physical examination was carried out at 6 weeks of age. Neonates who showed symptoms of possible CHD (cyanosis, tachypnea, and feeding difficulty) or signs (heart murmurs) were supposed to have a further echocardiographic examination on the same day to confirm diagnosis of CHD. All neonates who were diagnosed with severe CHD by an echocardiographic examination were admitted to the Children’s Cardiovascular Center at the Second Affiliated Hospital of Wenzhou Medical University for further treatment.
Cardiac auscultation
One experienced pediatric cardiologist from The Second Affiliated Hospital of Wenzhou Medical University performed auscultation for each newborn during 6 to 72 hours after birth. Five areas (the pulmonic area, the aortic lobe area, Erb’s point, the tricuspid area, and the mitral area) were selected for detailed auscultation, with a standard pediatric stethoscope. Notably, auscultation only occurred when the newborns were under a quiet condition in the general maternity ward. After auscultation, any heart murmur (including transient murmur) that was grade II or higher was considered abnormal.
Pulse oximetry detection
Pulse oximetry detection of the newborn was performed by the same clinician immediately after cardiac auscultation using a PM-50 pulse-oximeter (Mindray, Shenzhen, China). The following pulse oximetry measurement criteria proposed by the American Academy of Pediatrics were used: 26 (1) the measurement was considered abnormal after a pulse oximeter oxygen saturation of <90% in the right hand and in either foot; and (2) newborns with an initial pulse oximeter oxygen saturation of 90% to 95% received a repeated pulse oximetry testing after 4 hours. The screening was also deemed abnormal when the pulse oximeter oxygen saturation reading remained <95% or the difference between the two repeated measurements was >3%. Neonates needed to be quiet during pulse oximetry testing to reduce the influence caused by crying or moving on the quality and accuracy of this test.
Determination of CHD
An echocardiographic examination was considered as the gold standard for diagnosis of CHD and was used to further determine the findings of primary screening. A clinician with expertise in echocardiography implemented echocardiographic scans for each neonate who was positively screened at the bedside within 1 week from initial screening using a Philips IE-33 Ultrasound Machine (Philips, Andover, MA, USA). Cardiac position, atrioventricular morphology, valve morphology, and the connection between valves and large blood vessels for each newborn were examined while they were sleeping. The diagnostic criteria used for CHD followed the international pediatric CHD code. 27
Statistical analysis
All statistical analyses were performed using IBM SPSS version 23.0 software (IBM Corp., Armonk, NY, USA). Standard descriptive statistics were used for quantitative data (mean and standard deviation) and categorical data (frequency and percentage). The screening rate, positive screening rate, positive diagnosis rate, prevalence, and different types of CHD were obtained in this study. Moreover, sensitivity, specificity, positive and negative predictive values, positive and negative likelihood ratios, and the diagnostic ratio were calculated for pulse oximetry alone, cardiac auscultation alone, and pulse oximetry plus cardiac auscultation. The relative operating characteristic curve for each screening method was depicted by Stata 12.0 software (StataCorp LP, College Station, TX, USA) and the area under the relative operating characteristic curve was calculated. The Student’s t-test or χ2 test was used to compare differences between two groups. A P value <0.05 was considered as statistically significant.
Results
Primary screening results and components of CHD
A total of 5409 live newborns were delivered in the Second Affiliated Hospital of Wenzhou Medical University from 1 July 2019 to 31 January 2020. Among all live births, the screening information from 2082 newborns was missing and could not be obtained owing to the errors in the clinical information recording system. Therefore, the remaining 3327 newborns were eventually enrolled in the current screening study. The screening rate of this study was 61.5%. Among these 3327 neonates, 312 (180 male and 132 female neonates) were positive, with a positive screening rate of 9.41%. The median age at pulse oximetry combined with cardiac auscultation was 28 hours (range: 6–72 hours). Of 312 positive neonates, 276 with an abnormal pulse oximetry result (pulse oximeter oxygen saturation was <90% in the right hand and in either foot) and 47 with heart murmur level II or higher were identified. All of these newborns were recommended to receive an echocardiographic examination in our hospital, but parents of 18 refused. A total of 139 neonates were diagnosed with CHD by an echocardiographic scan. The positive diagnostic rate was 47.3% (139/294) and the incidence of CHD was 4.2% (139/3327).
The distribution of diagnosed CHD in 139 newborns is shown in Table 1. A patent ductus arteriosus was the most prevalent CHD, followed by atrial septal defect, ventricular septal defect, atrioventricular septal defect, and one case each of tetralogy of Fallot, pulmonary atresia, and ventricular septal defect with double outlet of the right ventricle.
Distribution of different types of CHD screened in the study.

Most newborns had multiple CHDs spontaneously and only one major malformation was recorded.
CHD, congenital heart disease.
Accuracy of pulse oximetry combined with cardiac auscultation in screening for CHD
The accuracy of pulse oximetry plus cardiac auscultation was evaluated and compared with pulse oximetry and cardiac auscultation alone. Only 24 of 139 (17.3%) CHD cases were detected by cardiac auscultation alone and 90 of 139 (64.7%) CHD cases were screened by pulse oximetry alone (Table 2). Strikingly, pulse oximetry combined with cardiac auscultation as a novel screening method showed 125 of 139 CHD cases (89.9%), which significantly improved the sensitivity in screening CHD compared with simple pulse oximetry or cardiac auscultation alone (both P < 0.01) (Table 3). Furthermore, addition of cardiac auscultation to pulse oximetry remarkably reduced the false negative rate and negative likelihood ratio compared with pulse oximetry or auscultation alone (all P < 0.01). However, there was no significant difference in the specificity or negative predictive value among these three methods. More importantly, the diagnostic ratio of pulse oximetry plus cardiac auscultation was 169.0, which was significantly higher than that of pulse oximetry alone and cardiac auscultation alone (both P < 0.01). Additionally, the relative operating characteristic curve and the area under the relative operating characteristic curve were used to further evaluate the diagnostic value of the three screening methods (Figure 1 and Table 4). The area under the relative operating characteristic curve of pulse oximetry combined with cardiac auscultation screening was significantly larger than that of pulse oximetry alone and cardiac auscultation screening alone (both P < 0.01). Collectively, these results suggested considerable accuracy and value of this combined method in the diagnosis of CHD.
Baseline data of newborns who were screened for CHD with different methods.
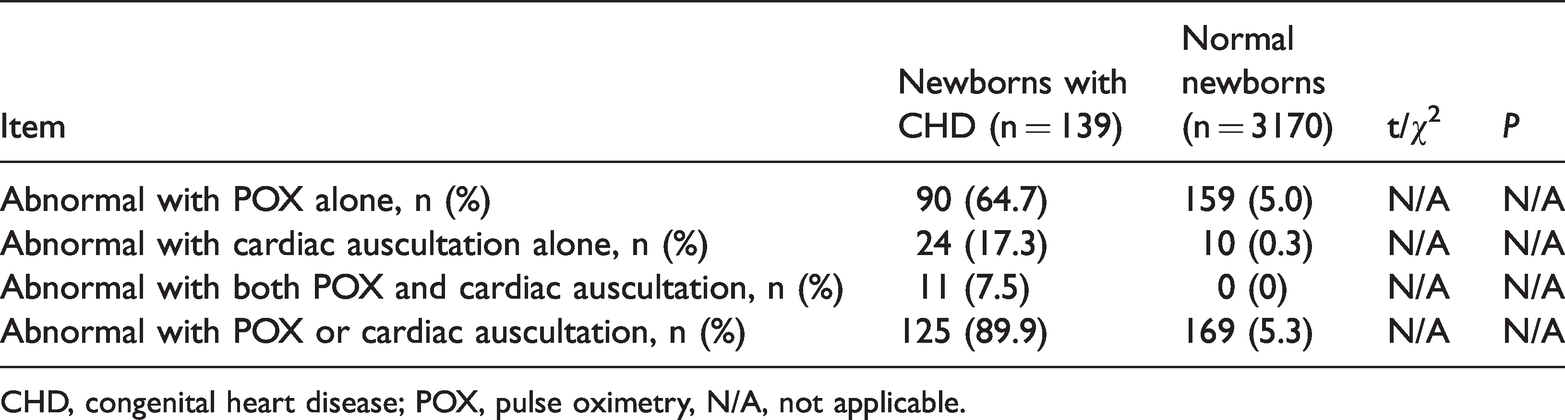
CHD, congenital heart disease; POX, pulse oximetry, N/A, not applicable.
Comparison of accuracy of diagnosing CHD by different screening modalities.
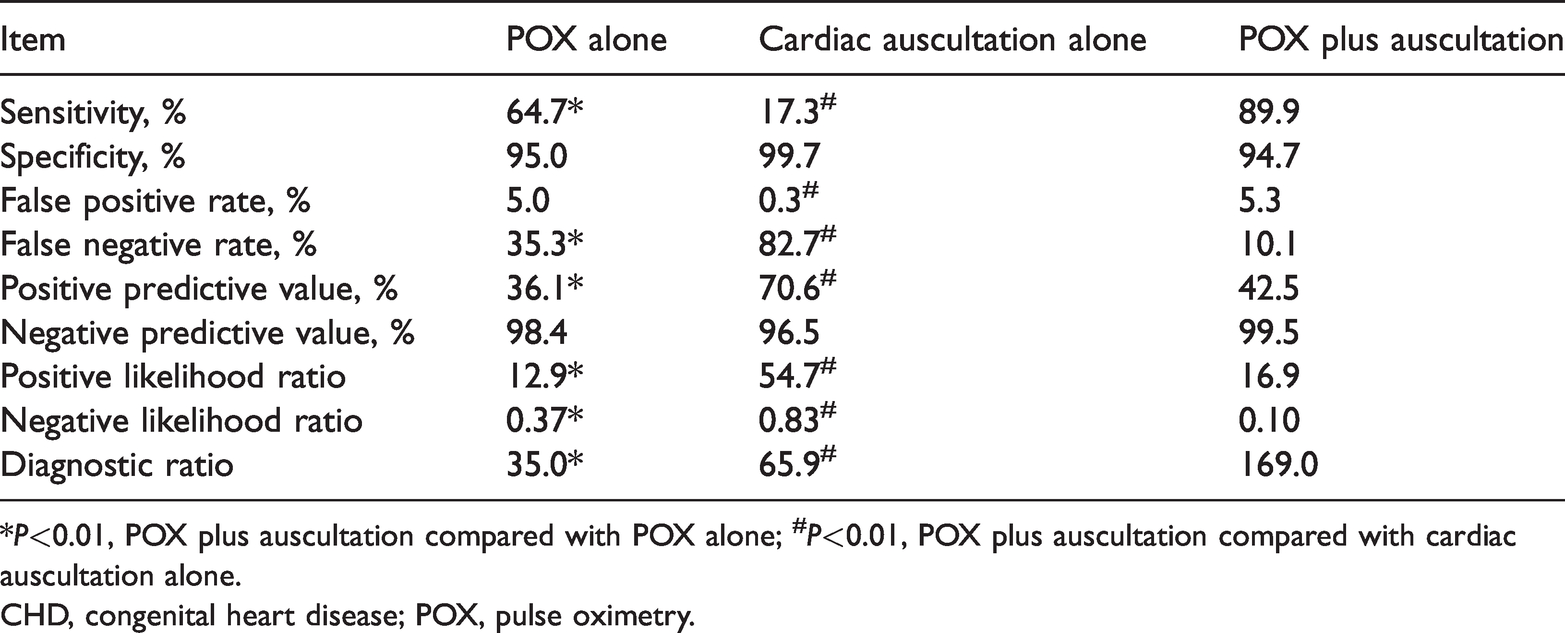
*P<0.01, POX plus auscultation compared with POX alone; #P<0.01, POX plus auscultation compared with cardiac auscultation alone.
CHD, congenital heart disease; POX, pulse oximetry.
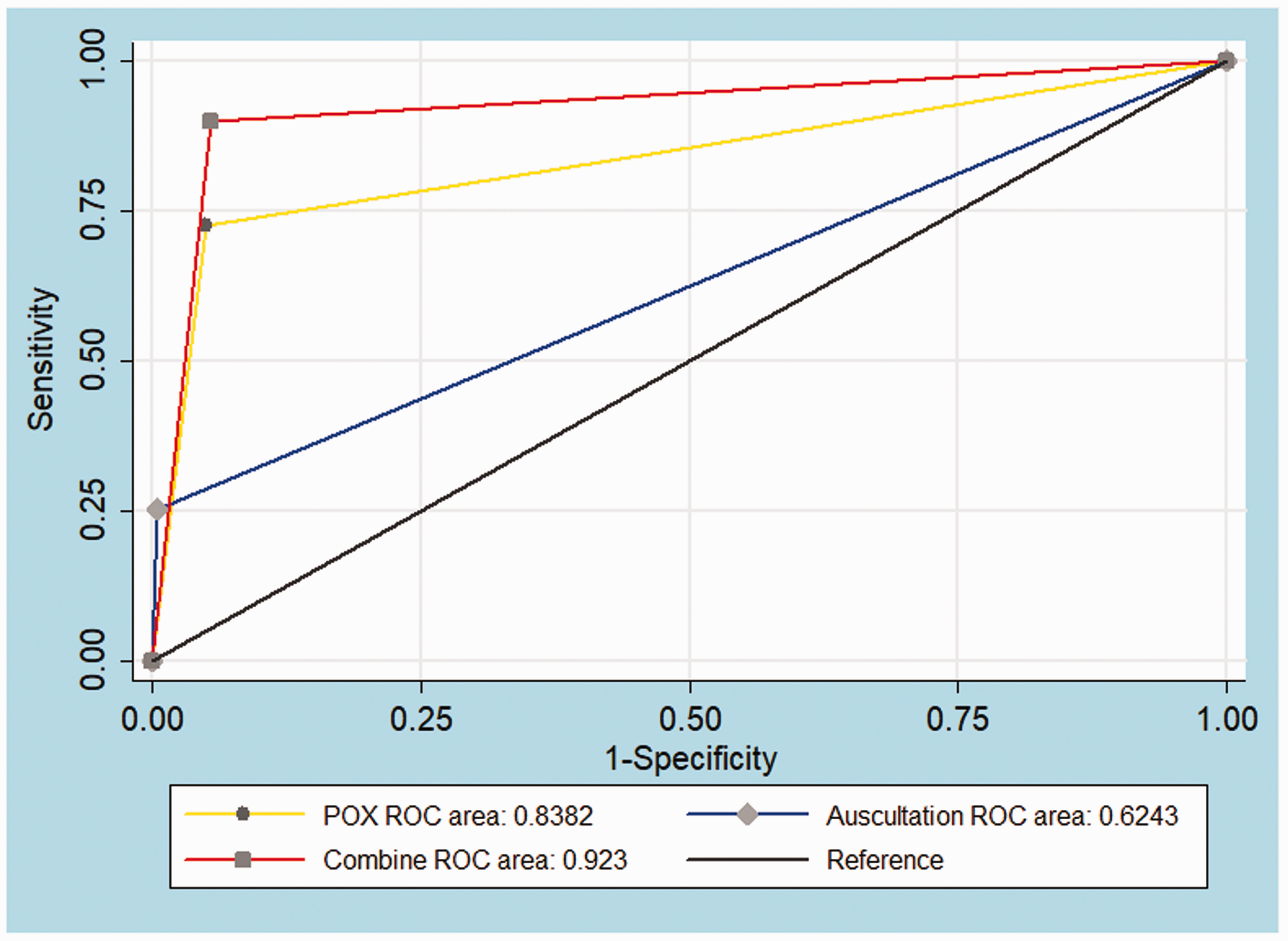
ROC curve of different methods in screening congenital heart disease.
Comparison of the AUC among the three screening methods.
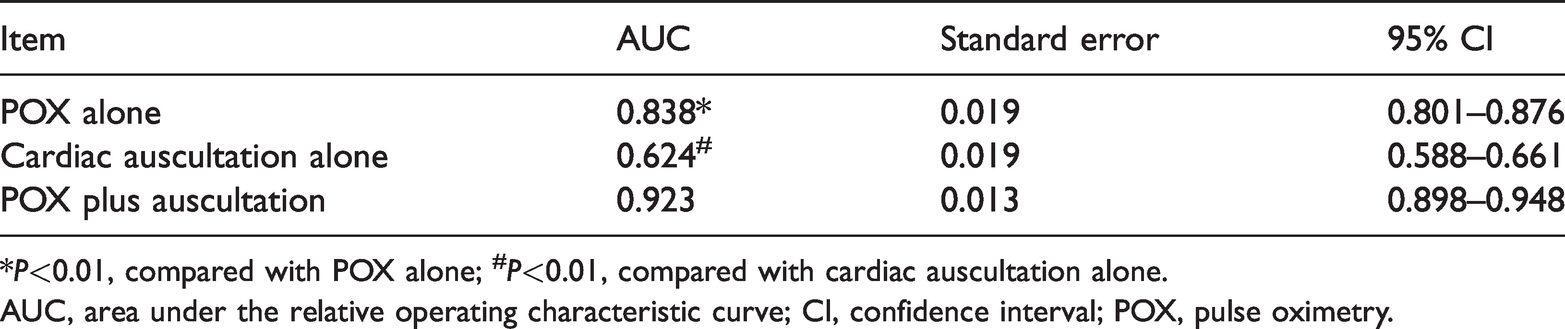
*P<0.01, compared with POX alone; #P<0.01, compared with cardiac auscultation alone.
AUC, area under the relative operating characteristic curve; CI, confidence interval; POX, pulse oximetry.
Discussion
Currently, delayed diagnosis of CHD in neonates is still a common problem worldwide, and CHD is a leading cause of infant death.7,28 Even in developed countries, approximately 13% to 48% of newborns with CHD leave hospital undiagnosed. 29 Additionally, approximately 10% to 30% of newborns who die from CHD do not have their condition diagnosed before autopsy.30,31 Cardiac auscultation is a routine examination for evaluating CHD in neonates after birth. 10 A heart murmur identified by auscultation may indicate critical CHD in some asymptomatic infants.14,32 Pulse oximetry is a non-invasive, cost-effective modality, which is easy to perform after basic training.33,34 However, most newborns with simple CHD (e.g., severe left heart obstructive lesions and large left-to-right shunt lesions) cannot be discerned by pulse oximetry at the early period of birth. 9 Strikingly, only infants with CHD and hypoxemia can be detected by pulse oximetry testing.9,35 Taken together, these previous findings and the current study suggested that the combination of pulse oximetry and neonatal cardiac auscultation was a useful screening method for detecting CHD.
Our study showed a low sensitivity (17.3%) and a high false negative rate (82.7%) of cardiac auscultation alone, which indicated that simple cardiac auscultation was not appropriate for CHD screening. In fact, the prevalence of heart murmur in neonates varies from 0.9% to 77.4%, depending on a series of factors, such as the examiner’s experience. 36 Even for an experienced pediatric cardiologist, accurately discerning a heart murmur during the early neonatal period is difficult.37,38 Therefore, clinicians need to improve the ability to distinguish a harmless murmur from a pathological murmur. Moreover, a novel sensitive method that will not be affected by different examiners in detecting CHD urgently needs to be developed.
Accumulated evidence has led to recommendation of using pulse oximetry testing with favorable outcomes for newborns to support identification of CHD.19,24,39,40 Our study showed only a moderate sensitivity (64.7%) of pulse oximetry alone, which is in accordance with some previous studies.19,22–25 This finding raises concerns regarding the feasibility and reliability of this method in screening CHD. Indeed, pulse oximetry has been used only in a small amount of Chinese hospitals to screen for CHD, especially in Shanghai, and also has not shown satisfactory screening accuracy alone. 41
To date, the accuracy and predictive value of addition of cardiac auscultation to pulse oximetry in cases of suspected CHD have been rarely reported. 41 Therefore, we conducted this pioneering study to evaluate the efficacy of pulse oximetry plus cardiac auscultation in screening CHD in neonates. We found that the combination of these two methods significantly improved the sensitivity and decreased the false negative rate compared with pulse oximetry alone and auscultation alone. Additionally, combination of these two methods also had a high and acceptable specificity. Furthermore, the combined screening method further reduced the negative likelihood ratio and increased the diagnostic ratio compared with either method alone. These findings suggest that this combined method is an accurate tool for early screening of CHD.
Limitations
One limitation to our study is that screening data for 2082 newborns were lost owing to errors in the clinical information recording system, which resulted in a screening rate of CHD of only 61.5%, which is lower than that in Shanghai (94.0%–99.8%). 41 Non-standardized data management of these newborns in our institute is the main reason for the low screening rate in our study. Therefore, several strategies, such as establishing a standardized clinical information system, should be implemented to improve the screening rate and stability in CHD screening.
Conclusion
Our study shows that pulse oximetry plus cardiac auscultation can be used as an accurate and feasible method for early screening of CHD in newborns, with encouraging results. More large-sample studies are still required to further clarify the applicable value of this combined method for detecting CHD.
Footnotes
Declaration of conflicting interest
The authors declare that there is no conflict of interest.
Funding
This work was supported by grants from the National Natural Science Foundation of China (Nos. 81771555 and 81471493). The study sponsors had no involvement in the collection, analysis, or interpretation of data, or in the writing of the manuscript.
Author contributions
Zhangye Xu, Guowei Wu, and Jiajia Song conceived and designed the study. Jiajia Song and Xianping Huang enrolled the subjects. Jiajia Song and Xianping Huang collected and analyzed the data. Shenzhi Zhao and Jiajia Chen prepared the figures and tables. Ruiheng Chen conducted cardiac auscultation and the pulse oximetry test. Jiajia Song and Xianping Huang prepared the manuscript. Zhangye Xu and Guowei Wu edited the manuscript. All authors read and approved the final manuscript.