
Abstract
Introduction. Collaborative efforts among communities, schools, parents, and health professionals are needed to prevent childhood obesity, which touches one third of Canadian youth. The purpose of this case study was to obtain parents’ experience and perceptions about stakeholder roles in a multidisciplinary community-based intervention aiming to tackle childhood overweight. Methods. Data were collected from semistructured interviews with 10 parents following their participation in a community-based program designed to help families with overweight children adopt a healthier lifestyle. Results and Discussion. All parents preferred a multidisciplinary health team to monitor their children’s health. They expect that a physician or a pediatrician could diagnose overweight, explain results to parents, and refer families to resources. The team could also include professionals from health and education such as nutritionists/dietitians, nurses, physical education teachers, psychologists, kinesiologists, and social workers. Parents’ own perceived role would consist of instructing and reinforcing their children about healthy behaviors, role modeling for a healthy lifestyle, and seeking for professional help when needed. Conclusion. Parents involved in a support group with overweight child consider their own role as crucial to help changing their family lifestyle. They also prefer a multidisciplinary team that can address different aspects of overweight/obesity. However, the physician was perceived as having the central role in mobilizing a group of stakeholders around youth with overweight/obese, including the parents. A further step would be to understand barriers and facilitators to collaboration among health professionals in childhood overweight prevention and treatment.
Introduction
Overweight and obesity is affecting nearly one third of school-aged Canadians. 1 The probability of obesity persistence from childhood to adulthood is moderate and significant. 2 Several initiatives have been implemented in order to prevent or treat childhood obesity. 3 Collaborative efforts among communities, schools, parents, and health professionals are needed to implement childhood obesity prevention programs. 4 Community-based programs can be specifically designed to assist overweight children and families to practice healthy behaviors. 5
However, interventions designed specifically for overweight or obese people come with challenges. First of all, recruiting and retaining participants is not an easy task. 6 Among barriers to successful recruitment, some professionals mentioned parents’ denial about their children’s weight and their resistance to discuss weight issues. Professionals also shared they had low self-efficacy in raising this topic among concerned people. 7 Last, the role of each group and stakeholder involved in childhood obesity prevention program must be identified. 4
Role of Parents Toward Their Overweight Children
Parents’ involvement is crucial when it comes to shaping their children’s health behaviors.8,9 Literature about parenting shows that practices such as instruction, reinforcement, and role modeling can influence children’s physical activity and fruit and vegetable consumption. 10 Parents of overweight teenagers have also raised the importance of setting up a healthy home environment (eg, food), parental role modeling, and providing encouragement for their children’s positive efforts. 11
Role of Health and Education Practitioners
Physicians and pediatricians have an important role to play in preventing and managing childhood overweight.12,13 They can measure relevant anthropometric measurements (usually body mass index [BMI]), screen overweight and obesity, identify related health problems, and follow-up with their young patients. However, a study conducted by Gage et al 14 revealed that physicians see their role toward overweight children as less important. In this study, authors demonstrated that parents thought physicians should be more involved and proactive than the physicians stated they should be. 14 Authors also suggest that physicians’ role needs to be clarified in the context of multiagency approaches. In a Canadian survey, doctors have expressed the need for support from other health professionals. 15
Along with physicians and pediatricians, many other health professionals can intervene toward overweight children. An expert committee 16 suggested a health team concept to manage overweight children. The team could include health professionals such as nurses, nutritionists/dietitians, psychologists, and exercise specialists. School personnel can also get involved, such as physical education teachers and school nurses. 17 Unlike the physicians, the role of other professionals toward overweight children is not extensively documented.
In 2006, the American Dietetic Association promoted multicomponent programs that include behavioral counseling, promotion of physical activity, parent training/modeling, dietary counseling, and nutrition education. 18 Following these recommendations, the Groupe Enjeux pour Parents d’Enfants avec Excès de Poids (GEPEEP) program was created in 2007, in Shawinigan (Quebec, Canada), to provide weekly sessions including physical activity, healthy cooking, and workshops about healthy lifestyle for the families involved. The program was a partnership between the CSSS (Centre de Santé et Services Sociaux) and several health professionals of the community. A multidisciplinary health team including nurses, kinesiologists, nutritionists/dietitians, and social workers provided the workshops. This context was an excellent opportunity to investigate about the professional’s roles in childhood obesity prevention. Moreover, understanding parental views about childhood overweight represents a key step in forming effective liaison between health professionals and parents. 19
The purpose of this study was to (1) understand parents’ experience and appreciation of their participation in multidisciplinary obesity prevention program; (2) obtain parents’ views of their role and responsibilities toward their overweight children; and (3) obtain parental perceptions about which professionals can intervene and how they can get involved in a multidisciplinary context to tackle childhood overweight.
Methods
In this study, all families who took part in the GEPEEP program between 2007 and 2012 (N = 15) were invited by email to be interviewed individually.
The interviews were semistructured and the duration averaged 30 minutes. The main themes explored were the following: (1) parents’ experience about their participation in the GEPEEP program; (2) parents’ views of their role and responsibilities toward their overweight children; and (3) parental perceptions about which professionals can intervene and how they can get involved in a multidisciplinary context to tackle childhood overweight.
The interview guide was developed by a graduate student and revised by 2 professors. They were recorded (audio), transcribed, and analyzed using QSR NVivo 8 software. The interviews were performed in French and some quotes were translated for the purpose of this article. Data categorization and coding were performed separately by 2 graduate students, and after comparing the coding of both, they reached an agreement on the disparities. The content was analyzed according to the method developed by L’Écuyer. 20 A mixed categorization allowed the use of themes found in literature as well as new emerging themes.
Ethical Approval and Informed Consent
This study obtained a written clearance by the University Ethical Committee for Research on Human Beings (Comité d’éthique de la recherche avec des êtres humains) to perform the study without the need for an approval from the ethic committee, since the study was part of an evaluation of the intervention sought by GEPEEP. However, before each interview, the participants read and signed an information letter about the research protocol and were allowed to ask questions before they signed a consent form. They could refuse the interview without affecting their status within the group. To ensure the participants’ confidentiality, their names were replaced by a participants’ identification numbers.
Results
Participants
Ten parents—9 mothers and 1 father—agreed to participate. Table 1 summarizes the participants’ characteristics and background, including their motives for taking part in the GEPEEP program and the persons who referred them to participate in the program. The most frequently reported motive to take part in GEPEEP’s activities was related with the weight management issue. Most participants (8 out of 10) were referred to the program by a health professional (Table 1).
Participants’ Characteristics and Background.

Abbreviation: GEPEEP, Groupe Enjeux pour Parents d’Enfants avec Excès de Poids.
Parental Views of Their Role Toward Their Overweight Children
Parents were invited to share about the role they play toward their overweight children. The duties they mentioned are summarized in Table 2, along with supporting quotes. The majority of parents (n = 8) recognized the importance of role modeling. They believe that leading by example is more efficient than simply telling their children what to do. One parent stated, You must lead by example, alongside him [ . . . ] Be congruent with what you preach also. If you don’t adopt the same habits as him, you are not a good role model. (P7)
Parental Views of Their Role Toward Their Overweight Children.

Abbreviation: GEPEEP, Groupe Enjeux pour Parents d’Enfants avec Excès de Poids.
Number of parents who reported each role.
According to 4 participants, it appears that awareness or admitting the overweight or obesity of their children would be the starting point for every parent looking to improve their children’s healthy habits. Three participants mentioned that providing a healthful home environment, especially healthy food, is also important considering that parents are in charge of buying and preparing the food for their children. Parents must also educate their children to have a healthy lifestyle. To be more specific, this can be carried out by giving them instruction and information about healthy behaviors (n = 5) and followed-up by reinforcing and encouraging their children’s healthy choices (n = 7). Also, a few parents (n = 3) mentioned that beyond their educational role, they sometimes have to provide moral support for their children when they are going through psychosocial difficulties. Finally, it is important for parents (n = 6) to recognize their own limits and to seek for professional help when needed.
Parental Perceptions About the Role of Professionals
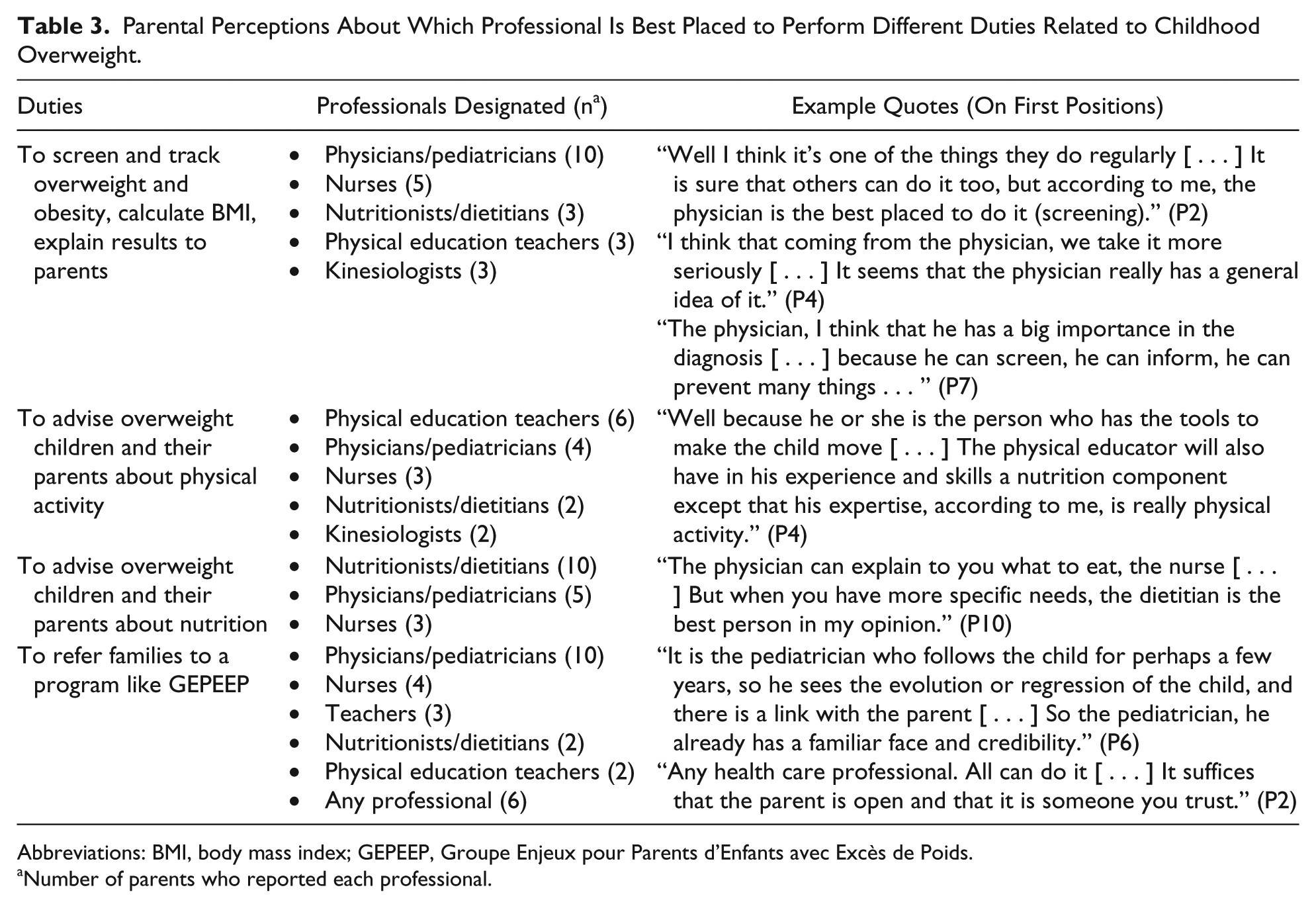
Table 3 summarizes parental perceptions regarding who (health professional or other) is best placed to perform different duties related to childhood overweight. The tasks included screening and tracking overweight and obesity, calculating BMI and explaining the results to parents, advising overweight children and their parents about physical activity and nutrition, and referring such families to a program like GEPEEP. The parents were also invited to share their views about who can play a role toward the overweight children and how everyone can be involved. Table 4 summarizes their answers.
Parental Perceptions About Which Professional Is Best Placed to Perform Different Duties Related to Childhood Overweight.
Abbreviations: BMI, body mass index; GEPEEP, Groupe Enjeux pour Parents d’Enfants avec Excès de Poids.
Number of parents who reported each professional.
Parental Perceptions About Professionals’ Role.

Abbreviations: BMI, body mass index; GEPEEP, Groupe Enjeux pour Parents d’Enfants avec Excès de Poids.
Number of parents who reported each professional. Only professionals named more than once are displayed.
In summary, all parents mentioned that physicians and pediatricians have a role to play toward overweight children. First of all, they were designated to do the screening and tracking of overweight or obesity, to take measurements, calculate BMI, and explain results to parents. Although many parents admitted that other professionals can also perform this task, the physicians and pediatricians are “the most appropriate” (P2) to do it. Participants explained that this is part of their duties in monitoring their patients’ health, that BMI is an indicator of the health of patients, and that they have the knowledge to interpret health risks. It appears that the message would be taken more seriously when coming from a physician: I think that coming from the physician, we take it more seriously. (P4) Parents will usually think: oops, now the physician told us . . . (P5)
Most parents (n = 9) believed that physicians and pediatricians were perceived as the most competent to refer families to a program like GEPEEP. However, 6 parents reported that any health professionals could perform this duty provided a bond of trust is established. Parents are unanimous about the relevance of nutritionists/dietitians and their role is well defined: to advise families about food. According to parents, it is a matter of expertise, skills, and knowledge. The physical education teacher came first to advise overweight youth and their families about physical activity. Participants explained that their training makes them competent to know how to get the children moving. Moreover, according to the parents, physical education teachers see the children at school on a regular basis. Other professionals such as nurses, psychologists, teachers, kinesiologists, and social workers were also considered by many parents to have a relevant role to play toward overweight children and their parents. Their roles as seen by the participants are reported in Table 4.
All parents felt that it was preferable that an overweight child was followed-up by a team rather than a single professional. They explained that having access to health care professionals with different specializations allows parents to get the tools they need (knowledge, information, and advice) to improve their children’s lifestyle, in addition to getting better service and solutions tailored for each family. Finally, 2 parents shared that being around peers in the same situation helped to motivate families.
Discussion
The main purpose of this study was to understand parents’ experience following their participation in the GEPEEP program and to obtain parental perceptions about stakeholders’ involvement in a multidisciplinary context to tackle childhood overweight. This section highlights the participants’ views in relation to the scientific literature on the same topic. Then, practical recommendations are offered to professionals dealing with overweight children and their parents. The study’s strengths and limitations are presented at the end of this section.
Participants’ Background
The fact that 9 out of 10 parents who agreed to participate in this study were mothers suggests that mothers feel more concerned than fathers by their children’s weight and health-related habits. When research related to children’s health requires parental participation, there is usually a higher response from the mothers. Indeed, in a systematic review on a related topic, maternal participation rated from 84% to 92%. 21 In the present study, parents have agreed to discuss the factors that led to their participation in the GEPEEP program. The majority indicated that the main reason was to better manage their children’s weight and also indicated that they were referred to the program by health professionals. It seems that communication about overweight children was carried out at a higher rate among participating families than in the general population, since 8 parents admitted that a doctor or pediatrician had already told them that their child was overweight. In general, less than a quarter of parents of overweight children receive this information from their doctor. 22 This suggests that better communication by practitioners could increase the number of families participating in programs like GEPEEP.
Parental Views of Their Role Toward Their Overweight Children
Parents see their role toward their overweight children as crucial. The roles or duties they described were grouped by themes, most of which can be found in the literature on parental roles, styles, influences, or practices. Thus, providing a healthy home environment, educating children about a healthy lifestyle, and reinforcing or encouraging the adoption and practice of these habits are roles that are well documented. 8 Modeling a healthy lifestyle is the role that was mentioned by most parents, which suggests that parents leading by example may have a better influence on young people’s health-related behavior compared with parents who do not practice what they teach. This phenomenon was also demonstrated by previous research. 10
Some parenting responsibilities emerged which, until now, had hardly been treated empirically. For example, participants emphasized the importance of being able to recognize and admit their child’s overweight. Since, according to previous studies, parents tend to underestimate the weight of their children, 23 this would be the starting point for anyone wanting to change the lifestyle and better manage the physical profile of their children. In another line of thought, some participants reported that they sometimes had to provide moral support to their children. Indeed, overweight children sometimes have psychological difficulties that may require moral support. 24 Finally, many parents stressed the importance of being able to benefit from professional help if necessary, by consulting specialists or by enrolling in an intervention program like GEPEEP.
Parental Perceptions About the Role of Professionals
This study provided information on parental perceptions of professionals who can play a role toward overweight children and their parents. It also provided their expectations about the responsibilities of stakeholders. Indeed, physicians have an important role in addressing the problem of overweight youth.12-15 They are the ones who have the most credibility in the eyes of parents. Their opinions and advice are taken seriously. Thus, they are designated to screen overweight and health problems, calculate BMI, and explain the results to parents. Although this task is recommended, 13 few practitioners carry it out consistently. 15 The results show that parents expect physicians to take care of it. Physicians and pediatricians are also at the top of the list for referring families to other resources (specialists or a program like GEPEEP). However, all professionals can refer families to a program like GEPEEP provided a bond of trust is established. Although doctors and pediatricians are able to provide advice about diet and physical activity, parents prefer to rely on specialists to help in this regard.
Nutritionists and/or dietitians were identified as experts to be consulted for advice on healthy eating while physical education teachers are those who can advise young people about physical activity. Although the interview guide was built so as to obtain health care professionals as the given response, several parents said that the school and school personnel can play an important role toward overweight youth. The school nurse and physical education teachers are the school personnel most likely to be involved in efforts to curtail the childhood overweight and obesity epidemic at the school level.17,25 Regarding nurses, participants indicated that they may support the efforts of doctors, performing some tasks that physicians do not always have time to do, in accordance with a recent study. 26 Psychologists can provide moral support to overweight children dealing with social or self-esteem problems. Social workers as well as parents can also provide psychological support. The relevance of psychologists’ involvement toward overweight children is already documented.15,16
Several stakeholders identified by the parents were part of the GEPEEP staff. We believe that having participated in the GEPEEP program and having consulted many professionals conferred on the participants a wealth of experience that allowed them to provide relevant answers to the research questions. Participants were also asked to explain their reasoning for the professionals and roles they mentioned. The explanations were related to the experience, skills, and expertise that each professional can contribute.
Last, all parents said it was preferable for overweight children to be monitored by a team of health professionals rather than by a single professional. This supports the wish of doctors to rely on the help of other professionals to address the problem of childhood overweight. 15 Parental mentions of the school nurse and the physical education teachers also suggest that there is a necessary link to build between the school and the health professionals. 25 Parents also feel that they should be part of the team.
Limitations of the Study
Like any case study, participants’ opinions are not necessarily generalizable to other parents. For example, their participation in the GEPEEP program probably contributed to deepen their understanding of childhood overweight and their knowledge of health professionals. Concerning the analysis of outcomes, it is possible that the researchers’ views and preconceptions have guided the categorization and the coding. To minimize this bias, this process was performed by 2 coders in parallel prior to the comparison. It is also possible that parents who enrolled in the program had a prior favorable bias toward such a program. For the same reason, parents not enrolled may not perceive that they can play a prominent role in their children’s weight management. 27 Furthermore, the overwhelming low proportion of father involved in the study may reflect the low capacity of such program to engage fathers, which seems a universal trend. 28
Conclusion and Recommendations for Action
Parental perceptions of their own role toward their overweight children showed that they feel important as agents of change for their children’s health and lifestyle. Several responsibilities have been previously identified in related literature were also relayed by our participants, such as providing a healthy environment and healthy food for their children, teaching them to have a healthy lifestyle, reinforcing their adoption and maintenance, and modeling a healthy lifestyle. Other parenting responsibilities have emerged such as awareness of the weight problem, offering psychological support, as well as seeking professional help if needed.
The fact that parents prefer a multidisciplinary approach should encourage practitioners to surround themselves with other professionals to monitor overweight children rather than trying to do it alone. Clinicians would benefit from working collaboratively rather than separately. Agencies wishing to develop an intervention program for overweight youth would also benefit from including professionals from several disciplines including education, which would be appreciated by parents.
Regarding professionals who can play a role in helping overweight youth and their families, parents identified physicians and pediatricians as primary care givers who can refer families to specialists or to programs like GEPEEP when needed. Nutritionists/dietitians, nurses, psychologists, kinesiologists or exercise specialist, and social workers are the other professionals mentioned by parents. Parents also recognized the contribution of teachers to educate young people about healthy lifestyles. Although many clinicians are reluctant to communicate with parents about their children’s weight status, parents have indicated that professionals can bring up the topic as long as a bond of trust is established.
Future research could investigate how health and education professionals see their role toward overweight children in a multidisciplinary environment, in order to compare their views with parents’ expectations. It could also be relevant to ask professionals working within a health care team about facilitators and barriers to effective collaboration.
Footnotes
Acknowledgements
The authors thank the GEPEEP program committee led by Ms Céline Raymond and the parents who volunteered to make this study possible.
Author Contributions
SB: Contributed to conception and design; contributed to acquisition, analysis, and interpretation; drafted manuscript; gave final approval; agrees to be accountable for all aspects of work ensuring integrity and accuracy.
JL: Contributed to conception and design; contributed to analysis and interpretation; critically revised manuscript; gave final approval; agrees to be accountable for all aspects of work ensuring integrity and accuracy.
FT: Contributed to conception and design; contributed to analysis and interpretation; critically revised manuscript; gave final approval; agrees to be accountable for all aspects of work ensuring integrity and accuracy.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.