
Abstract
We report a case of a neonate, delivered by C-section, that rapidly developed respiratory compromise and hemodynamic instability prompting admission to critical care. Urgent cardiology assessment with echocardiography revealed severe systolic dysfunction from localized myocardial ischemia and pulmonary hypertension. Their management progressively escalated, eventually requiring inotropic support. Despite intensive treatment and meticulous nursing with demonstrable improvement of cardiac function, they deteriorated suddenly and died on Day 2 post-partum. This case emphasizes the challenge in early recognition of neonatal shock due to often nonspecific presentations, with hemodynamic compromise arising later. We recommend close vigilance for deterioration, awareness of indolent etiology including viral myocarditis, titration of appropriate inotropes and synergistic adjunctive vasodilators, and consideration of immune modulators such as corticosteroids that addresses biochemical deficiencies and support cardiac function. Ultimately, aggressive, targeted, and multi-focal treatment, especially in resource-limited environments, maximizes the chances of survival in challenging clinical situations such as progressive neonatal shock.
Introduction
Shock in the newborn can have unique etio-pathological origins, necessitating careful assessment to direct specific interventions. Unlike adults and older pediatric patients, neonatal shock is often only discernible by the presence of hypotension in the uncompensated phase, at which point it may be too late to successfully resuscitate them. 1 Neonatal sepsis is particularly associated with systolic and diastolic myocardial dysfunction, 2 where non-survivors were found to have had significantly higher serum cardiac troponin-T concentrations and left ventricular Tei indices on echocardiography. 3 Furthermore, neonatal cardiomyopathies account for ~1% of childhood cardiac disease, with an incidence of ~1:10 000 live births, and are responsible for 10% of all pediatric cardiac deaths. 4 We report the following case with the aims of illustrating the clinical challenges in recognizing cardiogenic shock in the neonate, the importance of considering and addressing pathogenic causes of early cardiomyopathy, and highlighting the relatively novel role of immune modulation as well as corticosteroid therapy in their early management to augment cardiorespiratory support in critical care. Simply put, our educational objectives in this report are:
To highlight the challenges in diagnosing shock in neonates and determining the underlying cause, and thus the need for meticulous assessment.
To recommend simple yet crucial interventions in preventing neonatal mortality secondary to shock, particularly in resource-limited environments.
Case Report
A full-term newborn baby weighing 3.3 kg, delivered by Caesarian section due to pregnancy-induced hypertension (PIH), was a product of an otherwise uncomplicated pregnancy. Their mother (G4P3A0) had no significant medical history prenatally.
Post-delivery apnea was resuscitated, with an APGAR score at 1 minute post-partum of 4/10 rising to 7/10 at 5 minutes. One hour later, he became pale, cyanosed, tachypneic and irritable. Nasal O2 therapy at 1 L/minute was commenced, and he was transferred to the NICU with a heart rate (HR) of 170 bpm, respiratory rate (RR) of 70 cycles/minute, blood pressure (BP) of 55/35 mmHg, O2 saturations of 81% on supplementation, and temperature of 37.5°C. Clinical examination revealed skin mottling, cold peripheries, subcostal and intercostal recessions, and huge hepatomegaly. Their chest radiograph (shown in Figure 1) demonstrated cardiomegaly, while electrocardiography (ECG) recorded sinus tachycardia with evidence of biventricular hypertrophy. In light of these findings and their persisting cyanosis despite O2 therapy, a cardiology consult was sought urgently.

Chest radiograph performed on NICU within 2 hours post-partum prior to echocardiography, demonstrating cardiomegaly.
A subsequent echocardiography (using Simpson’s biplane method) demonstrated: severe left ventricular (LV) dysfunction with dilatation, a dilated right ventricle (RV) with moderate tricuspid regurgitation (TR), moderate-severe mitral regurgitation (MR), moderate aortic regurgitation (AR), dilated pulmonary artery, and normal ascending aorta with no coarctation. Ejection fraction (EF) was recorded at 33%.
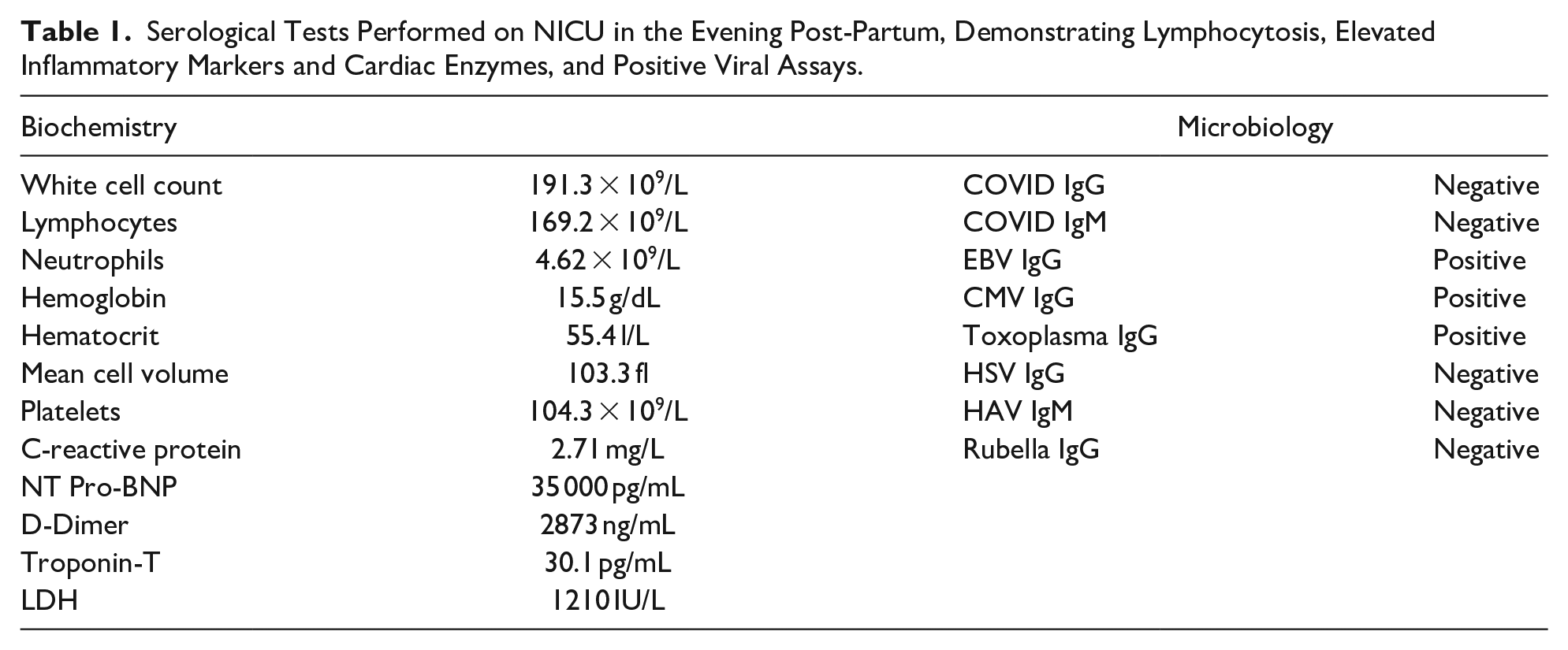
The patient consequently received fluid supplementation amounting to two-third of their daily requirements (totaling 70 mL/kg/day), diuresis via 3 doses of 1.5 mg Lasix (Furosemide), and empirical dual antibiotic therapy. Dopamine infusion was initiated at 10 µg/kg/minute, which failed to support his BP (now at 60/40)—this was switched to Dobutamine at 10 µg/kg/minute that resulted in an improved BP of 80/60 alongside rising O2 saturations (to 85%) over the ensuing 10 hours. Serological investigations prominently exhibited raised cardiac enzymes and positive viral assays (shown in Table 1).
Serological Tests Performed on NICU in the Evening Post-Partum, Demonstrating Lymphocytosis, Elevated Inflammatory Markers and Cardiac Enzymes, and Positive Viral Assays.
By the next morning, the patient’s condition had improved; he was less irritable, although crying for feed, with a positive rooting reflex and O2 saturations above 88%. At 20 hours, a follow-up echocardiogram demonstrated reduced LV dilation, mild MR/AR, persisting moderate-severe TR, but increased EF reaching 50% with a pulmonary (tricuspid regurgitation) gradient of 70 mmHg.
Accordingly, 3 doses of 1 mg Sildenafil were administered, while the patient maintained their BP at around 75/55 for the next 12 hours. However, in the following early morning his BP suddenly dropped to 50/0 along with rapid desaturation. Despite all resuscitative measures including intubation/ventilation, further inotropes, and eventual cardiopulmonary resuscitation, within 2 hours of deterioration the patient passed away. As per the wishes of the deceased patient’s family, a postmortem was not conducted.
Discussion
Hypotension, given its ease of monitoring, is the most commonly used determinant of decreased perfusion in NICU that nevertheless tends to be a late sign in neonatal shock 1 ; in this case, it arose a few hours after birth. Early clinical features of hemodynamic instability include pallor, poor feeding, tachycardia, tachypnea, and labile temperatures, while cardiac dysfunction in neonates can present in a similarly nonspecific manner. 5
A moderately dilated severely dysfunctional LV with associated MR suggests myocardial dysfunction or structural heart defects including aortic stenosis or coarctation—the latter were excluded. Furthermore, a markedly dilated RV and right atrium (RA) was attributed to pulmonary hypertension (PHTN) and severe TR, having also excluded total anomalous pulmonary venous drainage (TAPVD) and Ebstein’s anomaly. Here, PHTN was likely secondary to MR, while another report found that PHTN discovered at autopsy was consistent with long-standing LV failure. 6 Hence, determining pulmonary artery pressure in the presence of severe TR is important. 7
Nevertheless, the most probable underlying cause of this presentation is myocarditis. In addition to myocardial dysfunction with severe LV systolic dysfunction and dyskinetic hypokinetic LV walls, regional wall-motion abnormalities with anterior and posterior desynchronization indicative of local myocardial ischemia are discernible—this has been described in myocarditis. 6 Furthermore, the clinical value of cardiac enzymes in pediatrics is ascribed to acute myocarditis, cardiac arrhythmias, perinatal asphyxia, drug-induced cardiotoxicity, perioperative myocardial injury following intervention for congenital heart defects, and cardiac transplantation. 8 Raised Troponin-T in this presentation alludes toward myocarditis rather than myocardial infarction. 9
Critically, initial functional echocardiography (point-of-care sonography providing real-time hemodynamic information from myocardial function, loading conditions, and cardiac output) illustrated severe LV dysfunction within 2 hours of birth. This measure is vital in intensive care settings, influencing clinical management in 30% to 60% of cases.10,11
Despite follow-up echocardiography demonstrating improved extended wall motion and stability, the patient deteriorated, exhibiting hypotension and respiratory distress which may be explained by progressively exhausted myocardium losing its ability to support cardiac output due to fulminating myocarditis, or alternatively PHTN subsequent to either exaggerated mitral regurgitation or exacerbated pulmonary vascular tone. 12 Adding Sildenafil may have induced hypotension, although he was on concurrent inotropes. However, this was at minimum dosage; indeed, under-titration of inotrope dosage, alongside untargeted respiratory support, may have contributed to mortality.
Furthermore, the initial choice of Dopamine resulted in observable ongoing hypotension. In the context of acute pulmonary hypertension there is evidence Dopamine can cause nonspecific widespread vasoconstriction reducing left ventricular preload and increasing afterload, both limiting systemic perfusion, in addition to an increased risk of cardiac ischemia from its inotropic and chronotropic effects. 13 This was mediated by switching to Dobutamine with demonstrable improvement, although adrenaline (epinephrine) has been touted as an alternative given its less positively chronotropic profile with increase in cardiac index. These can be used in conjunction with alternative, potentially synergistic vasodilators such as Milrinone 13 and inhaled nitrous oxide 14 to improve oxygenation, although crucially adequate systemic pressures are required to maintain right and left ventricular perfusion respectively.
Additionally, the treatment plan lacked immunoglobulin infusion and antiviral therapy. Immunoglobulin is thought to improve outcomes of enteroviral diseases in neonates, although the evidence is limited, while antiviral therapy with Pleconaril (preventing viral RNA exposure) remains a promising yet experimental therapy. 15
Finally, low-dose corticosteroid has since been added to our treatment protocol, as there is strong evidence to suggest low cortisol levels in sick term and preterm infants associate with negative outcomes. 16 Both adrenal insufficiency and decreased vascular responsiveness to catecholamines can contribute even to vasopressor-resistant shock, hence the potential cardiovascular benefit of low-dose steroids in shocked infants. 17
Conclusion
Neonatal hemodynamic instability should be evaluated meticulously and supported by a rapid escalation plan. Timely specialist input is indicated if organ dysfunction is evident—early functional echocardiography provided crucial diagnostic insight which guided treatment. Perspective into the potential underlying etiology, which we believed to be myocarditis of possibly viral origin, is similarly crucial. Management should therefore entail early respiratory optimization and aggressive cardiovascular support with titration of appropriate inotropes, and consideration of adjunctive vasodilators where adequate systemic perfusion has been achieved. Adjuvant therapies such as immunomodulation and corticosteroid therapy may also help in augmenting cardiac function as well as curbing the systemic inflammatory response, ultimately reducing the chance of mortality.
Footnotes
Acknowledgements
We would like to thank the clinical staff at the Pediatric and Obstetric Units Neonatal Intensive Care Unit, and Pathology Department at Anwar Sheikha Medical City High-Quality Hospital for their provision of care and for contributing to this report to help impart fundamental learning.
Author Contributions
Finally, we recognize the contributions of the respective authors in the conception and design of the study (AFS, MHJ), the analysis and interpretation of all data involved (AFS, AMJ, MHJ), the drafting (AFS, AMJ) and critical revision (AFS, MHJ) of the manuscript, and final approval of the completed study (AFS, AMJ, MHJ).
Data Availability
Anonymized data for the purpose of medical research or teaching can be requested from the Department of Pediatrics at Anwar Sheikha Medical City High-Quality Hospital, Sulaimaniyah, Iraq.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval and Consent
All clinical information and imaging was provided and published with written consent of the relevant supervising clinicians and the hospital’s appointed legally authorized representative of the family of the deceased patient. As all data was anonymized and explicit consent was provided, this report did not require ethics board review, and was locally approved by the Institutional Clinical Governance Department.