
Abstract
There is variability in practice among care providers on feeding infants admitted with neonatal hypoglycemia (NH) for parenteral dextrose. We compared clinical outcomes in infants who were fed (NH-Fed) and hypoglycemic infants who were kept nothing per os (NPO) (NH-NPO) at the time of initiation of intravenous (IV) dextrose. We performed a retrospective review of all newborn infants admitted to the neonatal intensive care unit with NH for IV dextrose. Infants were grouped as per the feeding approach at initiation of IV dextrose: NH-Fed or NH-NPO infants. We found that infants in the NH-Fed group had lower maximum glucose infusion rate, less duration of glucose infusion therapy compared with the NH-NPO group, and significantly less number of days of hospital stay compared with the NH-NPO group (5.87 ± 1.4 days vs 4.9 ± 1.4 days, P < .006). In conclusion, feeding infants with hypoglycemia who require IV dextrose offers tangible benefits of shorter duration of parenteral dextrose and shorter length of hospitalization.
Introduction
Although hypoglycemia in the newborn infant is one of the most common diagnosis in infants, admitted to the neonatal intensive care unit (NICU), one cannot identify a specific concentration or range of plasma glucose concentration that defines significant hypoglycemia.1,2 The numerical definition of neonatal hypoglycemia (NH) and the glucose levels that will result in long-term neurological and developmental consequences are still not clear.3-6 Operational threshold values are useful guidelines for clinicians to take appropriate actions. 1 Hence, American Academy of Pediatrics recommends using the glucose level of 2.6 mmol/L (47 mg/dL) as a level at which interventions are needed to improve blood glucose (BG) level in infants. 7
Majority of infants with low BG levels after birth have either transient dysregulation or an increase in insulin secretion that normalizes over time. 8 The treatment strategy for NH takes into consideration factors such as symptomatic hypoglycemia and whether it is transient or persistent.6,9,10 Although unit-specific protocols exist in managing hypoglycemia, the management of transient hypoglycemia usually follows a sequential pattern of feeding followed by dextrose gel and intravenous (IV) glucose infusion for progressive worsening or no improvement in BG concentrations in these infants.
Interventions such as oral dextrose gel supplemented with feeds has been shown to be more effective than feeds alone in the management of asymptomatic hypoglycemia in term and late preterm neonates. 11 Infants who remain hypoglycemic (BG <47 mg/dL) despite dextrose gel therapy and enteral feeding are candidates for parenteral glucose infusion. Glucose infusion is started at a rate of 4 to 8 mg/kg/min with a goal of maintaining plasma glucose levels above 50 mg/dL 12 ; glucose infusion rates (GIRs) are titrated to maintain glucose levels >50 mg/dL with frequent monitoring. Feeding approaches at initiation of the IV glucose infusion generally varies between centers; one approach advocates for no feeds until the BG levels are stable to avoid hormonal stimulation.13,14 The other approach recommends to continue the feeding schedule while starting the IV dextrose fluid.15,16 In our facility, it is at individual provider discretion to decide which approach to follow. This has allowed us the opportunity to compare clinical outcomes between the infants with different feeding approaches at the initiation of IV dextrose fluid therapy for NH.
Methodology
An observational retrospective chart review of infants admitted to two NICUs at Women and Children’s Hospital of Buffalo and Millard Fillmore Suburban Hospital with diagnosis of NH for IV glucose infusion from January 2015 to July 2018 was performed. This study was approved by the University at Buffalo Institutional Review Board Committee (Approval Number: 00002810). The committee agreed to waive the need for informed consent for this observational study. Only infants with gestational age >35 weeks with the diagnosis of NH were included in the study. Exclusion criteria were other medical, social, or surgical diagnosis that could result in longer hospital stay, infants who were small for gestational age (SGA) or intrauterine growth restricted, infants with persistent or congenital hyperinsulinemia, and infants who were admitted and did not receive IV dextrose therapy for hypoglycemia.
Infants were classified into 2 groups: infants who were kept nothing per os (NPO) until BG levels were above 47 mg/dL for 3 BG levels checked every 3 hours after starting IV dextrose therapy and infants who were allowed to feed at initiation of IV dextrose therapy.
Both the NICUs follow the same protocol for admission of infants to the unit with the diagnosis of NH. All asymptomatic infants with risk factors such as <37 weeks, SGA, large for gestational age, maternal diabetes of any type, Cord pH < 7.10 or base excess of <−10, axillary temperature <36°C, maternal use of β-blockers, β-sympathomimetic, or oral hypoglycemic medications were screened with NH protocol. 11 Infants with low BG level of <47 mg/dL despite feeding (attempts made to breastfeed initially, then to provide pumped breast milk or supplemental formula based on parental preference) were supplemented with a maximum of 3 dextrose gels (611 mg) each administered every 1 hour until stable BG level was achieved. Infants with persistent low BG levels of <47 mg/dL despite 3 dextrose gels and feeds were admitted to the NICU for IV dextrose therapy. In both units, BG screening was preformed using bedside reagent test-strip glucose analyzer and any level <50 mg/dL or >150 mg/dL was confirmed by laboratory enzymatic method or by an i-STAT analyzer (Abbott Point of Care Inc, Princeton, NJ). Once the infant had 3 stable BG levels and fair enteral intake, weaning of the IV dextrose fluid would start. Infants were discharged home if able to maintain BG >60 mg/dL for >24 hours off IV dextrose on a routine feeding schedule every 3 to 4 hours.
Statistical Methods
Wilcoxon tests and Fisher’s exact tests were performed on the baseline characteristics to compare any differences between infants in whom feeds were continued versus infants who were kept NPO at initiation of parenteral dextrose therapy. Tests for differences between the 2 groups were performed on the outcomes of interest based on the corresponding models. Analysis of variance (ANOVA) models were fit for NICU length of stay, duration on IV dextrose fluid (with square root transformation to satisfy normality assumptions), and the infant’s lowest sodium level. Analyses based on the use of a generalized linear model in conjunction with a generalized estimating equations approach to parameter estimation was performed on the frequency of low BG levels after stabilization (treated as Poisson distributed). Additionally, an ANOVA model was fit for BG levels (log transformed to satisfy normality assumptions) at various time points, where time was treated as a repeated measure, and an unstructured covariance matrix was used. To check the robustness of the tests, similar tests for differences were performed from models that additionally adjusted for whether growth was appropriate for the gestational age, whether the mother had diabetes, and whether the mother was on insulin. All statistical analyses were performed using SAS version 9.4, and all tests were used with a nominal significance level of .05.
Results
A total of 257 infants were admitted to both the NICUs with the diagnosis of NH during the study period, and 76 infants (29.5%) met inclusion criteria for the study. Of the 76 infants, 47 (62%) infants did not receive enteral feeds until BGs were stable (3 consecutive BGs >50 mg/dL), while 29 (38%) infants were allowed to continue enteral feeding at the initiation of parenteral glucose therapy. There was no significant difference in baseline characteristics in any of the parameters studied between the 2 groups (Table 1).
Baseline Characteristics of Infants With Neonatal Hypoglycemia (NH) Who Were Fed (NH-Feeding) and Not Fed (NH-NPO) at Initiation of Parenteral Glucose Therapy on Admission to the NICU.
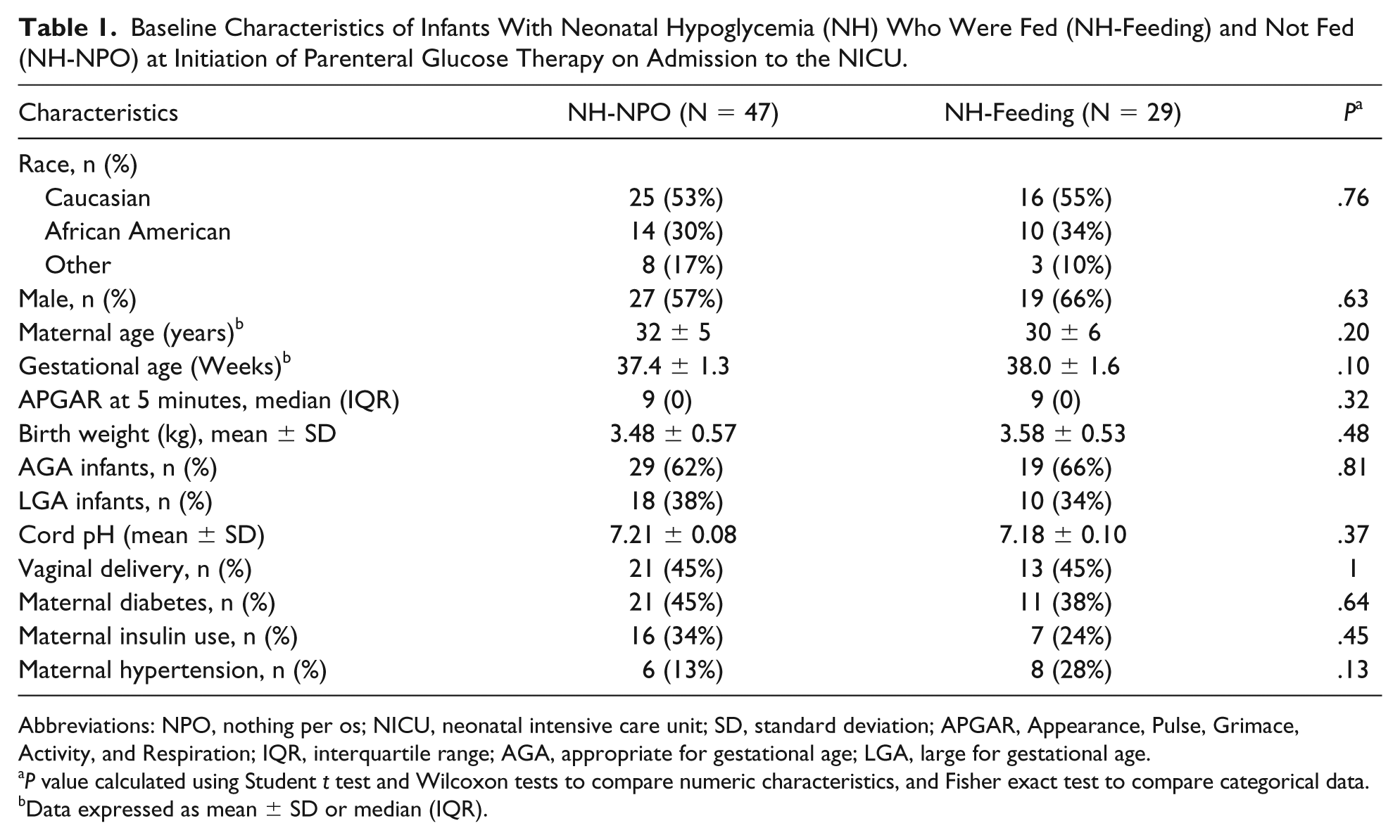
Abbreviations: NPO, nothing per os; NICU, neonatal intensive care unit; SD, standard deviation; APGAR, Appearance, Pulse, Grimace, Activity, and Respiration; IQR, interquartile range; AGA, appropriate for gestational age; LGA, large for gestational age.
P value calculated using Student t test and Wilcoxon tests to compare numeric characteristics, and Fisher exact test to compare categorical data.
Data expressed as mean ± SD or median (IQR).
The BG concentration on admission to the NICU at the time of initiation of parenteral dextrose therapy was not different between the groups (31 ± 7.3 mg/dL in NH-NPO group vs 34 ± 6.3 mg/dL in the NH-feeding group).
The outcome measures studied between the 2 groups are shown in Table 2.
Outcome Characteristics of Infants With Neonatal Hypoglycemia (NH) Who Were Fed (NH-Feeding) and Not Fed (NH-NPO) at Initiation of Parenteral Glucose Therapy on Admission to the NICU a .

Abbreviations: NPO, nil per os; NICU, neonatal intensive care unit; BG, blood glucose; SD, standard deviation; ANOVA, analysis of variance.
Data expressed as mean ± SD.
P value calculated using ANOVA model.
Adjusted P value calculated using ANOVA model after adjusting for birth weight, maternal diabetes status, and maternal insulin use.
All outcome measures studied by statistical models remained consistent even after adjusting for other covariates. After stabilization of BG levels (defined as having at least 3 stable BG >50 mg/dL measured every 3 hours in all infants), infants in the NH-NPO group had significantly more episodes of hypoglycemia (defined as BG <50 mg/dL) compared with the NH-Fed group. Infants who were fed at the time of the initiation of the IV dextrose therapy required shorter duration of IV dextrose therapy (67.3 ± 28 hours in NH-NPO group vs 53.2 ± 2.3 hours in NH-feeding group; P < .03) and had shorter NICU stay compared with the infant who were kept NPO (5.87 ± 1.4 days in NH-NPO group vs 4.93 ± 1.4 days in NH-feeding group; P < .006; Table 2). The maximum GIR measured in mg/kg/min required to stabilize BG was higher in the NPO group compared with the feeding group (7.0 ± 2.4 in NH-NPO group vs 5.3 ± 1.1 in NH-feeding group; P < .001). Enteral feedings were not included in the GIR calculation due to the fluctuations of oral intake.
Figure 1 represents the BG levels at various time points from admission to 24 hours later. Infants in both groups had similar BG levels at admission (31 ± 7.3 mg/dL in NH-NPO group vs 34 ± 6.3 mg/dL in the NH-feeding group). However, BG levels at 30 and 60 minutes were significantly higher in the feeding group compared with the NH-NPO group.

Blood glucose levels at 0 minute, 30 minutes, 1 hour, 2 hours, 3 hours, 6 hours, 12 hours, and 24 hours after admission to intensive care unit in both the treatment groups (neonatal hypoglycemia [NH]-Fed group: dashed line with filled triangles; NH-nothing per os [NPO] group: dark line with white circles). Blood glucose concentrations were significantly higher at 30 minutes and 1 hour after admission in the NH-Fed group (*P < .05, **P < .005; unpaired Student t test vs NH-NPO group).
Lowest sodium levels were compared as an objective measure to evaluate for the possibility for fluid overload that could occur in infants who continued to feed in addition to the parenteral fluids. Average lowest sodium level was not significantly different between the 2 groups (137.8 ± 3.5 mEq/L in the NH-NPO group compared with 136.9 ± 0.3 mEq/L in the NH-feeding group). There is no difference in the percentage of infants with serum sodium <135 mEq/L between the groups (20% in the NH-Fed group vs 13% in NH-NPO group; P value of .75).
Discussion
The results of the study suggest that infants admitted for parenteral dextrose therapy for NH who continued to feed at initiation of parenteral dextrose therapy required shorter duration of IV dextrose therapy, spent less time in the NICU, and had more stable BG concentrations compared with infants who were kept NPO for several hours at the initiation of IV dextrose therapy.
In this study, decision regarding initiation of feeds in infants with NH was solely based on the clinician’s preference. In infants who were either SGA and/or with intrauterine growth restriction, there was a general agreement to keep these infants without enteral feeds or on minimal feeds at the initiation of IV dextrose therapy; as it was shown in previous studies that SGA infants are at higher risk for gastrointestinal pathologies such as necrotizing enterocolitis and feeding intolerance.17,18 For this reason, these infants were excluded.
The proposed rationale for not feeding hypoglycemic neonates is to prevent pancreatic stimulation and insulin release by the presence of nutrients in the gastrointestinal tract and/or glucose in the bloodstream. 19 Theoretically, keeping infants NPO at initiation of IV dextrose therapy prevents spikes of insulin secretion associated with intermittent feeds causing recurrent episodic hypoglycemia, but there is limited evidence in the literature to support this theory. While high BG levels will stimulate insulin release in children and adults, this relationship is less clear in infants as shown previously by Hawdon et al. 20 Insulin levels did not correlate with BG levels in newborns at a wide range of blood sugars between 2.5 and 26.1 mmol/L. 20 Possible explanations for this relation may in part be that the presence of ketone bodies in term neonates that the brain utilizes for metabolism instead of glucose, which could result in preventing neuroendocrine suppression of insulin release. 21 Other explanation may be that in newborns, adenyl cyclase system that is responsible for the early phase of glucose-mediated insulin release is less responsive. 22
In our study, the frequency of episodes of BG <50 mg/dL after stabilization were significantly lower in the NH-feeding group. Enteral galactose supplementation in canines has been shown to enhance hepatic glycogen synthase activity compared with completely fasted pups. 23 Lactose (glucose + galactose), being the major component of human milk and/or infant formula, promotes glycogen synthesis in the liver and enhances liver carbohydrate uptake, which may play a role in the attenuation of BG variability following stabilization in these neonates. In addition to that galactose is quickly metabolized in newborn infants and provokes minimal stimulation of insulin secretion, 24 suggesting that it may be an excellent substitute for glucose among hyperinsulinemic infants of diabetic mothers or premature infants with glucose intolerance. 25 From the physiologic prospective, the benefits of feeding infants as soon as possible may result in less insulin secretion resulting in minimal variability in BG concentrations, as seen in our study. The clinical implications of feeding early even by a few hours are significant. This resulted in reduced GIR in these infants, leading to less number of hours on glucose infusion and shorter length of stay in the hospital. The longer term benefits are still not well characterized, as the pattern of insulin secretion in the newborn period may program the subsequent development of metabolic control as adults. 26
In our study, both groups of infants were started initially on IV dextrose to provide an infusion rate of 4 to 8 mg/kg/min. Infants who were allowed to feed benefited from extra calories mainly from the additional carbohydrates contained in the breast milk or supplemental formula. In addition to providing calories, lactose contained in either formula or maternal breast milk is quickly metabolized by the newborn with minimal stimulation of the insulin secretion. 24 Protein and fat in milk also contribute indirectly to glucose hemostasis by providing gluconeogenesis substrates. This likely resulted in higher BG levels at 30 minutes and 1 hour after parenteral glucose administration compared with the infants who were kept NPO. We also observed that the infants in the feeding group were less likely to have low BG levels after initial glucose stabilization. Earlier stabilization of blood sugars likely resulted in decreased duration of IV dextrose therapy and shorter length of stay. In addition to these benefits, it is also well known that enteral nutrition provides soothing effect for infants and it does play a major role in establishing the mother infant bonding, especially in breast-fed newborns. 27
We acknowledge several limitations to the study. In this retrospective study, although the infants in both groups were similar in baseline characteristics, admission BG levels, and hypoglycemia risk factors, we cannot rule out the presence of factors that were not documented that might have influenced decision-making regarding feeding. In addition, protocols for management of hypoglycemia and weaning protocols vary among institutions, and hence, the results may not be generalizable. We did not measure insulin levels, which could have confirmed the physiologic basis for feeding early. However, previous studies have indicated that insulin level at a single point of time may not reflect the real-time pancreatic response either due to periodic release of insulin or hepatic clearance of insulin. 28 Finally, due to technical difficulties at the time of the study, continuous glucose monitoring devices to monitor continuous glucose levels were not used and episodes of hypoglycemia may have gone undetected.
In conclusion, continuation of the feeding of the infants with hypoglycemia who require IV dextrose therapy not only results in a shorter duration of parenteral glucose therapy but also reduces length of stay in the hospital. This has important implications from the standpoint of cost and efficient utilization of resources in an intensive care setting, given the number of infants admitted with the diagnosis of NH. Decrease in length of stay also may translate to better maternal infant bonding promoting breastfeeding in infants. The results from this study should be further validated in a prospective cohort.
Footnotes
Acknowledgements
Statistical analysis reported in this publication was supported by the National Center for Advancing Translational Sciences of the National Institutes of Health under award Number UL1TR001412.
Author Contributions
MA: conceptualized and designed the study, collected, analyzed and interpreted the data; drafted the initial manuscript and reviewed and revised the manuscript.
LS, VHSK and BM: conceptualized the study design, contributed to analyses and interpretation of data, drafting and revising the manuscript for critically important intellectual content.
GEW and LM: supported analyses and interpretation of data and revised the manuscript critically for intellectual content. All authors approved the final manuscript as submitted and agree to be accountable for all aspects of the work.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.