
Abstract
Background. The antibiotic resistance patterns of young infants with urinary tract infections (UTIs) have evolved over the past 2 decades. Whether current empiric antibiotic regimens are sufficient in this age group is unknown. Methods. A retrospective review of patients aged 0 to 60 days admitted with a UTI discharge diagnosis. Results. Overall susceptibility to empiric antibiotics was 87%. Antibiotic resistance and length of stay were highest among those who were afebrile, those admitted to the intensive care unit, and those with culture diagnosis of enterococcal infection. The sensitivity and specificity of ultrasound as a screening tool for genitourinary anomaly was 70% and 40%, respectively, with a positive predictive value of 31.8%. Conclusions. Empiric antibiotic regimens cover a high percentage of UTIs in infants. However, high rates of resistance and prolonged length of stay in patients with enterococcal infection highlight the need for continued surveillance of such patients in this age group.
Introduction
Urinary tract infections (UTIs) are a major cause of serious bacterial infection (SBI) in young infants. 1 Recognizing UTI in young children remains difficult, as neonates and infants often have nonspecific signs of infection. In one study performed in North Carolina, UTI was the most common cause of SBI in young infants with fever without localizing signs. 2 American Academy of Pediatrics guidelines provide a recommended workup and treatment plan for patients 2 to 24 months of age. However, these guidelines do not address the management for infants less than 2 months of age.3,4 There is debate in the literature as to the epidemiology of UTIs in these patients as well as empiric treatment strategies.4-6 Recent evidence in febrile infants 0 to 90 days of age demonstrated differences among resistance patterns in this population. 6 A better understanding of the regional infectious causes of UTI and antimicrobial resistance in this population will aid the development of improved empiric treatment strategies. The objectives of the study were to (1) determine epidemiologic characteristics and clinical presentation of young infants less than 2 months of age with UTI and (2) determine the effectiveness of current empiric antibiotic regiments for UTI in this age group.
Methods
Study Design
A comprehensive retrospective chart review was performed on hospitalized pediatric patients 0 months to 6 months of age admitted to the North Carolina Children’s Hospital from January 1, 2002, through December 21, 2012. Patients were identified utilizing the Carolina Data Warehouse, which collects information on all patients admitted to the University of North Carolina Health Care System. Inclusion criteria included age criteria noted above and at least one of the following classifications: discharge diagnosis of UTI or discharge diagnosis of pyelonephritis similar to previously published studies.7-9 Community-acquired UTI was defined as patients with a positive urine culture collected ≤2 days of admission, while hospital-acquired UTI was defined as patients with a positive urine culture collected >2 days after admission. Empiric antibiotic coverage was defined as an antibiotic regimen received by patient prior to urine culture sensitivity results. Effectiveness of empiric antibiotic coverage was defined as empiric antibiotic regimen that included at least one antibiotic to which the isolate was listed as “sensitive” in the urine culture testing. The study was approved by the University of North Carolina Institutional Review Board (Study #13-1268).
Data Collection
Patients were identified utilizing the collected data of the Carolina Data Warehouse. On identification of potential patients, a retrospective chart review was performed on each patient to determine eligibility and collect information on study variables. Available historical and physical examination data, demographics, laboratory studies, imaging studies, pathology studies, hospital costs (defined as hospital charges), and billing information were reviewed for each patient.
Statistical Analyses
We used χ2 tests to describe differences in demographics, diagnostic testing conducted, and laboratory values, by age and location (hospital floor versus intensive care unit [ICU]). Analyses were conducted using R 3.3 and the survey 3.31 package.10,11
Results
Study Demographics
We identified 103 patients who met inclusion criteria and were included in the study. All cases met our criterion for community-acquired UTI. Ages ranged from 0 to 60 days with a mean age on admission of 35 days. Patients identified primarily as Hispanic (32%), Caucasian (32.0%), or African American (19.4%). Males comprised 70.9% of the total cohort and were the majority regardless of race or ethnicity. Gender distribution varied significantly by race, with 85.3% of Hispanic patients identified as male in comparison to just 54.5% of Caucasians. Complete demographic information is listed in Table 1.
Demographic Characteristics by Age of Infants With UTI.

Abbreviations: UTI, urinary tract infection; ICU, intensive care unit.
Temperature Characteristics
On admission, 24 (23.3%) patients had an abnormal temperature, including 4 neonates noted to be hypothermic. The majority (66.0%) were afebrile. History of fever was reported for 45.6% of patients, with fever duration ranging from 1 to 5 days. Among patients who were afebrile on admission, 34.7% had a fever before admission, while 90% of patients febrile on admission also had a prior fever history. The majority (75.7%) of patients were admitted to the general pediatric unit with the remaining managed either in pediatric ICU or neonatal ICU. None of the patients admitted to ICU-level care were febrile on admission, though one neonate had a 1-day history of fever prior to presentation. Nineteen (18.4%) patients were admitted after transfer from another facility, and fever status for each was reported at time of initial presentation prior to transfer.
Laboratory and Imaging Evaluation
Diagnostic evaluation was similar across the cohort regardless of age, location (ICU vs non-ICU), or fever status. Urine culture was sent for all patients and blood cultures obtained in a majority (93.2%). Lumbar puncture and cerebrospinal fluid studies were significantly more likely in patients presenting with fever (80%, P = .013) with no difference noted by age (58.5% neonates, 48.3% young infants). Patients admitted to intensive care were more likely to have one or more subspecialty consults (92%, P < .001). Laboratory values were largely unremarkable with no significant findings across any groups.
All patients had some form of imaging done, with radiographs, ultrasound, and voiding cystourethrogram (VCUG) performed at similar rates across all groups (Table 2). Renal and bladder ultrasound (RBUS) was obtained in 90.3% of patients and VCUG in 70.9%. The majority (63.4%) of ultrasounds obtained were abnormal across all patient groups, with the hydronephrosis and pelviectasis identified as the most common abnormalities. Results did not predict subsequent imaging with VCUG, which was obtained after normal ultrasound in 76.5% of cases and in 74.6% with abnormal findings. The sensitivity and specificity of ultrasound as a screening tool for genitourinary anomaly was 70% and 40%, respectively, with a positive predictive value of 31.8%.
Resource Use by Age, Fever, and Hospital Location.
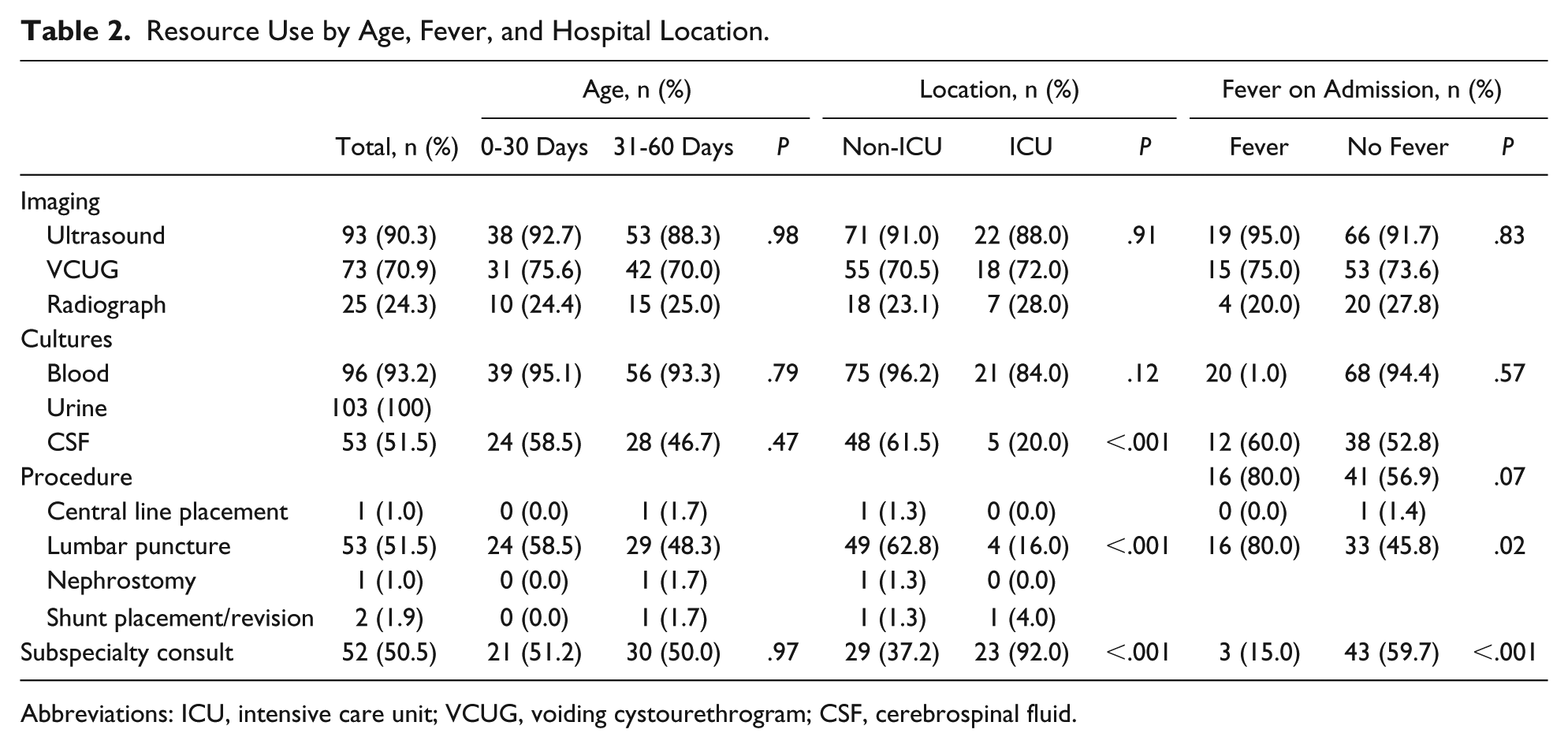
Abbreviations: ICU, intensive care unit; VCUG, voiding cystourethrogram; CSF, cerebrospinal fluid.
Efficacy of Empiric Treatment
Escherichia coli was the most common pathogen identified across all groups, with the exception of patients managed in an intensive care setting. Urine culture results by pathogen are listed in Table 3. E coli UTI was diagnosed in a majority (60%) of patients presenting with fever; however, results were not statistically significant (P = .07). Empiric antibiotic choice demonstrated organism susceptibility in 87.6% of cases, with highest resistance noted among Enterococcus (26.7%) and Klebsiella (14.3%) species (Figure 1). Nearly all (91.4%) E coli species were susceptible to empiric treatment choice. Empiric antibiotic treatment with ampicillin and gentamicin in combination was significantly more likely in neonates than young infants (P = .04), with both ampicillin and gentamicin identified as the most commonly used empiric antibiotic choice (either alone, together, or in combination with another antibiotic) across all groups. Ampicillin and cefotaxime was the second most common antibiotic combination.
Urine Culture Results by Age and Inpatient Location.

Abbreviation: ICU, intensive care unit.
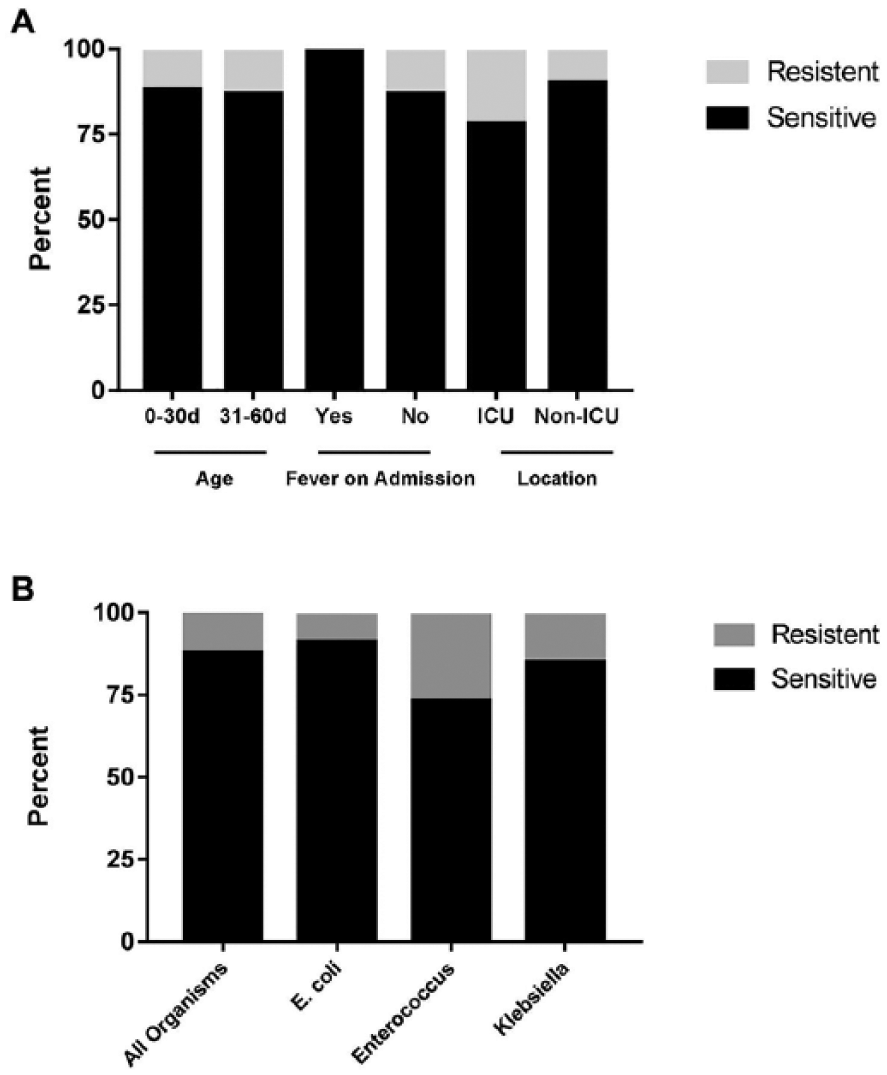
Efficacy of empiric antibiotic treatment.
Length of Stay
Length of stay (LOS) ranged from 4 to 272 days in our cohort, with significantly longer admissions for patients who were afebrile at presentation (30.48 ± 5.32 vs 3.82 ± 0.77, P = .01) and those admitted to ICU (85.13 ± 13.66 vs 9.99 ± 1.74, P < .001; Figure 2A). There was significant variability in length of hospital stay by pathogen (Figure 2B). Cases of E coli UTI had the shortest hospital course when compared with cases of Klebsiella and Enterococcus, with a significant difference noted when compared with Enterococcus species specifically (P = .01).

Length of stay by (A) clinical characteristics and (B) pathogen. Mean values of standard error reported (*P < .05, ***P < .001).
Discussion
In this retrospective analysis of young infants 0 to 60 days of age hospitalized with UTI, there are 3 main findings. First, overall effectiveness of empiric antibiotic regimens remains high for a large majority of infants with UTIs despite changing resistance patterns of urinary tracts pathogens. A caveat is that 12.4% of organisms demonstrated resistance to empiric antibiotic regimens. Second, there were differences in hospital LOS based on both clinical characteristics and pathogen source of UTI. Finally, this study corroborates previous reports of the limited predictive value of RBUS in infants with UTI.12,13
The etiology and clinical characteristics of young febrile infants has changed over the previous 2 decades. 2 Antibiotic resistance is a growing concern in the treatment of neonates and young infants with presumed SBI. 6 Despite evolving resistance patterns to UTI, susceptibility to empiric treatment remained very high across all clinical groups.6,14 Our findings of satisfactory empiric coverage of young infants with UTIs mirror those of febrile infants and infants with febrile UTI <90 days of age. 6
Enterococcus UTI, compared with other pathogens, was associated with increased resistance rate to first-line antibiotics and prolonged hospital stay. 15 Previous studies have demonstrated the significant differences between Enterococcus and gram-negative pathogens in febrile infants, including differences in gestational age, resistance patterns, pyuria, and urinary tract abnormalities.6,14,16,17 Our findings of variation in LOS compared with gram-negative pathogens substantiates previous findings differences in clinical course of Enterococcus UTIs. 16
The utility of RBUS to predict clinically significant genitourinary tract anomalies by subsequent VCUG is an ongoing discussion with wide variability reported in the literature.12,13 Our data reflect similar sensitivity and specificity of RBUS in predicting subsequent abnormal VCUG compared with infants 0 to 90 days of age. 12 These findings are consistent with the recent 2016 American Academy of Pediatrics recommendations that ultrasound and VCUG should be obtained in all infants aged 2 to 24 months diagnosed with a UTI. 4
There are limitations inherent to this type of retrospective study. First, this is a single-center study and our data may be influenced by local disease prevalence, which may not be generalizable to other geographic regions. We identified eligible patients on the basis of a diagnosis of UTI. Miscoding or erroneous diagnosis may limit the identification of patients. For example, it is possible that patients with sepsis due to UTI were misclassified as sepsis without a UTI diagnosis. We attempted to evaluate hospital outcomes using LOS. While this is a commonly used inpatient measure, it is possible that patients LOS may be more reflective of, for example, their hospital complications, than from the original UTI. Finally, our study is limited to hospitalized patients and may not be fully generalizable to outpatient UTI workups. Despite these limitations, out study provides evidence as to the etiology and clinical characteristics of UTI in young infants.
Conclusions
Empiric antibiotic regimens cover a high percentage of UTIs in infants. High rates of resistance and prolonged LOS in patients with Enterococcus highlight the need for identification and continued surveillance of such patients in this age group.
Footnotes
Author Contributions
JWA conceptualized and designed the study, interpreted the results, and drafted the initial manuscript. EHM obtained and interpeted data. PJR and AS performed data analysis and critically reviewed the manuscript. JAL designed the study, interpreted the results, critically reviewed the manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.