
Abstract
Background:
Improper inhaler technique negatively impacts asthma control, yet data on this issue in Vietnam remain limited. This study assessed the prevalence and impact of improper inhaler technique on pediatric asthma control and examined the role of caregivers in this context.
Methods:
An analytical cross-sectional study was conducted among children with asthma and their caregivers. Logistic regression analyzed associations between improper inhaler technique, uncontrolled asthma, and caregivers’ attitudes and practices in asthma management.
Results:
Among 186 children, 45.2% had improper inhaler technique, which was independently associated with uncontrolled asthma (AOR = 2.33, 95% CI: 1.27-4.3, P = .006). Regarding caregivers, failure to ensure adherence to prescribed controller medications and inadequate monitoring of remaining MDI medication were significantly associated with improper technique (P < .05).
Conclusion:
Improper inhaler technique is common and associated with poor asthma control. Caregivers’ involvement in medication adherence and monitoring plays a crucial role in addressing this issue.
Introduction
Asthma is a chronic respiratory condition affecting individuals of all ages, characterized by airway inflammation, bronchial hyperresponsiveness, and reversible airflow obstruction. It is a leading cause of healthcare utilization, school absenteeism, economic burden, and impaired quality of life in pediatric populations.1 -4 Despite advancements in management and the availability of effective treatments, asthma control remains inadequate in many regions, including Vietnam. 5 Poor asthma control is linked to frequent exacerbations, hospitalizations, and long-term complications, making it essential to address contributing factors.6,7
Inhaled medications, such as corticosteroids and bronchodilators, play a critical role in managing asthma by targeting airway inflammation and obstruction directly.8,9 However, their effectiveness depends on correct inhaler technique, an area where many patients face challenges. Studies have shown that lack of knowledge, non-adherence to treatment, and incorrect technique are factors that affect asthma control in both adults and children.10 -12 Incorrect usage reduces medication delivery to the lungs, diminishing its therapeutic effects and contributing to poor disease control.13,14 Studies highlight widespread errors with metered-dose inhalers (MDIs) among children, with error rates ranging from 50% to 81%.13,15 While the use of spacer devices improves technique, issues such as rapid breathing and insufficient breath-holding persist, influenced by developmental limitations, a lack of training, and gaps in understanding asthma management.14,16,17
Caregivers significantly influence pediatric asthma outcomes, particularly in Vietnamese families, where strong family-oriented values place them at the center of health-related decisions.14,18 -20 However, many caregivers lack the knowledge and skills to support proper inhaler use and consistent treatment adherence. Research reveals substantial knowledge gaps, with more than half of parents unaware of how corticosteroid inhalers work and many administering them only during symptomatic episodes rather than as part of a daily regimen. 19 Other challenges include financial constraints, difficulties understanding medication instructions, and limited capacity to monitor adherence, particularly when children are at school.21,22 Misunderstandings and inconsistent practices among caregivers contribute to poor asthma control and improper medication use.
Data on the prevalence and consequences of improper inhaler technique among Vietnamese children remain scarce. Barriers such as insufficient asthma education programs, limited training for caregivers and patients, and systemic healthcare challenges exacerbate the problem. 23 Additionally, misconceptions, reliance on traditional remedies, and stigma surrounding chronic illnesses negatively impact adherence to treatment guidelines.20,24 Addressing these obstacles is crucial for improving asthma outcomes in this population.
This study aims to investigate characteristics of inhaler technique in Vietnamese children with asthma, assess its impact on asthma control, and explore caregiver attitudes and practical behaviors that may contribute to improper usage. Understanding these factors is vital for developing targeted interventions, including improved education and training programs, to optimize asthma management and enhance outcomes for affected children.
Methods
Study Design, Settings, and Participants
An analytical cross-sectional study was conducted on pediatric asthma patients and their caregivers at the pediatric asthma outpatient clinics of a pediatric hospital in Vietnam, from March to September 2024. This hospital houses one of the largest professional pediatric outpatient clinics for asthma patients in the region and is the most specialized pediatric care facility.
Children aged 4 to 16 years with asthma diagnosed according to GINA guidelines, who had been under management for at least 1 consecutive month and were currently using metered-dose inhaler devices for asthma control, were invited to participate in the study. Their caregivers, who were primarily responsible for their asthma care and had lived with them for an extended period since the asthma diagnosis, were also invited to participate. Patients and their caregivers were excluded if either was unable to complete the interview or asthma control assessment due to subjective or objective issues. Additionally, children were excluded if they had siblings living in the same household who had already participated in the study.
The required sample size was determined using the formula for estimating a proportion. 25 Based on a prior study, which reported that 13.4% of children had no errors in inhaler technique, 14 the sample size was calculated with an alpha level of .05, a margin of error of 5%, and an attrition rate of 4% to account for incomplete data. The resulting sample size was 186 children with asthma. A convenience sampling method was employed to recruit an adequate number of participants during the study period.
Data Collection
Data on demographics, medical history, asthma control, and inhaler technique were collected from medical records and direct interviews. Asthma control was evaluated using the Childhood Asthma Control Test (C-ACT) for children aged 4 to 11 years, and the Asthma Control Test (ACT) for children aged 12 years and older. The level of asthma control was categorized based on the C-ACT or ACT scores, with scores ≤19 indicating uncontrolled asthma and >19 indicating controlled asthma.26,27
The inhaler technique was evaluated and scored using a standard checklist outlined in a previous study, which included 7 essential steps for each type of MDI usage: MDI alone, MDI with a spacer without a mask, and MDI with a spacer and mask. 14 Among these 7 steps, 4 were identified as critical (Appendix Table 1). During the interview, caregivers and their children were shown photos of inhalers and/or actual devices to help them correctly identify the device used. This information was cross-checked with medical records to ensure accuracy and consistency regarding the inhaler type used by the child. In the culturally family-oriented context of Vietnam, caregivers at our clinics are routinely instructed on the essential steps for proper MDI device usage and how to assist and supervise their child in using the device before asthma management begins. During the assessment, caregivers were asked to describe the steps their child followed to use the inhaler. Each correctly performed step was awarded 1 point, with a maximum score of 7 per device type. Any incorrectly performed step resulted in a deduction. Inhaler technique was considered adequate if all steps were performed correctly, and inadequate if at least 1 error was identified.
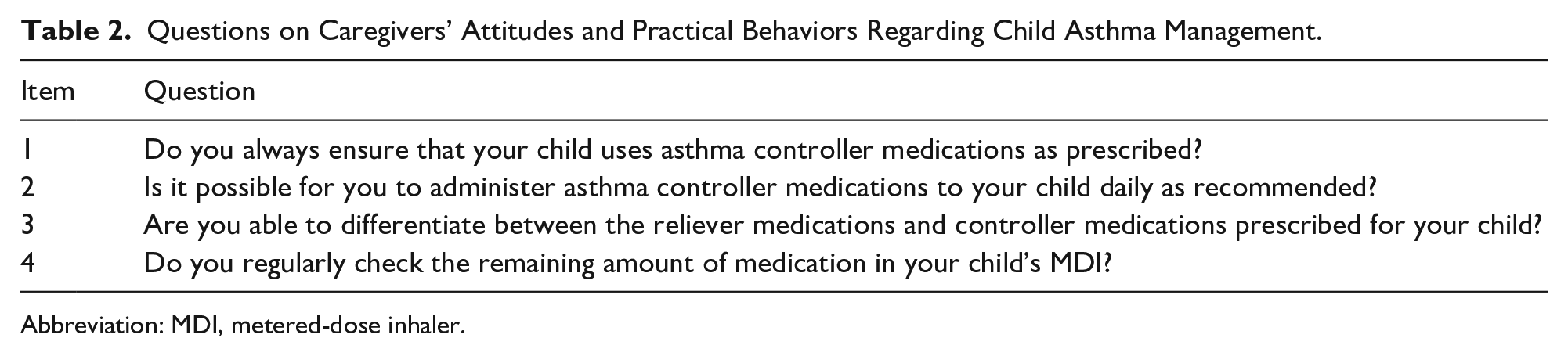
Caregivers’ attitudes and practical behaviors regarding asthma management were assessed based on 4 key aspects: ensuring the child uses asthma controller medications as prescribed, administering these medications daily as recommended, differentiating between reliever and controller medications, and regularly checking the remaining amount of medication in the MDI (Appendix Table 2). These aspects were derived from common challenges caregivers often encounter in clinical practice. Further research is necessary to validate these questions and enhance their psychometric properties for application in the Vietnamese context. Caregiver responses were recorded as “yes” or “no” during direct interviews.
Statistical Analysis
Analyses in this study were performed using R version 4.4.2. Data are descriptively presented as frequency (n) and percentage (%) for categorical variables, with comparisons made using the chi-square test or Fisher’s exact test, as appropriate. Quantitative variables are presented as mean ± standard deviation (SD) for data with a normal distribution or as median and interquartile range (IQR) for non-normally distributed data. Univariable and multivariable logistic regression analyses were conducted to investigate the association between inhaler technique and asthma control, as well as the association between caregivers’ attitudes and practical behaviors and improper inhaler technique. Odds ratios (ORs) with their 95% confidence intervals (CIs) are reported along with P-values. A P-value of less than .05 was considered statistically significant.
Ethical Approval and Informed Consent
This study obtained ethical approval from the Ethics Committee in Biomedical Research at Can Tho University of Medicine and Pharmacy (IRB approval number 23.114.SV/PCT-HDDD) and received approval from the Board of Directors of Can Tho Children’s Hospital. Written informed consent was obtained from parents or legal guardians for their and their child’s participation before the study commenced.
Results
General Characteristics of Study Participants
A total of 186 participants with a mean age of 7.0 ± 2.4 years were included in the study, with males comprising 53.2% of the sample. Nearly half of the participants had a history of asthma for 1 to 5 years (45.2%), a similar proportion (44.6%) for less than 1 year, while 10.2% had asthma for more than 5 years. Additionally, 34.9% of the participants had been hospitalized due to asthma exacerbations in the past year. Overweight and obesity were prevalent, accounting for 55.9% of the study population. Furthermore, allergic conditions such as food allergies, allergic rhinitis, and atopic dermatitis were reported in 18.3%, 31.7%, and 5.4% of the participants, respectively. A parental history of asthma was present in 16.1% of the participants. Regarding asthma control, participants had a mean C-ACT/ACT score of 21.3 ± 4.2 points. Using a cut-off score of 19, 43.5% of the participants were classified as having uncontrolled asthma. In terms of inhaler use, most participants (72%) used an MDI with a spacer and mask, while 19.9% used an MDI alone and 8.1% used an MDI with a spacer. ICS alone constituted 44.1% of the primary treatments used in the past 4 weeks (Table 1).
General Characteristics of Patients with Asthma (n = 186).

Abbreviations: SD, standard deviation; GERD, gastroesophageal reflux disorder; MDI, metered-dose inhaler; ICS, inhaled corticosteroids; LABA, long-acting beta agonists; FDC, fixed dose combination; LTRA, leukotriene receptor antagonists.
Inhaler Technique and Asthma Control
Regarding the inhaler technique, only 54.8% of participants demonstrated correct use (no errors). The uncontrolled group exhibited a significantly higher rate of incorrect technique compared to the controlled group (56.8% vs 36.2%, P = .005). Furthermore, analysis revealed a clear difference in inhaler technique between the 2 groups. The controlled group demonstrated a higher proportion of participants with completely correct technique, with 63.8% performing all 7 steps correctly, compared to only 43.2% in the uncontrolled group. A similar pattern was observed in the performance of the 4 critical steps, with the controlled group demonstrating better results. Both of these differences were statistically significant (P = .010 for the total steps and P = .007 for the critical steps), as shown in Table 2.
Characteristics of Metered-Dose Inhaler Technique by Asthma Control Level.

Abbreviation: MDI, metered-dose inhaler.
Fisher’s exact test.
Critical steps.
For patients using MDIs alone/with a spacer without a mask, 50% performed all 7 steps of the inhaler technique without any errors. Of the remaining participants, 23.1% made 1 error, 11.5% made 2 errors, and a smaller proportion made 3 to 5 errors. When focusing on the 4 critical steps, 50% performed without errors, while 28.8%, 13.5%, and 7.7% made 1, 2, and 3 errors, respectively (Figure 2). Among patients using this type of MDI, Steps 7 and 2 had the lowest proportion of correct execution (57.7% and 75%, respectively). Notably, the controlled group demonstrated significantly better performance in Step 6 (97% vs 68.4%, P = .007; Table 2 and Figure 1).

Distribution of correct metered-dose inhaler technique by usage type.
Similarly, for patients using MDIs with a spacer and mask, 56.7% performed all 7 steps without errors. The remaining participants showed a decreasing proportion of errors, with 26.1% making 1 error, 13.4% making 2 errors, and lower percentages making 3 to 5 errors. In the critical steps analysis for this group, 56.7% performed without errors, 29.1% made 1 error, 12% made 2 errors, and only 2.2% made 3 errors, as detailed in Figure 2. When using this type of MDI, Step 7 also had the lowest proportion of correct execution in both groups (68.7%), followed by Step 2 with a rate of 76.1%. The proportion of participants who correctly performed Steps 2 and 7 was higher in the controlled group than in the uncontrolled group (P > .05). There were no other significant differences observed between the groups for the remaining steps in either MDI type (Table 2 and Figure 1).
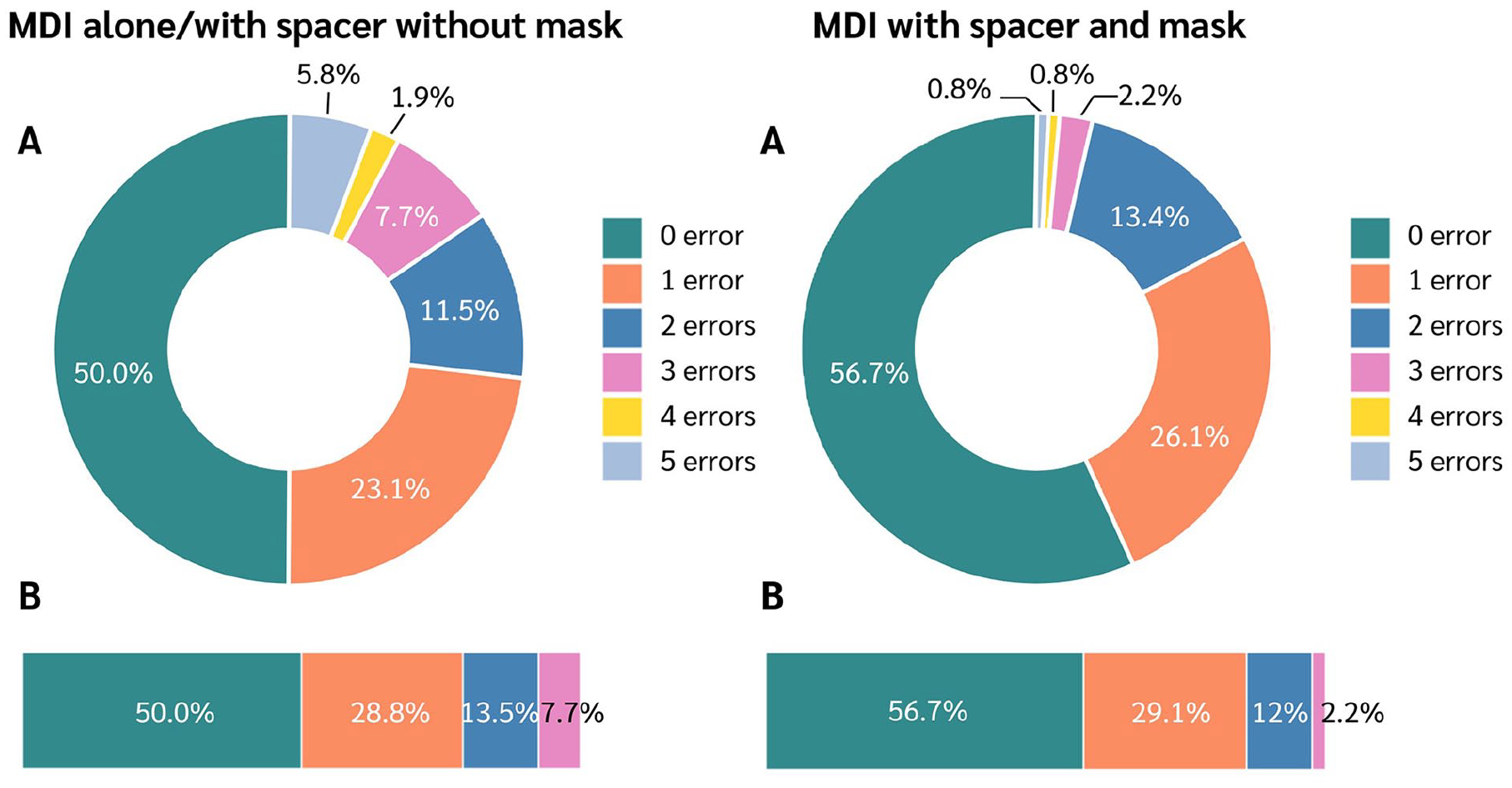
Error rate in MDI technique among patients. (A) Proportion of technique errors across 7 steps. (B) Proportion of technique errors in 4 critical steps.
In the logistic regression analysis, we found that improper technique was independently associated with uncontrolled asthma. Patients with improper technique had a 2.33 times higher risk of uncontrolled asthma compared to those with correct technique (AOR = 2.33, 95% CI: 1.27-4.3, P = .006; Table 3).
The Association Between Inhaler Technique and Uncontrolled Asthma.

Abbreviations: COR, crude odds ratio; AOR, adjusted odds ratio; CI, confidence interval; Ref, reference value; SD, standard deviation; IQR, Interquartile range.
Data are presented as n (%), mean ± SD or median (IQR).
We assessed factors associated with proper inhaler technique from 2 perspectives: caregiver attitudes and practical behaviors. We found that failure to ensure adherence to prescribed controller medications and inadequate monitoring of remaining MDI medication were significantly associated with improper technique (P < .05), as shown in Table 4.
Caregiver’s Factors Associated with Inadequate Inhaler Technique.

Abbreviations: COR, crude odds ratio; AOR, adjusted odds ratio; CI, confidence interval; Ref, reference value.
Data are presented as n (%).
The variables were adjusted for caregiver age, caregiver gender, and child’s asthma duration.
Discussion
The first pressurized metered dose inhaler (MDI), which was introduced in 1956 by Riker Laboratories, Inc., has become a cornerstone of asthma management in children for over 60 years. 28 However, treatment efficacy depends critically on not only the medication itself, but also on its accurate delivery to the airways. Effective treatment requires proper inhaler technique, but the multi-step process can be difficult for children to perform. 29 Our study evaluated the inhaler technique in children with asthma to assess its impact on disease control and identify factors influencing its correct use.
General Characteristics of Study Participants
Our study recorded an average C-ACT/ACT score of 21.3 ± 4.2 points. The uncontrolled group accounted for a large proportion, 43.5%. The majority of participants used MDI with a spacer and mask (72%), followed by MDI alone (19.9%), and only a small portion used MDI with a spacer (8.1%). Meanwhile, Almomani et al recorded an uncontrolled asthma rate of 67.3%. Among 134 cases using MDI, MDI alone accounted for 56%, followed by MDI with spacer and mask and MDI with spacer with rates of 25.4% and 18.6%, respectively. 14
The difference in the type of device used is due to the age and characteristics of each subject included in the study. In addition, studies have shown that using an MDI with a spacer and mask provides many benefits compared to using an MDI alone.29,30 One of the main benefits is the ability to improve the effectiveness of inhaled medication. The spacer helps keep the medicine in for a few seconds, allowing the patient to inhale slowly without having to coordinate the pressing of the button and inhalation, which is very important for young children or those who have difficulty using MDIs. In addition, the use of a mask and spacer helps ensure that the medication is fully delivered to the lungs, reducing the risk of medication deposition in the throat and mouth, thereby minimizing side effects such as oropharyngeal candidiasis and dysphonia.30 -32
Inhaler Technique and Asthma Control
Our study found that 54.8% of participants demonstrated adequate inhaler technique. When categorized by device type, 50% of those using MDIs alone or with a spacer without a mask exhibited the correct technique. Among those using an MDI with a spacer and mask, 56.7% demonstrated correct use. However, the reported prevalence of adequate inhaler technique varies considerably across studies. Notably, Sleath et al reported a rate of 8.1%, Almomani et al found 13.4%, Can et al observed 60.6%, and Capanoglu et al reported 68.1%.14,33 -35 This wide range reflects differences in study methodologies, age groups, and the criteria used to assess inhaler technique, as well as study settings.33 -35 These findings underscore the need for further research to identify the various factors influencing proper inhaler use.
When evaluating the steps involved in inhaler technique among patients using MDIs alone or with a spacer without a mask, we observed that Step 7 (“Hold breath for 10 seconds then exhale”) and Step 2 (“Breath out slowly away from the mouthpiece”) had the lowest performance rates, at 57.7% and 75%, respectively. Similar results were found in those using MDIs with a spacer and mask, with adherence rates for Step 7 (“Hold the mask over your child’s nose and mouth for 10-15 seconds”) and Step 2 (“Breath out slowly away from the mouthpiece”) at 68.7% and 76.1%, respectively. Notably, among those using MDIs with a spacer and mask, the controlled asthma group had higher adherence rates for these 2 steps compared to the uncontrolled group (all P-values <.05). The slow exhalation away from the mouthpiece in Step 2 helps empty the lungs, allowing for a deep and slow inhalation in the following steps, thereby optimizing drug delivery into the airways. 36 In Step 7, holding the mask over the child’s nose and mouth for 10 to 15 seconds allows the child to breathe normally, ensuring optimal drug deposition from the spacer. 30 By forming a seal, the mask prevents the medication from escaping and ensures more reaches the child’s lungs. 30 When a mask is not used, Step 7 (“Hold breath for 10 seconds then exhale”) allows time for the drug particles to interact with the bronchial or alveolar epithelium. Since the drug particles need to contact the epithelial surface to release the active substance and bind to the receptors on the cells, this is especially important for fine particles, which undergo Brownian motion and tend to be exhaled before they can contact the epithelium without a breath-hold.32,36 Therefore, these are 2 critical steps in performing the inhalation technique. However, our study recorded a high rate of errors in performing these 2 steps. Similarly, Almomani et al 14 also reported low accuracy rates for Step 2 and Step 7, with only 21.6% and 80% of participants performing these steps correctly, respectively. Moreover, this study showed that 51.5% of participants incorrectly performed Step 1 (“Shake the inhaler”). Various other studies have also demonstrated high error rates in these steps, even among adult populations.35,37,38
From a detailed assessment of the steps involved in using the inhaler, we observed that the controlled asthma group had more participants with adequate inhaler technique than the uncontrolled asthma group (63.8% vs 43.2%, P = .005). Subsequently, in the logistic regression analysis, we found that the odds of uncontrolled asthma were 2.33 times higher in the group with inadequate inhaler technique compared to the group with adequate technique (AOR = 2.33, 95% CI: 1.27-4.3, P = .006). Similarly, Capanoglu et al 35 reported that, among participants with controlled asthma according to the ACT and TRACK criteria, the proportion with adequate inhaler technique was significantly higher than those with inadequate technique (65.7% vs 47.2%, P = .016). Moreover, various studies conducted across different age groups have also demonstrated a statistically significant association between inadequate inhaler technique and uncontrolled asthma.39 -41 These findings highlight the importance of proper inhaler technique in pediatric asthma management, a point also emphasized in the GINA recommendations. 31
Caregiver and Inhaler Technique
Numerous studies have highlighted the significant influence of caregivers on children’s inadequate use of inhaler techniques. Therefore, to elucidate the role of caregivers in this issue, our study investigated factors related to caregivers’ attitudes and practices regarding their children’s inhaler use. Our findings revealed that caregivers who did not ensure their child used asthma controller medications as prescribed had a 1.88-fold increase in the odds of their children exhibiting inadequate inhaler technique compared to those who did (AOR = 1.88, 95% CI: 1.01-3.52, P = .046). This item assessed the caregiver’s commitment and responsibility toward their child’s inhaler technique. Similarly, caregivers who did not regularly check the remaining amount of medication in the MDI had 2.05 times the odds of their children not performing the technique correctly compared to those who did (AOR = 2.05, 95% CI: 1.11-3.85, P = .024). This item evaluated practical behaviors related to medication management. Meanwhile, caregivers who did not administer these medications daily as recommended, and who were unable to differentiate between reliever and controller medications, had an increase in the odds of their children exhibiting inadequate inhaler technique of 1.21 and 1.81 times, respectively. However, these associations did not reach statistical significance (P > .05). Many studies have clarified the role and emphasized the importance of caregiver knowledge as a factor related to inhaler technique and asthma control in children.14,16,19,23 Our study data further expands on this by clarifying that caregivers’ commitment, responsibility, and practical behaviors related to medication management are independently associated with children’s inhaler technique. This underscores the importance of caregivers’ attitudes and practical behaviors in pediatric asthma management.
Our study highlights that improper inhaler technique significantly impacts asthma control in children. Moreover, caregivers play a crucial role in ensuring proper inhaler use. These findings underscore the need for targeted education for both children and caregivers to improve caregivers’ knowledge, attitudes, and practices in pediatric asthma management, particularly in the context of Vietnam.
Strengths and Limitations
This study evaluated the inhaler technique in asthmatic children, including its impact on asthma control and the influence of caregivers on the prevalence of inadequate technique. However, this study has certain limitations. Firstly, our study was conducted at a single center and may not be representative of the entire Vietnamese population, a country with diverse cultural practices. Secondly, some information was collected from caregivers, potentially introducing recall bias. Finally, we assessed caregivers’ attitudes and practical behaviors through 4 key aspects derived from clinical practice. These questions have not been validated or had their psychometric properties enhanced for application in the Vietnamese context. Therefore, further research is needed to evaluate this issue in the Vietnamese population.
Conclusion
Our study identified a high prevalence of inadequate inhaler technique among children with asthma, which was significantly associated with uncontrolled asthma. Additionally, caregiver commitment, responsibility, and practical behaviors related to medication management were linked to inadequate inhaler technique in children.
Footnotes
Appendix
Questions on Caregivers’ Attitudes and Practical Behaviors Regarding Child Asthma Management.
| Item | Question |
|---|---|
| 1 | Do you always ensure that your child uses asthma controller medications as prescribed? |
| 2 | Is it possible for you to administer asthma controller medications to your child daily as recommended? |
| 3 | Are you able to differentiate between the reliever medications and controller medications prescribed for your child? |
| 4 | Do you regularly check the remaining amount of medication in your child’s MDI? |
Abbreviation: MDI, metered-dose inhaler.
Acknowledgements
We acknowledge the continued support from Can Tho University of Medicine and Pharmacy for this scientific research. We are also grateful to the Board of Directors of Can Tho Children’s Hospital and our colleagues at the pediatric asthma clinics for their support in this study. We extend our deepest thanks to our participants for their invaluable contributions to this research.