
Abstract
The usage of prophylactic oral antibiotics following distal hypospadias repair with stenting has been recently challenged. This study evaluated the incidence of symptomatic urinary tract infections (UTIs) following stented, distal hypospadias repair and the impact of prophylactic antibiotic therapy. Subjects 0 to 5 years of age with distal hypospadias were randomized to either Group 1 (antibiotics) or Group 2 (no prophylactic therapy). Urinalysis/urine culture was obtained intraoperatively with no preoperative antibiotics given. Phone interviews at 1 month and 3 months after surgery were done. Forty-eight patients were successfully randomized to either Group 1 (24) or Group 2 (24). The incidence of symptomatic UTI in this pilot study is low, and prophylactic antibiotic therapy does not appear to lower the incidence of symptomatic UTI. A larger, randomized, multicenter trial is needed to determine whether antibiotic prophylaxis reduces the risk of symptomatic UTIs following stented, distal hypospadias repair.
Introduction
Surgical correction of distal hypospadias often includes temporary postoperative urinary stent drainage. Because of concern over postoperative urinary tract infection (UTI), the majority of pediatric urologists administer prophylactic antibiotics after hypospadias repair while the postoperative urethral stent is in place. 1 This practice is based on previous studies that have demonstrated decreased bacteriuria in patients who were treated with prophylactic antibiotics. 2 However, the increased likelihood of bacteriuria in these patients was not well correlated with symptoms suggestive of UTI. It has since been established that bacteriuria is a common finding in catheterized children and is also found in healthy noncatheterized children.1,3,4 Treating asymptomatic bacteriuria has been called into question recently as well.5,6 The disadvantages of antibiotic use in this setting include antibiotic resistance, adverse drug reactions, and increased cost.
Kanaroglou et al 7 retrospectively examined the role of prophylactic antibiotics in this setting by comparing the incidence of symptomatic UTI in patients receiving antibiotics with those who did not. No symptomatic UTIs were observed in either the antibiotic prophylaxis (78) or the antibiotic-sparing group (71), with urine cultures obtained only when symptoms of UTI manifested.
In light of the question of whether postoperative antibiotic therapy is beneficial during urethral stenting after distal hypospadias repair, we conducted a randomized controlled trial to assess the incidence of symptomatic UTI in patients with urethral stent drainage following distal hypospadias repair and to determine whether the incidence of symptomatic UTI is affected by prophylactic antibiotic usage.
Materials and Methods
Institutional review board approval and intramural grant funding were obtained for this prospective study of male subjects undergoing primary hypospadias repair with open urethral stent drainage for distal penile, coronal, or balanic hypospadias. Patients were randomly assigned to 1 of 2 groups: an antibiotic prophylaxis cohort (Group 1) or an antibiotic-sparing cohort (Group 2). All potential patients between January 2015 and February 2017 were screened and recruited for enrollment. Males undergoing fistula repair, glanular hypospadias repair without open incontinent urethral stent drainage, or proximal hypospadias repair were excluded from the study.
For all patients studied, a urinalysis and a urine culture were obtained on initiation of their surgical procedure to rule out underlying bacteriuria or UTI. No antibiotic prophylaxis was given at the time of surgery for either cohort. Standard distal hypospadias repair was performed with urethral stent drainage into a single diaper postoperatively. Patients randomized to the antibiotic prophylaxis group received sulfamethoxazole/trimethoprim (2 mg/kg of trimethoprim daily) unless a sulfa allergy was present, in which case nitrofurantoin or cephalexin prophylaxis was alternatively administered.
Follow-up urine cultures were obtained for only patients with clinical symptoms suggestive of a UTI (ie, fever, dysuria, hematuria, or abdominal pain). UTI was defined as described in the American Academy of Pediatrics Workup of Febrile UTIs: the presence of pyuria and at least 50 000 colon-forming units per mL of a single uropathogen in an appropriately collected urine specimen. 8 For all patients with a positive urine culture following presenting symptoms, antibiotics were administered.
Patients in both groups were reevaluated in person at the time of urethral stent removal 5 to 8 days after surgery. Interval assessment of participating patients for symptoms of symptomatic UTI or other problems was performed 1 month after surgery by the research nurse in our team. Patients were reevaluated again in the clinic 3 months after hypospadias repair.
The primary endpoint of this study was the presence of symptomatic UTI within 30 days of surgery. Secondary endpoints evaluated included surgical site infections (SSIs) and complications of hypospadias repair (urethral fistula, meatal stenosis, dehiscence, and diverticulum).
In order to eliminate bias in group assignment while producing groups of the same size, this study used a randomized, permuted block scheme in a 1:1 allocation stratified by 2 age group (≤2.5 years of age and >2.5 years of age). Using the block randomization procedures, a subject was assigned to a study group by computer using the Research Electronic Data Capture REDCap randomization module. 9 Descriptive statistics included standard measures of central tendency (mean, median) and variability (standard deviation, first and third quartiles) for continuous data, and frequencies and percentages for categorical variables. The primary aim of this study is to assess the prevalence of symptomatic UTI in subjects receiving standard of care dispensation of prophylaxis versus subjects selected to an antibiotic-sparing group. The primary outcome is defined as a binary outcome, the presence of symptomatic UTI (yes/no) within 30 days of surgery. Association between the primary outcome and all clinical and demographic variables were performed using Wilcoxon rank-sum test for continuous variables, and χ2 test for categorical variables. All analyses were completed using R version 3.4.0 (R Foundation for Statistical Computing, Vienna, Austria).
Results
Two hundred, seventy-eight consecutive, potential patients were screened with 90 eligible candidates identified. Eighteen patients were not enrolled due to one of the following reasons: simultaneous antibiotic therapy for preoperative nonurologic illness (5), operative procedure on research staff holiday (6), or prior intraoperative antibiotic therapy before consent (7). Of the remaining 72 patients (Figure 1), 11 families refused participation citing concerns over usage of antibiotic therapy, and 11 patients were consented but excluded from the analysis due to the following: intraoperative recognition of proximal hypospadias (1), positive urine culture at the time of the procedure (1), concordant treatment of otitis media with antibiotic therapy within the 30 day period (5), inadvertent treatment with intraoperative prophylactic antibiotic therapy (2), or lack of collection of intraoperative urinalysis/urine culture (2). All of the remaining 50 patients were randomized to either Group 1, the antibiotic prophylaxis cohort (24), or Group 2, the antibiotic-sparing cohort (24). Two additional patients were excluded from the analysis due to postoperative antibiotic treatment for SSI by their primary care provider within the 30-day period. Of note, both the patients treated for SSI by their primary care provider demonstrated no sign of SSI or other symptoms at the time of stent removal, and both these patients were randomized to Group 1 with antibiotic prophylaxis administered postoperatively. The remaining 48 patients successfully completed the protocol and were analyzed.
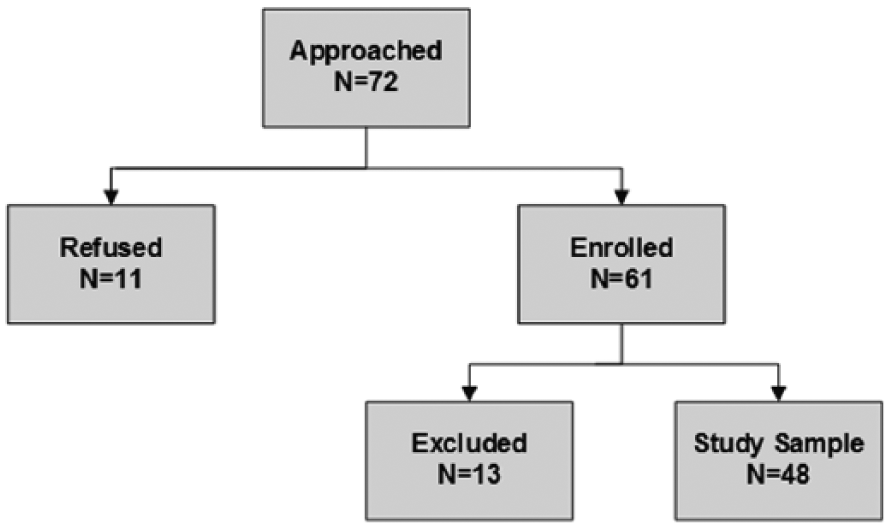
Chart delineating enrollment.
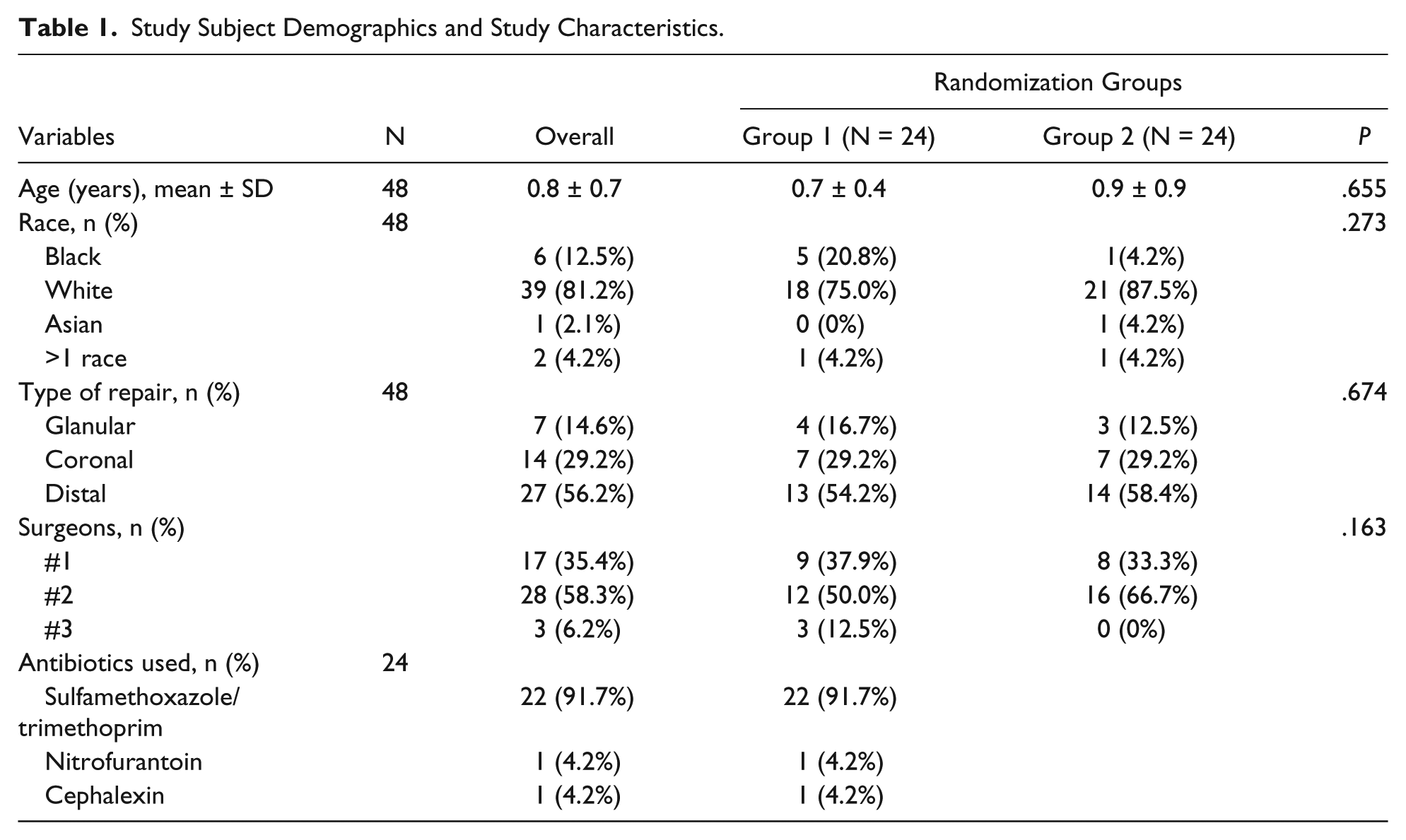
The average age for the 2 cohorts was comparable: 0.9 and 0.7 years (antibiotics; P = .66), and there was no difference in ethnicity or location of the patient’s urethral meatus (Table 1). The majority (22/24, 91.7%) of patients in Group 1 received sulfamethoxazole/trimethoprim.
Study Subject Demographics and Study Characteristics.
The average number of days of urethral stenting was comparable in both groups: 7.1 (Group 1) versus 7.9 days (Group 2) (P = .126, Table 2). There was no difference observed in the prevalence of symptomatic UTI between the 2 groups with a single patient in Group 1 diagnosed and treated for a morganilla morganii UTI. No patient in either group was observed to have symptoms of SSI by our team. No patient in either cohort was found to have dysuria, hematuria, obstructive symptoms, or unexplained fevers within their 3- to 6-month follow-up. There was no difference in total complications of hypospadias repair for Group 1 (2) versus Group 2 (3) (P = .796). Complications for Group 1 consisted of urethrocutaneous fistula (1) and glans dehiscence (1), while Group 2 complications included meatal stenosis (1), urethrocutaneous fistula (1), and glans dehiscence (1).
Study Findings Regarding Stent Removal Visit, 30-Day End Point, and Follow-up.
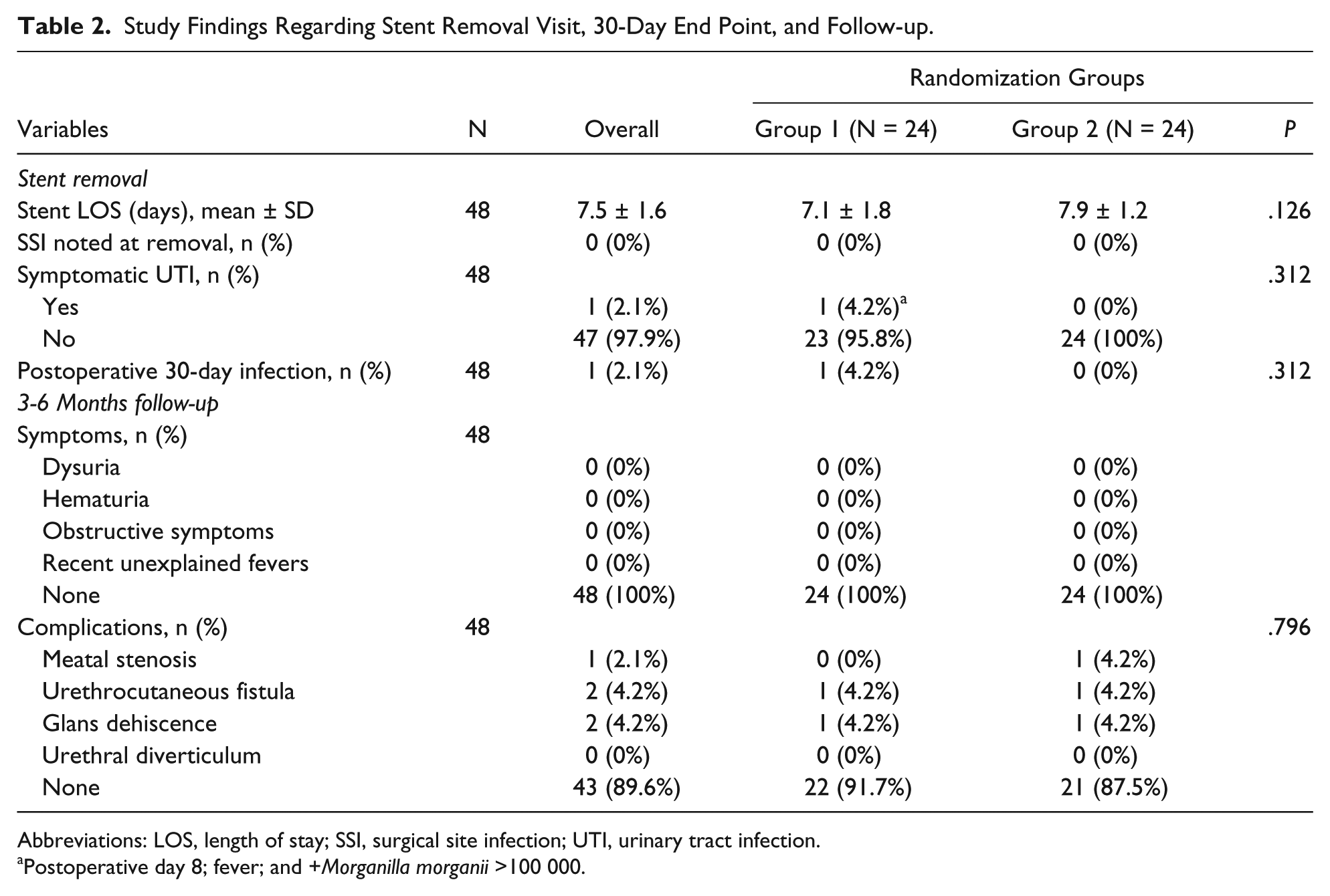
Abbreviations: LOS, length of stay; SSI, surgical site infection; UTI, urinary tract infection.
Postoperative day 8; fever; and +Morganilla morganii >100 000.
Discussion
Antibiotic resistance is a growing problem in the practice of pediatric urology with increased resistance to multiple antibiotics typically used for uropathogens. 10 Recent attention has been directed toward improving understanding of the benefits of antibiotic prophylaxis in the management of pediatric urologic diseases, such as vesicoureteral reflux and prenatal hydronephrosis. However, despite preliminary evidence questioning the utilization of antibiotic therapy both before and after stented, distal hypospadias repair,7,11,12 the majority of pediatric urologists continue to administer antibiotics in conjunction with hypospadias repair. 1 Since hypospadias is one of the most common congenital anomalies with an incidence from 0.3% to 0.7% in live male births, 13 overutilization of perioperative antibiotic therapy with hypospadias repair could potentially affect up to 10 000 boys born in the United States per year. 14
Shohet et al 2 first demonstrated the benefit of reduction of bacteriuria following stented hypospadias repair in 1983. Since that time, standard practice following stented hypospadias repair has included prophylactic antibiotic therapy for the duration of urethral stenting. With the recent concern of overutilization of antibiotic therapy, many have begun to question the necessity of antibiotic therapy with distal hypospadias repair. Kanaroglou and colleagues 7 reviewed their experience of stented hypospadias repair by a single surgeon of 149 consecutive patients with 78 given oral prophylactic therapy during urethral stenting and 71 treated without antibiotics. All patients in this series received 1 dose of preoperative cefazolin or an alternative antibiotic if a medicine allergy was present. The primary endpoint was the observation of symptomatic UTIs rather than bacteriuria, and secondary endpoints included complications of hypospadias repair and SSIs. No culture proven, symptomatic UTIs occurred in either group; however, a single patient was treated for SSI with antibiotics by his pediatrician. While this study was indeed provocative, the analysis was retrospective in nature and included both reoperative and proximal hypospadias patients.
Two randomized, prospective series have assessed the prevalence of symptomatic UTIs after stented, hypospadias repair. Meir et al 15 published a series that examined 101 boys undergoing tubularized incised plate urethroplasty with urethral catheter placement during a 16-month period who were all given cefonicid prior to surgery with subsequent randomization to an antibiotic prophylaxis or a nontreatment group. They observed a similar reduction in bacteriuria in the antibiotic prophylaxis group (11/52, 21%) as compared with the nontreatment group (25/49, 51%). They also observed a significantly higher rate of “complicated UTIs,” defined by temperature greater than 38.5°C in the nontreatment group (12/49, 24.5%) as compared with the antibiotic prophylaxis group (3/52, 5.8%; P < .05). No other additional detail of the symptoms experienced was reported though. 15
Roth et al also presented a prospective series of 50 consecutive patients randomized to antibiotic prophylaxis or nontreatment in 2016 (presented at the 2016 Society for Pediatric Urology meeting in San Diego, CA). While the primary endpoint was presence of bacteriuria at the first postoperative visit, they also evaluated presence of UTI defined as presence of fever, fussiness, or other symptoms with >50 000 colon-forming units of bacteria along with the rate of postoperative complications. Although this study has not yet been published, their group reported a similar rate of increased bacteriuria in the nontreatment group with 12/16 (75%) versus 2/22 (9%) in the antibiotics group (P < .001). However, contrary to the results reported by Meir et al, 15 they also noted that no patients experienced symptomatic UTIs in either group. Their description of such a symptomatic UTI was more detailed than that of Meir et al 15 with a prevalence of symptomatic UTI consistent with findings of both Kanaroglou et al 7 and our findings.
Our study represents the first prospective, randomized study published demonstrating no difference in the prevalence of symptomatic UTIs after stented, distal hypospadias repair (P = .312). Important distinctions between our series and others reported include the following: (1) this study consisted of only patients with distal hypospadias repair and (2) no patients received preoperative, empiric antibiotic therapy prior to surgery. All of the other series evaluating the utilization of postprocedural antibiotic prophylaxis included patients with more severe, proximal hypospadias7,15 and were given preoperative antibiotic therapy. Since we believe there may be a higher risk for SSI in more proximal hypospadias, we excluded patients with proximal hypospadias. Furthermore, evidence exists that preoperative antibiotic therapy is not beneficial for many routine wound class 1 pediatric urologic surgical procedures in reduction of SSIs. 16 Since we question whether distal hypospadias repair is truly a wound class 2 procedure, one surgeon at our institution discontinued administration of preoperative antibiotic therapy for distal hypospadias several years ago and has reported no increased risk for SSI in a small subset of patients treated without antibiotics before or after surgery. 12
Although practice patterns may have changed in the past few years since pediatric urologists were last surveyed, the majority of pediatric urologists administer prophylactic antibiotics after hypospadias repair while the postoperative urethral stent is in place. 1 We hypothesize that fear among surgeons significantly influences the reluctance to discontinue antibiotic utilization despite the lack of evidence of increased hypospadias complications for patients not given postoperative in multiple series.7,15 Our study provides further evidence that there appears to be no increase in hypospadias complication in patients treated without antibiotic therapy both before and after the procedure (P = .796).
Even though this study was a grant-funded, prospective, randomized study, we experienced challenges leading to some limitations of the study. Recruitment and execution of the study were challenges as evidenced by the number of patients excluded from consideration and the number of protocol violations leading to exclusion. Family concern of overutilization of antibiotic therapy appeared to be a driver in their reluctance to participate in the study. Some variability in success of patient recruitment of patients per surgeon for the study was a factor as well. We believe that all of these factors are a function of the cultural overreliance on antibiotics and the difficulty to enact change in practice patterns for antibiotic utilization. Given these challenges and the low rates of infection and hypospadias repair complications, a large, randomized multicenter, prospective study would be beneficial to broaden our understanding.
Conclusion
The prevalence of symptomatic UTI following stented, distal hypospadias repair in this pilot study is low, and prophylactic antibiotic therapy following this procedure does not appear to lower the prevalence of symptomatic UTI. A larger, randomized, multicenter trial is needed to determine whether antibiotic prophylaxis reduces the risk of symptomatic UTIs following stented, distal hypospadias repair.
Footnotes
Author Contributions
SC: Contributed to conception and design; contributed to acquisition, analysis, and interpretation; drafted manuscript; critically revised manuscript; gave final approval; agrees to be accountable for all aspects of work ensuring integrity and accuracy.
MKM: Contributed to interpretation; critically revised manuscript; gave final approval; agrees to be accountable for all aspects of work ensuring integrity and accuracy.
AC: Contributed to interpretation; critically revised manuscript; gave final approval; agrees to be accountable for all aspects of work ensuring integrity and accuracy.
AP: Contributed to conception and design; contributed to acquisition; critically revised manuscript; gave final approval; agrees to be accountable for all aspects of work ensuring integrity and accuracy.
IZ: Contributed to conception and design; contributed to acquisition; critically revised manuscript; gave final approval; agrees to be accountable for all aspects of work ensuring integrity and accuracy.
SB: Contributed to design; contributed to acquisition, analysis, and interpretation; drafted manuscript; critically revised manuscript; gave final approval; agrees to be accountable for all aspects of work ensuring integrity and accuracy.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The Children’s University Medical Group intramural grant.